Turp syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"TURP syndrome" transurethral resection hyponatremia
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is a full overview:
TURP Syndrome
Definition
TURP syndrome (transurethral resection of the prostate syndrome) is a potentially life-threatening complication of monopolar TURP characterized by symptomatic hyponatremia and intravascular volume overload caused by systemic absorption of large volumes of hypotonic, electrolyte-free irrigating fluid. It can occur as early as a few minutes into the procedure or as late as several hours after completion.
Pathophysiology
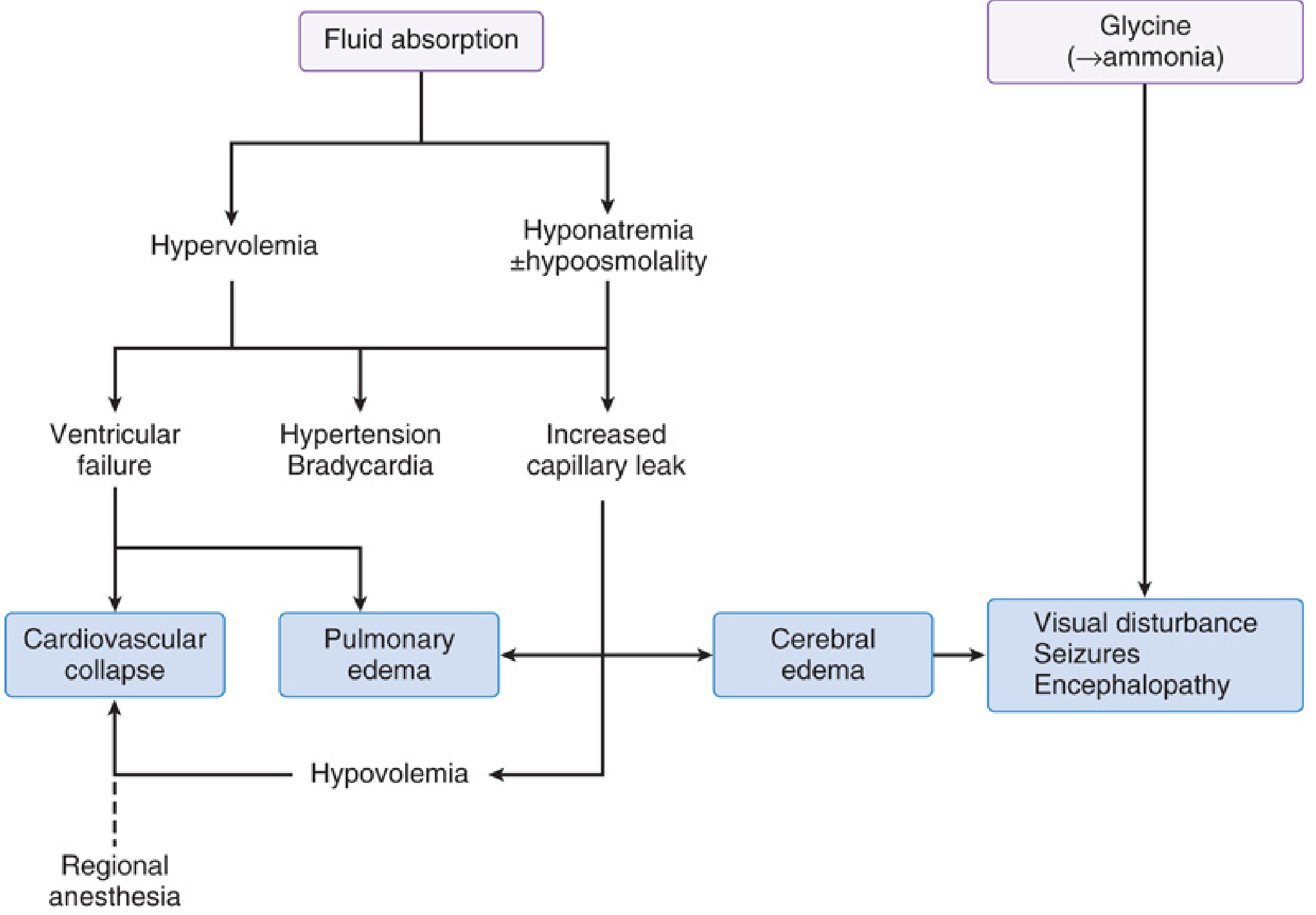
During monopolar TURP, the resectoscope opens prostatic venous sinuses. Because electrolyte solutions cannot be used (they disperse electrocautery current), hypotonic, non-electrolyte irrigants are required. These fluids are absorbed systemically, causing three overlapping problems:
1. Hypervolemia
- Absorbed fluid expands intravascular volume, leading to hypertension and reflex bradycardia initially
- Ventricular failure and pulmonary edema may follow, especially in patients with limited cardiac reserve
- Later, increased capillary leak causes hypovolemia, which can produce cardiovascular collapse - paradoxically, early hypertension can be followed by profound hypotension
2. Hyponatremia / Hypoosmolality
- All commonly used irrigants are hypotonic; their absorption dilutes serum sodium
- Neurological symptoms typically develop when serum Na⁺ falls below 120 mEq/L
- At Na⁺ <100 mEq/L, acute intravascular hemolysis can occur due to extreme hypotonicity
- Cerebral edema results, causing encephalopathy, seizures, and coma
3. Solute Toxicity
Specific to the irrigant used:
| Irrigant | Toxicity |
|---|---|
| Glycine 1.5% (most common) | Hyperglycemia, hyperammonemia (glycine degrades to ammonia), transient blindness (glycine is an inhibitory NT in the retina), seizures (allosteric NMDA activation) |
| Sorbitol 2.7% + mannitol 0.54% | Hyperglycemia (sorbitol), intravascular volume expansion (mannitol) |
| Distilled water | Severe hemolysis (rarely used now, restricted to bladder tumor resection) |
Irrigating Fluids Used in Monopolar TURP
| Solution | Osmolality |
|---|---|
| Glycine 1.5% | 230 mOsm/L |
| Sorbitol 2.7% + mannitol 0.54% | 195 mOsm/L |
| Sorbitol 3.3% | ~165 mOsm/L |
| Mannitol 3% | ~165 mOsm/L |
The absorption rate is 10-30 mL/minute of resection time. Procedures up to 2 hours can result in 6-8 L of absorbed fluid.
Risk Factors
- Prolonged resection time (>90 minutes significantly increases risk)
- Large prostate gland (>45 g)
- High irrigant bag/bottle height (increases intravesical pressure)
- Excessive bladder distension
- Extensive opening of venous sinuses
Incidence & Mortality
- Overall incidence of mild-to-moderate TURP syndrome: 0.78-1.4% of M-TURP procedures
- The syndrome may complicate 10-15% of TURP procedures (including subclinical cases)
- Mortality up to 25% has been reported for severe TURP syndrome (Na⁺ < 120 mEq/L)
-
- Miller's Anesthesia, 10e, p. 8471
Clinical Features
Onset can be intraoperative or postoperative (up to 24 hours later).
Neurological:
- Headache, restlessness, confusion
- Transient visual disturbances / blindness
- Seizures, coma
- Encephalopathy
Cardiovascular:
- Early: hypertension, bradycardia (from hypervolemia)
- Late: hypotension, cardiovascular collapse
- Arrhythmias
Respiratory:
- Dyspnea, cyanosis
- Pulmonary edema
Other:
- Nausea, vomiting
- Hemolysis (severe cases)
Diagnosis
- High clinical suspicion (especially in awake patient under regional anesthesia - symptoms not masked)
- Serum electrolytes (Na⁺, glucose), serum osmolality
- Arterial blood gas
- 12-lead ECG
The most sensitive monitoring approach is serum sodium measurement during and after surgery.
Treatment
Treatment is guided by severity of symptoms and serum sodium level:
| Severity | Serum Na⁺ | Treatment |
|---|---|---|
| Mild | >120 mEq/L | Fluid restriction + IV furosemide (loop diuretic) |
| Severe | <120 mEq/L | 3% hypertonic saline IV - correct carefully to avoid osmotic demyelination syndrome |
| Seizures | Any | Midazolam 2-4 mg IV; consider endotracheal intubation to prevent aspiration |
| Hypoxemia | Any | Supplemental O₂, ventilatory support |
| Cardiovascular | Any | Hemodynamic support |
Key principle: Correct Na⁺ no faster than 10-12 mEq/L per 24 hours to avoid central pontine myelinolysis.
Terminate surgery as rapidly as possible once TURP syndrome is suspected.
Tolvaptan (oral, 15 mg 2 hours pre-op) has been proposed as a preemptive measure in high-risk/prolonged cases - it is a selective V2 vasopressin receptor antagonist that promotes free water excretion.
Prevention
- Bipolar TURP - uses isotonic saline irrigation, essentially eliminates dilutional hyponatremia (though volume overload risk remains)
- Laser/plasma vaporization, microwave ablation, aquablation - all use physiologic saline
- Limit resection time (<90 min)
- Keep irrigant bag height low (reduce hydrostatic pressure)
- Regional (spinal/epidural) anesthesia is preferred - T10 level is sufficient; awake patients can report symptoms early, facilitating prompt diagnosis
- Use warmed irrigating fluids (prevents hypothermia)
Anesthetic Considerations
Regional anesthesia (spinal or epidural to T10) is preferred over general anesthesia for TURP because:
- The awake patient can report symptoms of TURP syndrome early
- May reduce postoperative venous thrombosis risk
- Large-database studies show lower 30-day mortality with neuraxial vs. general anesthesia (ACS-NSQIP, 28,486 patients, 2010-2016)
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 1303-1305 | Miller's Anesthesia, 10e, pp. 6372-6373 & 8471-8478
This is a shared conversation. Sign in to Orris to start your own chat.