How best to taper estrogen and steroid after positive beta hcg following embryo transfer
estrogen progesterone luteal support taper IVF embryo transfer pregnancy
estrogen progesterone steroid taper after positive beta hCG IVF embryo transfer protocol 2024 2025
luteal phase support discontinuation IVF frozen embryo transfer
corticosteroid immunosuppression IVF embryo transfer taper pregnancy
progesterone supplementation duration IVF pregnancy first trimester
when to stop estradiol progesterone after IVF positive beta hCG tapering protocol guidelines 2025
https://pmc.ncbi.nlm.nih.gov/articles/PMC9580666
progesterone cessation IVF "luteal phase support" first trimester safety
corticosteroid prednisone dexamethasone taper after embryo transfer IVF pregnancy protocol steroid
corticosteroid prednisone IVF embryo transfer adjuvant outcome
Tapering Estrogen and Steroids After Positive Beta hCG Following Embryo Transfer
Understanding Why Luteal Support Is Needed
1. Progesterone Tapering
| Protocol | Common stopping point | Evidence |
|---|---|---|
| Fresh IVF (GnRH-antagonist) | Day of positive beta hCG, or up to 7 weeks | RCTs show comparable outcomes with early vs. late cessation |
| Frozen/HRT cycle FET | 8-10 weeks gestation (most common) | Observational and RCT data |
| Extended support (conservative approach) | Up to 12 weeks gestation | Used where miscarriage risk is high or CL absent |
- A PLOS ONE study of poor responders found no significant difference in outcomes between early progesterone cessation (at positive beta) vs. continuation to 9 weeks.
- A literature review (PMC9580666) found that ESHRE guidelines recommend progesterone "at least until the day of the pregnancy test." The same review notes that most contemporary clinicians continue to 8-10 weeks given the low risk profile of progesterone supplementation.
- Most clinics do NOT taper progesterone - they continue at the full prescribed dose until the chosen gestational week, then stop abruptly. The evidence does not support that gradual tapering is necessary for progesterone.
- If a conservative taper is preferred: reduce dose by ~25-33% every 1-2 weeks starting at 8 weeks, targeting complete cessation by 10-12 weeks.
- Some protocols stop abruptly at confirmation of fetal cardiac activity on ultrasound (typically 6-7 weeks).
2. Estrogen (Estradiol) Tapering
- Standard approach: Continue estrogen in parallel with progesterone and taper/stop simultaneously, usually at 8-10 weeks gestation.
- Tapering schedule: Estradiol is typically reduced more gradually than progesterone due to theoretical concerns about endometrial stability. A common approach:
- Week 8-9: Reduce dose by ~25-50%
- Week 9-10: Reduce by another 25-50%
- Week 10-12: Discontinue
3. Steroid (Corticosteroid) Tapering
- Recurrent implantation failure (RIF)
- Elevated NK cells or autoimmune profiles
- Thin endometrium protocols
- ASRM's immunotherapy guideline (2018) found "no clear evidence that peri-implantation glucocorticoids significantly improve clinical outcomes" in unselected populations, though benefit may exist in specific subgroups (e.g., positive ANA/antiphospholipid antibodies).
- A 2025 Cell Death Discovery review confirms continued heterogeneity in evidence for glucocorticoids in RIF.
| Steroid | Common stopping approach |
|---|---|
| Prednisolone 5-10 mg/day | Stop at 12-16 weeks, or taper over 2-4 weeks if on >4 weeks |
| Dexamethasone 0.5 mg/day | Usually given only peri-implantation (days -3 to +5 of transfer); if continued into pregnancy, stop by 8-10 weeks with a brief 1-2 week taper |
| Higher-dose steroids (e.g., for antiphospholipid syndrome or autoimmune conditions) | Taper more slowly, guided by underlying indication; do not stop abruptly if >3-4 weeks of use |
Summary Table
| Medication | Positive beta hCG action | Duration | Taper needed? |
|---|---|---|---|
| Progesterone (HRT-FET) | Continue at full dose | Until 8-10 weeks gestation | Not required; abrupt stop acceptable |
| Progesterone (fresh IVF with CL present) | May stop at positive beta or 6-7 weeks | Evidence supports early cessation if hCG rising | No |
| Estradiol (HRT-FET) | Continue | Until 8-10 weeks gestation | Gradual dose reduction over 2-4 weeks preferred |
| Prednisolone 5-10 mg (peri-implantation) | Continue per protocol | Stop by 10-12 weeks | Not required if short course (<4 weeks) |
| Dexamethasone 0.5 mg (peri-implantation) | Continue per protocol | Stop by 8-10 weeks | Brief 1-2 week taper if >4 weeks' use |
Clinical Pearls
- Never stop support based on symptoms alone. A "good feel" pregnancy or strong symptoms do not correlate with placental steroidogenesis.
- Monitor serum beta hCG every 48 hours until confidently rising (doubling appropriately), then confirm fetal cardiac activity at 6-7 weeks before considering any reduction.
- HRT cycles are unforgiving - the endometrium has no autonomous hormonal backup if you stop estrogen or progesterone prematurely.
- Individual clinic protocols differ significantly. The clinician running the cycle has context on the specific protocol used, embryo grade, and patient history - always defer to the protocol in use unless there's a clinical reason to diverge.
- Patients with a history of recurrent pregnancy loss, antiphospholipid syndrome, or thrombophilia may require extended support beyond 12 weeks; this should be managed in conjunction with maternal-fetal medicine.
How significant is an isolated finding of single umbilical artery on anomaly scan?
"single umbilical artery" isolated outcome perinatal
isolated single umbilical artery anomaly scan significance management guidelines 2024 2025
PMID: 34883005
https://www.mdpi.com/2077-0383/13/24/7749
"single umbilical artery" fetal growth restriction chromosomal anomaly surveillance
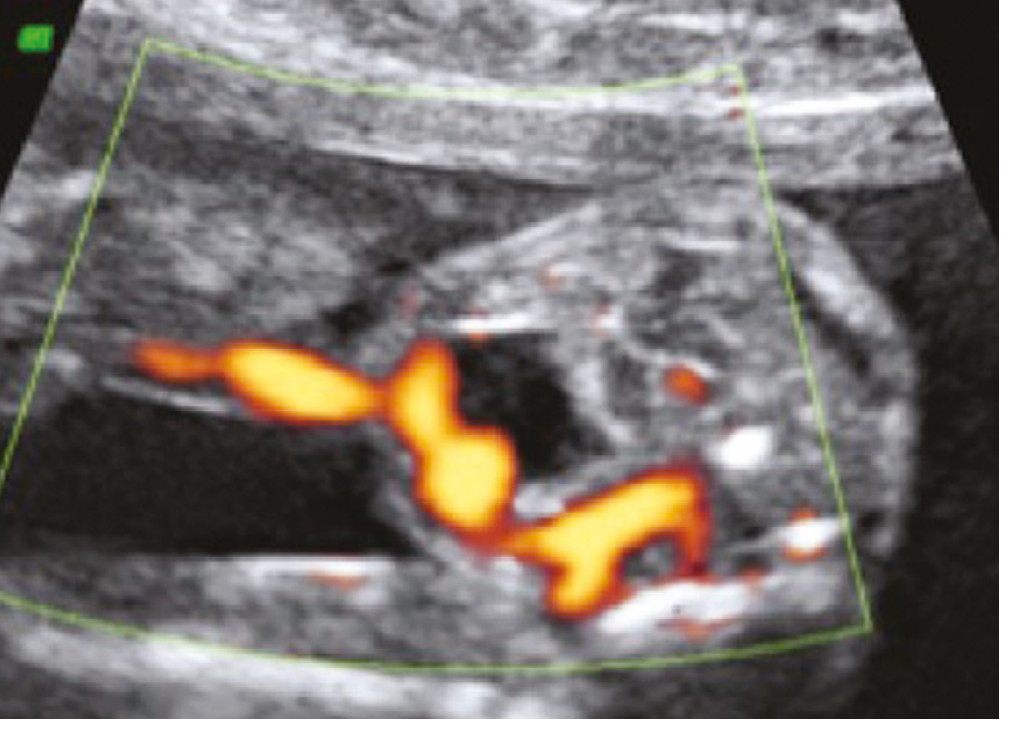
Single Umbilical Artery (SUA) on Anomaly Scan: Clinical Significance
What Is It?
How to Diagnose Correctly
Non-Isolated SUA: Significant Finding
- ~30% of all SUA cases have coexisting structural anomalies - cardiac, renal (most common), gastrointestinal (oesophageal/anal atresia), and vertebral defects.
- Among SUA fetuses with associated anomalies, chromosomal aneuploidy rates range from 5-50% (trisomy 18 and 21 are the most common).
- Invasive testing (amniocentesis for karyotype, chromosomal microarray) is clearly indicated when other anomalies are present.
Isolated SUA: Moderately Significant
| Adverse Outcome | Odds Ratio (95% CI) |
|---|---|
| Small for gestational age (SGA) | OR 2.90 (2.02-4.18) |
| Intrauterine death (IUD) | OR 2.62 (1.43-4.79) |
| Preterm birth | OR 2.48 (1.73-3.56) |
| Pregnancy-induced hypertension | OR 2.23 (1.41-3.54) |
| NICU admission | OR 2.28 (1.52-3.44) |
| Caesarean section | OR 1.64 (1.11-2.41) |
Management of Isolated SUA
At Time of Diagnosis (Anomaly Scan, ~18-22 weeks):
- Complete detailed anatomical survey - cardiac (including outflow tracts and three-vessel view), renal, GI, and limbs. Ideally by a fetal medicine specialist.
- Fetal echocardiogram - if the four-chamber view and outflow tracts were not adequately assessed during the anomaly scan, a formal echo is warranted.
- Invasive testing (amniocentesis/CVS) - NOT routinely indicated for isolated SUA. Chromosomal risk <1% does not justify routine amniocentesis. Offer only if:
- Additional anomalies found
- Soft markers present
- Patient requests after counselling
- Review prior biochemical screening (combined first-trimester or quadruple screen) - if low risk confirmed, this supports the isolated classification.
Third Trimester Surveillance:
- Serial growth scans starting at 28-32 weeks, typically every 4 weeks, to detect FGR early.
- Umbilical artery Doppler if FGR develops.
- Biophysical profile/CTG only if FGR or other complications arise - not routinely required in truly isolated SUA.
Delivery:
- No indication for routine early delivery in isolated SUA without FGR or other complications.
- Mode and timing of delivery determined by the presence of FGR or other anomalies.
- If structural anomalies are confirmed, plan delivery at a level III centre with NICU capability.
Postnatal:
- Examine newborn carefully for structural anomalies not detected prenatally.
- One study found a 60% excess of children who did not complete compulsory schooling in isolated SUA, suggesting possible neurodevelopmental associations - though this is not well-established and should not be communicated as a firm finding in counselling.
Counselling Summary
| Feature | Isolated SUA | SUA + Anomalies |
|---|---|---|
| Chromosomal risk | <1% | 5-50% |
| Structural anomalies | By definition absent | Common (cardiac, renal, GI) |
| FGR risk | ~2-3x increased | Higher still |
| Perinatal mortality | ~2.6x increased | Significantly higher |
| Invasive testing | Not routine | Indicated |
| Delivery planning | Standard unless complications develop | Level III centre |
How to practically prescribe HRT
practical prescribing HRT menopause estrogen progestogen regimens guidelines 2024 2025 NICE BMS
hormone replacement therapy menopause prescribing guidelines
https://cks.nice.org.uk/topics/menopause/prescribing-informa…
https://mot.southyorkshire.icb.nhs.uk/doncaster/files/Doncas…
HRT contraindications risks benefits breast cancer VTE cardiovascular 2024 NICE NG23
How to Practically Prescribe HRT
Step 1 - Establish the Indication
- Genitourinary syndrome of menopause (GSM) - vaginal dryness, dyspareunia, recurrent UTIs
- Prevention of osteoporosis (in women at high fracture risk who cannot use first-line agents)
- Premature ovarian insufficiency (POI) / surgical menopause at any age - HRT here is not optional, it is standard of care until at least age 51
- Mood disturbance, joint pains, poor sleep when clearly related to menopause
Step 2 - Assess for Contraindications
- Oestrogen-dependent cancer (breast, endometrial, ovarian) - current or recent
- Unexplained vaginal bleeding
- Active or recent venous thromboembolism (VTE) - note: transdermal route does not substantially raise VTE risk
- Active liver disease
- Uncontrolled hypertension
- Pregnancy
- History of hormone-induced VTE (e.g. pill-provoked DVT)
- Cardiovascular disease (coronary artery disease, stroke, TIA) - relative, consider with specialist input
- Strong family history or BRCA mutation
- Active gallbladder disease (oral oestrogen worsens; transdermal avoids this)
- Active migraine with aura (avoid oestrogen-containing combined oral contraceptive-type risks; transdermal preferred)
- High BMI, immobility, thrombophilia - if systemic HRT chosen, use transdermal route
Step 3 - Determine the Regimen Type
| Patient | Regimen |
|---|---|
| No uterus (hysterectomy) | Oestrogen-only HRT |
| Has uterus - perimenopause or <12 months amenorrhoea | Sequential (cyclical) combined HRT |
| Has uterus - postmenopause (>12 months amenorrhoea) | Continuous combined HRT |
| Post-endometrial ablation | Treat as having a uterus - add progestogen |
Step 4 - Choose the Oestrogen
| Route | Examples | Notes |
|---|---|---|
| Transdermal patch (preferred 1st line) | Evorel 25/50/75/100 mcg, Oestradot 25/37.5/50/75/100 mcg | Changed twice weekly. Avoids first-pass liver metabolism - lower VTE risk, safer in obesity, migraines, hypertension. Apply to abdomen or buttocks. |
| Transdermal gel | Oestrogel 0.06% (1 pump = 0.75 mg oestradiol), Sandrena sachets (0.5 mg or 1 mg) | Applied to thighs or arms, dry before dressing. Dose flexibility. |
| Transdermal spray | Lenzetto 1.53 mg/spray | 1-3 sprays daily. Quick-drying. |
| Oral | Ellest Solo 1 mg/2 mg tablets | 2nd line (higher VTE risk, more liver effects). Choose if patient preference or absorption issues with transdermal. |
- Standard: Evorel 50 mcg patch / Oestrogel 2 pumps / Sandrena 1 mg sachet / Lenzetto 2 sprays
- Low (perimenopausal, sensitive, elderly): Evorel 25 mcg / Oestrogel 1 pump / Sandrena 0.5 mg
- Higher (for POI, persisting symptoms): Evorel 75-100 mcg / Oestrogel 3-4 pumps / 3 sprays Lenzetto
Step 5 - Choose the Progestogen (Women With a Uterus)
- Progesterone taken for 12-14 days per cycle - this induces a withdrawal bleed
- Micronised progesterone 200 mg orally at bedtime for days 14-28 of cycle
- OR norethisterone 5 mg/day for 12 days/month (synthetic, less preferred due to breast cancer signal)
- OR medroxyprogesterone acetate 10 mg/day for 12 days/month
- OR dydrogesterone 10 mg/day for 12-14 days/month
- Progestogen taken every day alongside oestrogen - aim is amenorrhoea
- Micronised progesterone 100 mg at bedtime nightly (off-licence in UK at this dose but accepted by BMS)
- OR norethisterone 0.5-1 mg/day continuous
- Sequential: increase micronised progesterone to 300 mg for 12-14 days/cycle
- Continuous: increase micronised progesterone to 200 mg nightly
- Sequential: Evorel Sequi (2 weeks oestradiol-only patch, then 2 weeks oestradiol + norethisterone patch, changed twice weekly)
- Continuous combined: Evorel Conti (oestradiol 50 mcg + norethisterone 170 mcg/24h, changed twice weekly)
Step 6 - Local (Topical) Oestrogen for GSM
- Vaginal oestradiol: Vagifem/Vagirux pessaries 10 mcg (insert nightly for 2 weeks, then twice weekly ongoing)
- Vaginal cream: Ovestin cream (oestriol 0.1%)
- Vaginal ring: Estring 7.5 mcg/day - changed every 3 months
- Prasterone (Intrarosa): Intravaginal DHEA - converts locally to oestrogen and testosterone
Step 7 - Consider Testosterone
- Use Testogel 1% (male product, used off-licence): apply 1-3 cm (50-100 mg testosterone gel) to inner thigh daily - approximately 1/10th of the male dose
- AndroFeme 1% cream (licensed in Australia specifically for women): 0.5 mL (5 mg testosterone) daily
- Always ensure adequate systemic oestrogen is in place first
- Check testosterone level at baseline and 3-6 months. Aim for upper end of premenopausal female range (1-2.5 nmol/L)
Step 8 - The "Window of Opportunity" Concept
- Starting HRT within 10 years of menopause or before age 60 ("the window of opportunity"): net benefit - reduces cardiovascular risk, all-cause mortality reduced in women aged 50-59 on oestrogen alone (RR 0.79, WHI 20-year follow-up), no increased breast cancer risk in first 7 years
- Starting after age 60 or >10 years post-menopause (established atherosclerosis): cardiovascular risk may increase. Benefits still apply to symptoms and bones, but risk-benefit less favourable
- Premature menopause/POI: HRT is not optional - these women have significantly elevated cardiovascular, osteoporosis and cognitive risk if untreated
Step 9 - Risk Quantification for Breast Cancer Counselling
| Situation | Extra breast cancers per 1,000 women over 5 years |
|---|---|
| Oestrogen-only HRT | ~0 (may even reduce risk based on WHI 20-yr data) |
| Oestrogen + micronised progesterone | ~2-3 (lowest combined) |
| Oestrogen + synthetic progestogen | ~5-6 |
| BMI >30 | ~12 |
| Drinking 2 units alcohol/night | ~7 |
| No HRT baseline (age 50-59) | ~91 in 1,000 |
Step 10 - Follow-Up and Monitoring
- Symptom control assessment
- Side effects (breast tenderness, bloating, nausea from oral oestrogen; skin reactions from patches)
- Blood pressure check
- Unscheduled bleeding - normal within first 3-6 months on sequential HRT; needs investigation if heavy, prolonged, or persisting
- Expected within first 6 months - no action
- Investigate (USS ± hysteroscopy) if: persists beyond 6 months, bleeding is heavy/prolonged, 2+ minor risk factors for endometrial cancer, or 1 major risk factor
- Expected for first 3-6 months as endometrium atrophies
- Investigate if: persists beyond 6 months, amenorrhoea not achieved, new bleeding after amenorrhoea established
- Confirm indication still present
- Screen for new contraindications
- Breast awareness, mammography per national screening programme
- Update shared decision-making on continuing vs. stopping
- No arbitrary age limit for stopping - risks increase modestly after age 60 or after 10 years, but this does not mandate cessation
- Can be stopped abruptly or tapered - neither approach is clearly superior, but tapering reduces rebound symptoms
- There is no mandatory duration limit; duration is guided by ongoing indication and annual risk-benefit reassessment
Quick Reference Prescribing Summary
WOMAN WITH UTERUS - PERIMENOPAUSE:
Oestradiol transdermal (e.g. Evorel 50 mcg patch, twice weekly)
+ Micronised progesterone 200 mg at bedtime days 14-28 of cycle
→ Expect monthly withdrawal bleed
WOMAN WITH UTERUS - POSTMENOPAUSE:
Oestradiol transdermal (e.g. Evorel 50 mcg, twice weekly)
+ Micronised progesterone 100 mg at bedtime every night
OR + Mirena IUS (5-year use)
→ Aim for amenorrhoea (may take 3-6 months)
WOMAN WITHOUT UTERUS:
Oestradiol transdermal (e.g. Evorel 50/75 mcg)
- No progestogen needed
LOCAL SYMPTOMS ONLY (GSM):
Vagifem 10 mcg pessary (nightly x2 weeks, then twice weekly)
- No progestogen needed even with intact uterus
ADD TESTOSTERONE IF HSDD persists after adequate oestrogen:
Testogel 1% - 0.5-1.5 cm to inner thigh daily (off-licence)