Clinical approach to headache
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content to compile a thorough clinical approach to headache. Let me synthesize everything into a well-structured answer.
Clinical Approach to Headache
Overview
Headache is one of the most common complaints in clinical practice. The vast majority of patients have a benign primary headache disorder, but a small proportion have an underlying medical or surgical condition requiring prompt diagnosis. The clinical challenge is identifying the "needle in the haystack" — life-threatening causes hidden among the overwhelming majority of benign presentations — while avoiding the widespread overuse of imaging.
The brain parenchyma itself is insensitive to pain. Pain-sensitive structures include the meninges, cerebral arteries and veins, and tissues lining the skull cavities. Much headache pain, especially vascular and migrainous, is mediated through cranial nerve V (trigeminal), which may refer pain to areas not directly involved. — ROSEN's Emergency Medicine, p. 196
Classification
| Category | Examples |
|---|---|
| Primary | Migraine, tension-type, cluster headache, trigeminal autonomic cephalalgias |
| Secondary — benign | Post-traumatic, post-LP, cervicogenic, sinusitis, medication overuse |
| Secondary — emergent | SAH, ICH, meningitis/encephalitis, cerebral venous sinus thrombosis, cervical artery dissection |
| Secondary — critical/toxic | Carbon monoxide poisoning, temporal arteritis, acute angle-closure glaucoma, hypertensive emergency, preeclampsia, IIH |
Step 1: History — The Most Important Tool
Physical findings may be minimal even in serious headache, making the history the cornerstone of evaluation.
Key historical elements:
-
Onset and pattern — Rapid ("thunderclap") onset reaching maximum intensity within seconds to a minute is highly associated with SAH and other vascular causes. Recurrent headaches similar to prior episodes favor a primary disorder; a marked change in pattern signals a new or serious problem.
-
Severity and quality — "Worst headache of life" is a red flag even when examination is normal.
-
Associated symptoms
- Fever → meningitis, encephalitis, abscess
- Nausea/vomiting — nonspecific; present in migraine, raised ICP, glaucoma, and systemic illness
- Visual changes → glaucoma, IIH, posterior circulation stroke, temporal arteritis
- Focal neurological symptoms → hemorrhage, stroke, mass lesion
- Neck stiffness → meningitis, SAH
-
Onset triggers — Exertion, sexual activity, or Valsalva → coital/exertional headache or SAH
-
Context — Multiple household members affected simultaneously → carbon monoxide poisoning
Step 2: "Red Flags" (SNOOP4 Mnemonic)
| Feature | Possible Cause |
|---|---|
| Systemic signs (fever, weight loss, HIV, cancer) | Infection, malignancy, temporal arteritis |
| Neurological deficits (focal) | Mass lesion, hemorrhage, stroke |
| Onset sudden/thunderclap | SAH, RCVS, ICH |
| Older age (>50) new headache | Temporal arteritis, mass |
| Pattern change or progressive worsening | Mass, increasing ICP |
| Postural component | IIH, CSF leak, venous thrombosis |
| Precipitated by Valsalva/exertion/sex | SAH, coital/exertional headache |
| Papilledema | Raised ICP |
Red-flag features requiring urgent evaluation, per Bradley & Daroff's Neurology:
- New-onset severe headache with no significant headache history
- Progression of headaches — increasing frequency or severity
- Headache always localized to one area
- Headaches in a cancer patient
- Headache with fever, altered mental status, or focal neurological deficit — Bradley and Daroff's Neurology in Clinical Practice, p. 793
Step 3: Physical Examination
The examination focuses on:
- Mental status (altered → emergency)
- Fundoscopy — papilledema (raised ICP), subhyaloid hemorrhage (SAH)
- Meningeal signs — Kernig's, Brudzinski's, nuchal rigidity
- Cranial nerve examination — particularly CN II, III, IV, VI
- Vital signs — fever, hypertension
- Temporal artery — tenderness, thickening, or absent pulse (temporal arteritis)
Step 4: Differential Diagnosis by Urgency
Critical (life-threatening)
- Subarachnoid hemorrhage (SAH)
- Carotid/vertebral artery dissection
- Cerebral venous sinus thrombosis
- Carbon monoxide poisoning
- Temporal arteritis (risk of permanent visual loss)
Emergent
- Bacterial meningitis/encephalitis
- ICH / subdural / epidural hematoma
- Acute angle-closure glaucoma
- IIH with impending vision loss
- Mass lesion / traction headache
- Hypertensive emergency / preeclampsia
Non-emergent (primary)
- Tension-type headache
- Migraine (with or without aura)
- Cluster headache
- Post-traumatic headache
Risk factors for emergent causes (selected)
| Cause | Key Risk Factors |
|---|---|
| SAH | Sudden severe pain, exertion/sex trigger, "worst ever," family history, polycystic kidney disease, hypertension |
| Meningitis | Fever, immunocompromise, sinus/ear infection, age extremes, communal living |
| Temporal arteritis | Age >50, female sex (4:1), elevated ESR/CRP, jaw claudication |
| Carbon monoxide | Enclosed space, multiple household members, winter heating |
| Cerebral venous thrombosis | Female, pregnancy/OCP, prothrombotic state |
| Acute glaucoma | Age >30, pain in dark, prior history of glaucoma |
| IIH | Female, obesity, prior benign intracranial hypertension |
Step 5: The Ottawa SAH Rule
Apply to patients ≥15 years with non-traumatic headache reaching peak intensity within 1 hour.
Exclusions: New neurological deficit, prior aneurysm, prior SAH, known intracranial mass, chronic recurrent headaches.
If none of the following are present, SAH can be reasonably excluded:
- Age >40 years
- Neck pain or stiffness
- Witnessed loss of consciousness
- Onset during exertion
- Thunderclap onset (immediate peak pain)
- Limited neck flexion
High sensitivity, low specificity — use to reduce unnecessary testing, not as a standalone rule-out tool. — ROSEN's Emergency Medicine, p. 199
Step 6: Diagnostic Algorithm
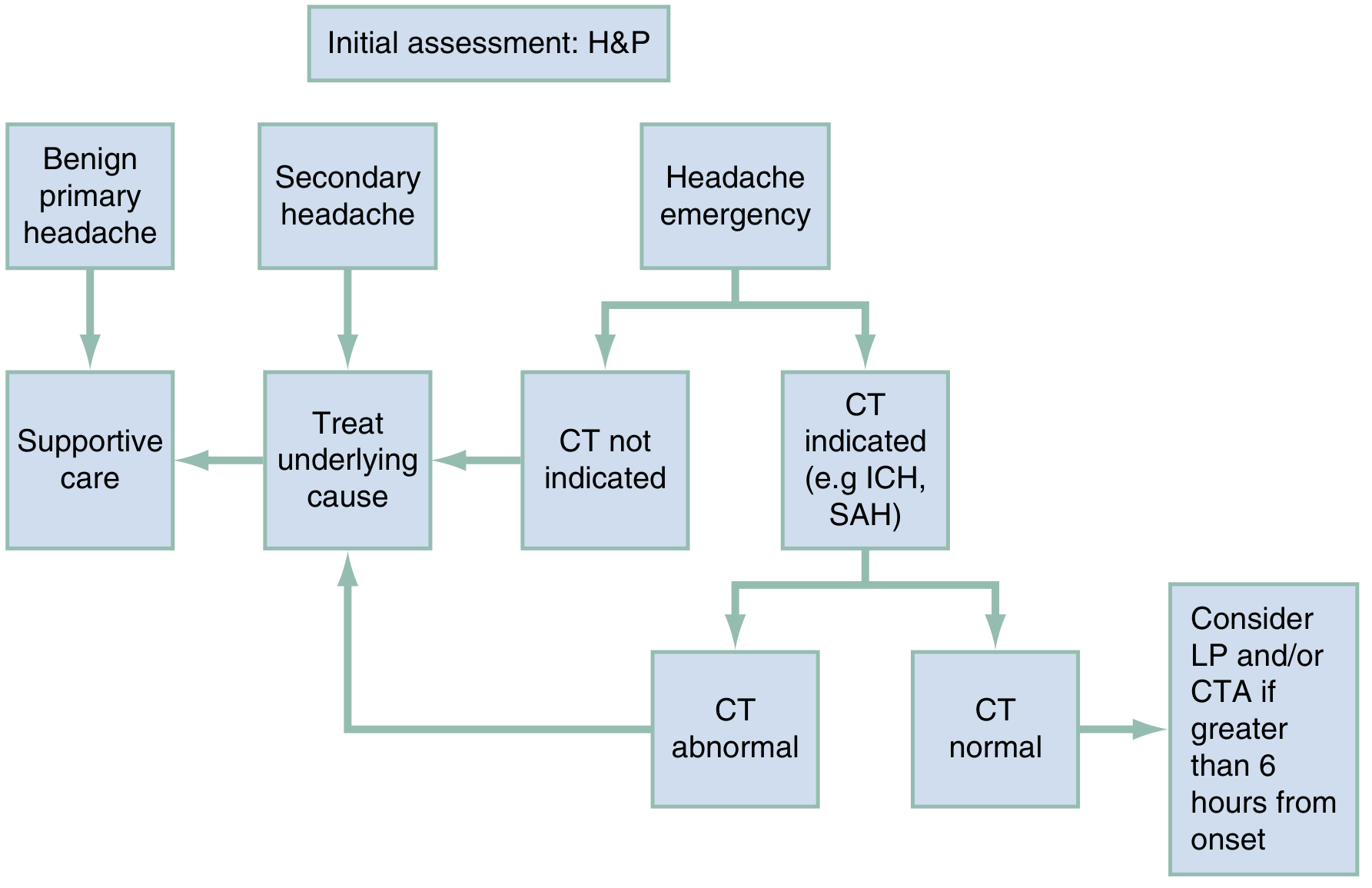
When NO red flags are present:
Symptomatic treatment without imaging is appropriate for clinically suspected primary headache (gradual onset, minor severity, no meningeal signs, normal neurology, normal fundoscopy).
When a specific etiology is suspected:
Directed testing is indicated (e.g., intraocular pressure for glaucoma, LP for meningitis).
For suspected SAH:
- Apply Ottawa SAH Rule
- CT within 6 hours of onset: high sensitivity (~99%) for SAH with a 3rd-generation scanner
- CT normal + >6 hours from onset: LP and/or CT angiography (CTA)
- LP findings in SAH: xanthochromia (CSF yellow discoloration), elevated RBCs that do not clear between tubes
Step 7: Investigations
| Test | Indication | Expected Finding |
|---|---|---|
| Non-contrast CT head | Suspected SAH, ICH, mass | Blood in subarachnoid/epidural/subdural space, mass, hydrocephalus |
| CT venogram / MR venogram | Suspected cerebral venous thrombosis | Filling defect in dural sinus |
| MRI brain (±gadolinium) | Posterior circulation stroke, mass, infection, IIH | Better than CT for posterior fossa |
| LP | SAH (>6 h), meningitis, IIH | Xanthochromia / RBCs; ↑WBC, ↓glucose, ↑protein; ↑opening pressure |
| ESR / CRP | Temporal arteritis | ESR >50 mm/h; elevated CRP |
| Intraocular pressure | Acute angle-closure glaucoma | Elevated IOP |
| CO-oximetry / carboxyhemoglobin | Carbon monoxide poisoning | Elevated COHb |
| ECG | SAH | Non-specific ST/T wave changes |
| CBC | Anemia-related headache | Severe anemia |
Most patients with headache do not require neuroimaging. Advanced imaging should be tailored to specific elements of the differential diagnosis, not used as a default. — ROSEN's Emergency Medicine, p. 199
Step 8: Management
Benign primary / non-specific headache
- Mild–moderate: NSAIDs (ibuprofen, naproxen), acetaminophen
- Moderate–severe migraine: Dopamine antagonists (metoclopramide, prochlorperazine IV/IM); triptans; ketorolac (IV/IM)
- Opioids: Not indicated for primary headaches
- Non-pharmacological: Rest, moist heat, massage, cognitive behavioral therapy, trigger avoidance
Specific emergent causes
| Cause | Initial Management |
|---|---|
| SAH | Neurosurgical consult, nimodipine, BP control, supportive care |
| Bacterial meningitis | Empirical antibiotics before LP if meningitis strongly suspected |
| Temporal arteritis | High-dose corticosteroids (prednisolone) immediately to prevent visual loss |
| CO poisoning | Remove from source, 100% high-flow O₂ |
| Acute glaucoma | Ophthalmology consult, IOP-lowering agents |
| ICH | BP control, neurosurgical consult, reversal of anticoagulation |
Summary: The Clinical Mindset
- Most headaches are benign — avoid reflexive CT scanning for every headache.
- A change in pattern is always suspicious — even in a known migraineur.
- Thunderclap = SAH until proven otherwise.
- Physical examination cannot exclude SAH — a normal neuro exam does not rule it out.
- Nausea/vomiting is nonspecific — present in migraine, raised ICP, glaucoma, and systemic illness alike.
- "CT before LP" for suspected mass — primarily because CT may give the diagnosis and render LP unnecessary, not because LP definitively causes herniation.
Sources:
- ROSEN's Emergency Medicine: Concepts and Clinical Practice — Headache chapter (Walker LE)
- Bradley and Daroff's Neurology in Clinical Practice — Imaging in headache
- Creasy & Resnik's Maternal-Fetal Medicine — Headache in pregnancy
This is a shared conversation. Sign in to Orris to start your own chat.