Q. Discus the rationale and steps of radical neck dissection with suitable diagrams in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"neck dissection" AND "recent advances" AND head neck cancer
Finding Sources
Reading File
Searching PubMed
"neck dissection" AND "head and neck neoplasms"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching the Web
radical neck dissection steps technique RGUHS ENT surgery classification levels
Loading Image
Reading File
I now have comprehensive, detailed content from Cummings covering history, anatomy, classification, technique, complications, and recent advances. I have the key diagram. Now let me compile the comprehensive 50-mark answer.
Radical Neck Dissection - A Comprehensive 50-Mark Answer
Sources: Cummings Otolaryngology Head and Neck Surgery (6th Ed), Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Dhingra, Hazarika, and related recent literature
1. HISTORICAL BACKGROUND
The concept of radical en bloc resection of cervical lymphatics dates to the early 20th century. George W. Crile (1906) is credited with first systematically describing and reporting the efficacy of the radical neck dissection (RND). He postulated that head and neck cancer spread primarily via lymphatics rather than hematogenously, and described a block resection encompassing all cervical nodal groups from the mandible above to the clavicle below - the foundation of the modern RND.
- 1933 and 1941: Blair, Brown, and Hayes Martin popularized the RND and insisted categorically that the spinal accessory nerve (SAN), internal jugular vein (IJV), and sternocleidomastoid muscle (SCM) be sacrificed as part of every cervical lymphadenectomy.
- 1950s: Ward and Robben reported that the neck dissection could be modified by sparing the SAN, reducing postoperative shoulder drop.
- 1960s: Suárez in Argentina and Bocca and Pignataro independently described the "functional neck dissection" - removing all lymph node groups while preserving the SAN, SCM, and IJV - emphasizing that fascial compartments can be resected without sacrificing nonlymphatic structures.
- 1989-1994: Medina, Robbins, and Byers proposed formal classifications of neck dissection types.
- 2002: The American Academy of Otolaryngology - Head and Neck Surgery (AAOHNS) and the American Head and Neck Society (AHNS) published a standardized classification system based on cervical lymph node levels I-VI.
(Cummings Otolaryngology, Ch. 118, p. 2288)
2. SURGICAL ANATOMY AND LYMPH NODE LEVELS
The Six-Level System (Robbins/AHNS Classification)
The patterns of spread of cancer from various primary head and neck sites to the cervical lymph nodes have been documented through retrospective analyses of large neck dissection series. The nodal groups are categorized according to the level system originally described by the Memorial Sloan Kettering Group:
DIAGRAM: Cervical Lymph Node Levels I-VI
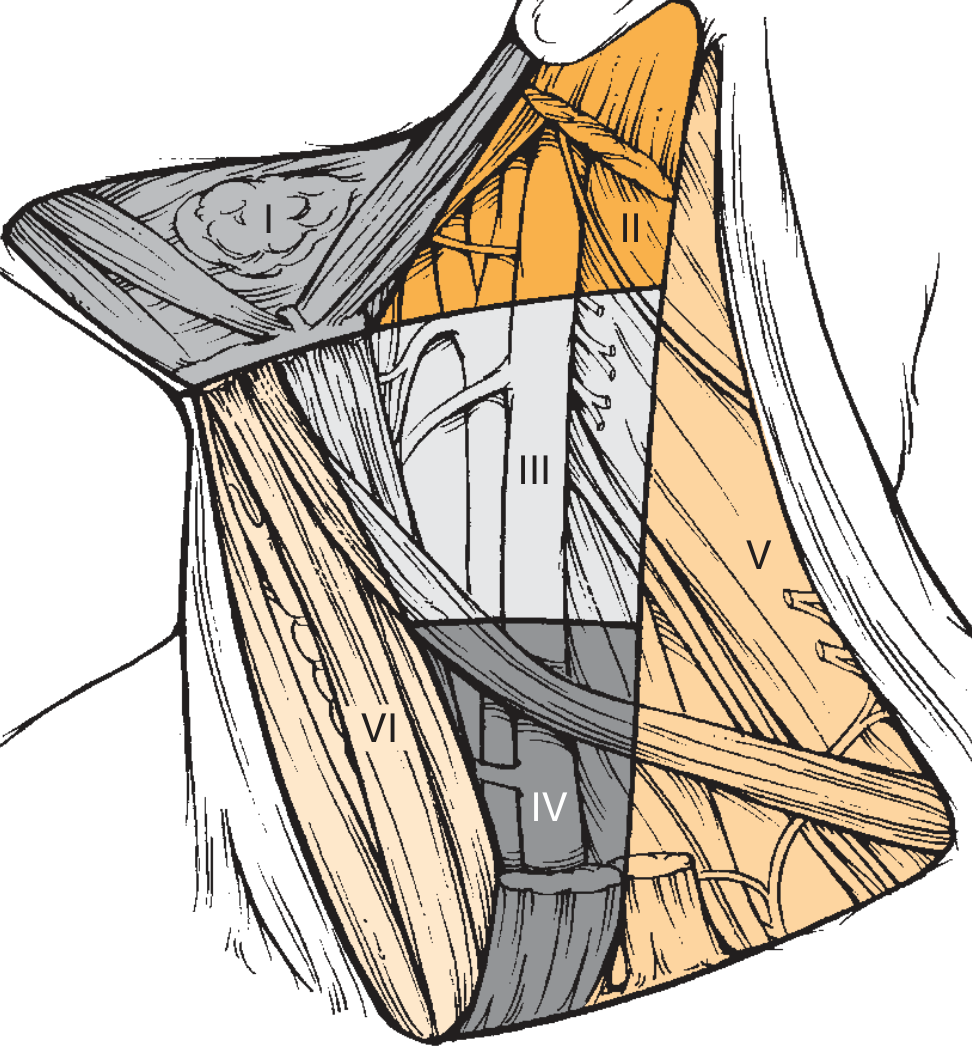
Fig. 118.1 - The six levels of the neck. Level I (submental and submandibular), Level II (upper jugular), Level III (middle jugular), Level IV (lower jugular), Level V (posterior triangle), Level VI (anterior compartment). Courtesy Cummings Otolaryngology, p. 2289.
| Level | Name | Boundaries | Key Structures |
|---|---|---|---|
| IA | Submental | Anterior bellies of both digastrics + hyoid | Midline structures (tip of tongue, floor of mouth, lower lip) |
| IB | Submandibular | Ant. & post. belly of digastric + body of mandible | Submandibular gland, facial vessels |
| IIA | Upper jugular (ant. to SAN) | Skull base to hyoid; medial to SCM | Oropharynx, oral cavity, nasopharynx, larynx |
| IIB | Upper jugular (post. to SAN) | Same as IIA, posterior to SAN | Nasopharynx, oropharynx primaries |
| III | Middle jugular | Hyoid to cricoid/omohyoid junction | Oral cavity, oropharynx, larynx, hypopharynx |
| IV | Lower jugular | Cricoid to clavicle | Larynx, hypopharynx, cervical esophagus, thyroid |
| VA | Posterior triangle (upper) | Trapezius, SCM, clavicle; above cricoid | Nasopharynx, oropharynx, cutaneous head |
| VB | Posterior triangle (lower) | Below cricoid | Thyroid, infraclavicular |
| VI | Anterior compartment | Hyoid to suprasternal notch, between carotid sheaths | Thyroid, subglottis, hypopharynx, cervical esophagus |
(Cummings, pp. 2288-2292)
Level VII (superior mediastinal nodes below the suprasternal notch) is included in some classifications, particularly for thyroid cancer.
3. CLASSIFICATION OF NECK DISSECTION
The AAO-HNS 2002 (updated AHNS) classification recognizes four types:
NECK DISSECTION CLASSIFICATION
|
┌──────┴──────────────────────┐
│ │
RADICAL NON-RADICAL
(Levels I-V + SCM + │
IJV + SAN) ┌───────────┼───────────┐
│ │ │
MODIFIED SELECTIVE EXTENDED
RADICAL (one or (removes
(I-V, spares more node additional
≥1 of SCM/ levels structures)
IJV/SAN) preserved)
Types in Detail:
1. Radical Neck Dissection (RND)
- Removes: Levels I-V + SCM + IJV + CN XI (SAN)
- Also removes: Tail of parotid gland, cutaneous branches of cervical plexus, submandibular gland, cervical fat and fascia
2. Modified Radical Neck Dissection (MRND)
- Removes: Levels I-V
- Preserves: One or more of SAN / IJV / SCM
- Type I: SAN preserved
- Type II: SAN + IJV preserved
- Type III (Functional Neck Dissection): SAN + IJV + SCM all preserved
3. Selective Neck Dissection (SND)
- Preserves: All three non-lymphatic structures (SAN, IJV, SCM)
- Removes: Only node levels at highest risk based on primary site
- Supraomohyoid (I-III): Oral cavity
- Lateral (II-IV): Larynx, hypopharynx, oropharynx
- Posterolateral (II-V): Thyroid, skin of posterior scalp
- Central (VI): Thyroid, subglottis
4. Extended Radical Neck Dissection
- RND + removal of one or more additional structures (carotid artery, parotid gland, overlying skin, hypoglossal nerve, vagus nerve, etc.)
(Cummings, p. 2293; AHNS Classification 2008)
4. RATIONALE FOR RADICAL NECK DISSECTION
Oncological Basis:
A. Lymphatic Spread Pattern
Head and neck carcinomas spread predictably via the cervical lymphatic system. The risk of occult nodal metastases for most UADT carcinomas exceeds 15-20%, justifying surgical clearance. Specific high-risk factors include:
- Perineural invasion
- Lymphovascular invasion
- Advanced T stage
- Certain subsites (e.g., pyriform sinus, base of tongue)
B. Extracapsular Spread (ECS)
ECS is the single most important adverse pathological feature after neck dissection:
- Macroscopic ECS: 44% recurrence rate (Carter et al.)
- Microscopic ECS: 25% recurrence rate
- Patients with 4+ positive nodes had dramatically worse 4-year survival
C. Block Resection Principle
The en bloc removal of all lymphatic tissue within its fascial compartments, originally championed by Crile, ensures adequate oncological clearance by:
- Removing all lymph nodes in potential drainage territory
- Clearing microscopic perilymphatic tumor deposits
- Preventing seeding during dissection
D. Indication for RND specifically
- Extensive lymph node metastases with extracapsular extension involving the SAN and IJV
- Tumor directly encasing or infiltrating the SCM, IJV, or SAN
- Cases where the nerve or vein cannot be safely separated from tumor (Cummings, p. 2293)
E. Therapeutic vs. Elective Neck Dissection
- Therapeutic (TND): Performed for palpable/radiologically detectable metastases in a patient with previously untreated cancer
- Elective (END): Performed when likelihood of microscopic lymphatic metastasis is significantly high AND reliable surveillance with salvage is not feasible
- Planned: 6-8 weeks after RT/CRT completion when probability of residual disease is high
- Salvage: Metastatic disease after previous treatment
5. PREOPERATIVE ASSESSMENT
PREOPERATIVE WORKUP FLOWCHART
│
Primary Site Assessment
│
┌────────┴────────┐
Clinical Radiological Histological
exam (CT, MRI, (Biopsy,
(N+/N0) PET-CT) FNAC)
│
Risk Stratification
│
┌────────┴──────────────┐
Low Risk High Risk
(<15-20%) (>15-20%)
│ │
Observation/RT Neck Dissection
Imaging:
- CT neck with contrast: Detects nodal metastases >10mm, ECS, vascular involvement
- MRI: Superior soft tissue definition
- PET-CT: Useful for post-chemoradiation assessment (reliable >3 months after CRT)
- Ultrasonography with FNAC: For accessible nodes
Fitness Assessment:
- Cardiorespiratory evaluation (IJV sacrifice may increase intracranial pressure if bilateral)
- Coagulation profile
- Thyroid function (level VI dissection)
6. STEPS OF RADICAL NECK DISSECTION
(Based on Cummings, Ch. 118, pp. 2293-2296; Scott-Brown's Vol 2; Dhingra Diseases of ENT)
STEP 1: POSITIONING
- Patient supine on the operating table
- A rolled towel/sandbag placed under the shoulders to extend the neck optimally
- Head turned to the contralateral side and supported on a donut
- Skin prepped and draped to expose:
- Both sides of the neck
- Lower face including the mentum
- Both mastoid processes and earlobes
- Clavicles and suprasternal notch inferiorly
STEP 2: INCISION PLANNING
The incision must provide:
- Optimal exposure of all lymph node levels (I-V)
- Preservation of maximal blood supply to flaps
- Broadly based flaps (superiorly or inferiorly)
- Avoidance of trifurcations overlying the carotid sheath
Standard incisions used:
INCISION OPTIONS FOR RND
A. HOCKEY STICK (most common for unilateral)
─── horizontal limb along skin crease ───
│
└── vertical limb down SCM
B. BOOMERANG / MODIFIED MacFEE
Parallel transverse incisions
C. McFEE INCISION
Two parallel horizontal incisions
(avoids trifurcation, better blood supply)
D. APRON INCISION
Bilateral hockey stick - for bilateral ND
E. SCHOBINGER INCISION
Y-shaped (trifurcation should not
overlie carotid sheath)
The hockey stick and boomerang patterns are preferred as they avoid trifurcations over the carotid sheath. The McFee incision (two parallel horizontal incisions) is particularly useful in previously irradiated necks due to superior blood supply to the skin flaps.
STEP 3: ELEVATION OF SKIN FLAPS
- Superior flap: Elevated superiorly to the level of the inferior border of the mandible and the mastoid process
- Inferior flap: Elevated inferiorly to the level of the clavicle
- Plane of dissection is deep to the platysma - care is taken to keep the platysma with the skin flap to protect the marginal mandibular branch of the facial nerve
- The external jugular vein is usually sacrificed during flap elevation
- Great auricular nerve is identified and may be sacrificed or preserved as needed
STEP 4: IDENTIFICATION AND LIGATION OF THE EXTERNAL JUGULAR VEIN
- The EJV is identified superficial to the SCM and ligated at its superior and inferior ends
STEP 5: DISSECTION OF LEVEL I (SUBMENTAL AND SUBMANDIBULAR TRIANGLE)
Submental triangle (Level IA):
- The submental fat pad containing nodes is dissected off the mylohyoid muscle
- Anterior bellies of both digastric muscles define the boundaries
Submandibular triangle (Level IB):
- The marginal mandibular branch of CN VII is identified as it crosses the facial artery and vein at the inferior border of the mandible - it is carefully preserved by ligating and dividing the facial vessels below the nerve
- The submandibular gland (SG) is dissected in a subcapsular plane off the mandible
- The lingual nerve (CN V3) and submandibular duct (Wharton's duct) are identified anteriorly
- The submandibular duct is divided and ligated close to the mouth floor
- The submandibular ganglion is divided, allowing the lingual nerve to retract superiorly
- The hypoglossal nerve (CN XII) and its venae comitantes are protected in the deep portion
- The facial artery is ligated proximally as it exits deep to the SG
- Complete excision of all contents within the muscular boundaries of the submandibular triangle is required
STEP 6: DIVISION OF STERNOCLEIDOMASTOID MUSCLE (SCM)
- The SCM is divided at its mastoid and occipital insertions superiorly
- It is also divided from the sternal and clavicular origins inferiorly
- This exposes the underlying carotid sheath and the contents of the posterior triangle
STEP 7: LIGATION AND DIVISION OF INTERNAL JUGULAR VEIN (IJV)
- The carotid sheath is opened
- The IJV is ligated and divided at its inferior end (just above the clavicle) first
- Double ligation with non-absorbable sutures (silk 2-0) or vascular clips
- The thoracic duct on the left (or right lymphatic duct on the right) must be identified and ligated to prevent chylous fistula
- The IJV is then ligated and divided superiorly (just below the skull base / jugular foramen)
- The vagus nerve (CN X) within the carotid sheath is identified and preserved
- The common/internal carotid artery is kept intact and protected throughout
STEP 8: CLEARANCE OF THE POSTERIOR TRIANGLE (LEVELS IIB, III, IV, V)
- The Spinal Accessory Nerve (SAN, CN XI) is identified:
- Below the jugular foramen: lies deep to digastric and stylohyoid, lateral/immediately posterior to the IJV
- Runs obliquely downward and posteriorly to reach the medial surface of SCM at the junction of the superior and middle thirds
- In RND, the SAN is sacrificed at its entry into the SCM
- The contents of the posterior triangle are swept anteriorly off the floor muscles:
- Floor muscles: levator scapulae, splenius capitis, scalenus medius
- The phrenic nerve (C3,4,5) on the anterior surface of scalenus anterior is identified and preserved
- Brachial plexus roots are also protected
- The transverse cervical artery and vein are divided
- The omohyoid muscle is divided at its intermediate tendon
- Level V (posterior triangle) nodes along the SAN and transverse cervical vessels are cleared
STEP 9: DISSECTION OF LEVELS II, III, AND IV (JUGULAR CHAIN)
- With the SCM and IJV now divided, the jugular nodal chain is elevated en bloc
- Dissection proceeds from inferior to superior (or superior to inferior depending on surgeon preference)
- The hypoglossal nerve is identified crossing the great vessels at level II/III junction and preserved
- The contents are swept off the carotid vessels and vagus nerve
- The IJV, SCM, SAN, and all nodal tissue are delivered as one specimen
STEP 10: DIVISION OF IJV SUPERIORLY AND SPECIMEN REMOVAL
- Superior ligation of the IJV just below the skull base
- The en bloc specimen containing levels I-V, SCM, IJV, and SAN is removed
- The specimen is oriented and labeled for the pathologist
STEP 11: HEMOSTASIS AND WOUND CLOSURE
- Meticulous hemostasis using bipolar cautery and ties
- Neck drains (suction - Redivac type, 2 drains):
- Inserted through separate stab incisions at the most dependent areas of dead space
- Drain the anterior and posterior dead spaces separately
- The wound is closed in two layers:
- First: Platysma (anteriorly) and subcutaneous tissue (laterally)
- Second: Skin (with interrupted/subcuticular sutures or staples)
- Compressive dressing is applied
7. STRUCTURES REMOVED IN RND
STRUCTURES REMOVED IN RADICAL NECK DISSECTION
Lymphatic: ────── Levels I, II, III, IV, V
────── Submandibular gland
────── Tail of parotid gland
Non-lymphatic: ────── SCM (sternocleidomastoid muscle)
────── IJV (internal jugular vein)
────── SAN (CN XI / spinal accessory nerve)
────── EJV (external jugular vein)
────── Omohyoid muscle (intermediate tendon)
────── Cutaneous cervical plexus branches
Structures NOT Removed in Standard RND:
- Postauricular and suboccipital nodes
- Periparotid nodes (except tail)
- Perifacial and buccinator nodes (Nodes of Stahr)
- Retropharyngeal nodes
- Paratracheal nodes
(Cummings, p. 2293)
8. VARIATIONS IN APPROACH
"Variations in the approach to the RND should be made depending on the location of the disease and its degree of mobility. It is best to mobilize the areas that are least involved with tumor first, enhancing exposure of anatomic structures that may be directly invaded."
- Cummings, p. 2296
9. RESULTS AND ONCOLOGICAL OUTCOMES
| Scenario | Recurrence Rate |
|---|---|
| RND for pathologically node-negative (historical) | 3-7% |
| Therapeutic RND, macroscopic ECS | 44% |
| Therapeutic RND, microscopic ECS | 25% |
| Positive nodes in 1 level | 36.5% recurrence |
| Positive nodes in multiple levels | 71% recurrence |
| Modified RND (nerve-sparing), therapeutic | 0-20% |
The use of adjuvant radiotherapy is widely accepted to improve neck control rates after neck dissection, particularly with ECS or multiple positive nodes. (Cummings, p. 2297)
10. COMPLICATIONS OF NECK DISSECTION
(Cummings, Ch. 118, "Complications of Neck Dissection", p. 1718)
COMPLICATIONS OF NECK DISSECTION
INTRAOPERATIVE POST-OPERATIVE
───────────── ──────────────
• Hemorrhage EARLY:
• Air embolism • Hematoma / Seroma
• Injury to CN XII • Wound infection / dehiscence
• Injury to CN X (vagus) • Chylous fistula (esp. left side)
• Injury to phrenic nerve • Carotid artery rupture
• Carotid artery injury • Facial/cerebral edema (bilateral IJV sacrifice)
• Brachial plexus injury • Air leak
• Thoracic duct injury • Blindness (raised ICP)
• Pneumothorax • Pneumothorax / bilateral chylothorax
LATE:
• Shoulder syndrome (SAN sacrifice)
- Shoulder drop, pain, restricted abduction
• Horner's syndrome (sympathetic chain)
• Trismus
• Hypertrophic scar / keloid
• Lymphedema
• Frey's syndrome (chorda tympani injury)
• Hypothyroidism (parathyroid injury)
Shoulder Syndrome (Most Significant Morbidity of RND):
- Results from SAN sacrifice
- Features: Shoulder droop, pain, restricted abduction above 90°, winging of scapula, trapezius wasting
- Prospective studies (Sobol, 1985; Remmler et al.): RND causes major, permanent trapezius EMG dysfunction, while nerve-sparing procedures show recovery by 12 months
- Justifies the preference for MRND/SND when oncologically safe
Chylous Fistula:
- Results from thoracic duct injury during dissection at the left neck base (level IV)
- Recognized by milky fluid in drain post-feeding
- Management: NPO, medium-chain triglyceride diet, pressure dressing; if persistent > 2 weeks, re-exploration
11. SHOULDER REHABILITATION AFTER RND
Post-RND shoulder physiotherapy includes:
- Passive range-of-motion exercises from postoperative day 1
- Progressive active exercises
- Scapular stabilization exercises
- Referral to physiotherapy is mandatory for all patients
12. RECENT ADVANCES
(Based on Cummings, Scott-Brown, and PubMed evidence)
A. Sentinel Node Biopsy (SNB)
- Technique: Injection of radiotracer (Tc-99m sulfur colloid) and/or blue dye around the primary tumor
- Lymphoscintigraphy identifies the first-echelon draining node
- Under evaluation for oral cavity cancers (T1/T2 N0)
- Systematic review evidence supports selective approaches in salivary gland malignancies
B. Minimally Invasive / Endoscopic Neck Dissection
- Endoscopically assisted neck dissection has been demonstrated as feasible
- Takes approximately 1 hour longer than open technique on average
- No significant difference in lymph node yield or complications compared to open approach
- Useful for minimizing wound morbidity in selected patients (Cummings, p. 1718)
C. Robotic Neck Dissection (RAMND)
- Robot-Assisted Modified Neck Dissection (RAMND) via retroauricular or transaxillary approach
- Chan et al. (2024) systematic review (PMID: 38777980): Current robotic applications in head and neck surgery include neck dissection, with comparable nodal yield to open surgery
- Advantages: Better cosmesis, magnification, instrument precision
- Limited to selective and modified radical neck dissections in current practice
D. PET-CT-Guided Decision Making
- Post-CRT PET-CT assessment at 3 months to guide decision for planned neck dissection
- Studies show PET-CT surveillance is cost-effective compared to planned neck dissection for post-radiotherapy necks
- PET at 3 months post-CRT has high negative predictive value for residual disease
E. De-Escalation in HPV-Positive Oropharyngeal Cancers
- HPV-positive (p16+) oropharyngeal SCC has a dramatically better prognosis
- Ongoing trials exploring neck management de-escalation (fewer levels, less radical dissections)
- Transoral robotic surgery (TORS) with upfront staged neck dissection is increasingly preferred
F. AHNS Classification Updates
The AHNS Neck Dissection Committee has continued to refine classification systems to enable modular, accurate reporting across different tumor types and management courses, improving communication between institutions and countries. (Cummings, p. 2293)
13. DRAINAGE PATTERN BY PRIMARY SITE (FLOWCHART)
PRIMARY SITE → LEVELS AT RISK → RECOMMENDED SND
─────────────────────────────────────────────────
Oral Cavity → I, II, III → Supraomohyoid (I-III)
Oropharynx → II, III, IV (±I) → Lateral (II-IV) or I-IV
Hypopharynx → II, III, IV, VI → Lateral (II-IV) ± VI
Larynx → II, III, IV, VI → Lateral (II-IV) ± VI
Nasopharynx → II, III, IV, V → Lateral (II-V)
Thyroid → VI, IV, III → Central (VI) ± lateral
Parotid → II, III ± I, V → Selective
14. CONTRAINDICATIONS TO RND
Absolute:
- Unresectable distant metastases (M1)
- Unresectable primary tumor with no palliative benefit
- Patient unfit for general anesthesia
Relative:
- Fixed nodes involving the carotid artery bilaterally
- Bilateral IJV involvement (severe risk of facial edema/raised ICP)
- Previous radical contralateral neck dissection
15. SUMMARY TABLE: COMPARISON OF NECK DISSECTION TYPES
| Type | Levels | SCM | IJV | CN XI | Indication |
|---|---|---|---|---|---|
| RND | I-V | Removed | Removed | Removed | ECS involving SAN/IJV |
| MRND Type I | I-V | Removed | Removed | Preserved | Grossly visible nodes, nerve free |
| MRND Type II | I-V | Removed | Preserved | Preserved | Multiple levels without vascular invasion |
| MRND Type III (FND) | I-V | Preserved | Preserved | Preserved | N0/N+ nodes without nonlymphatic invasion |
| SND (I-III) | I-III | Preserved | Preserved | Preserved | Oral cavity N0 |
| SND (II-IV) | II-IV | Preserved | Preserved | Preserved | Larynx, oropharynx N0 |
| Extended RND | I-V + extra | + extra | + extra | + extra | Carotid/skin/nerve invasion |
16. KEY TAKEAWAYS FOR RGUHS EXAMINATION
- Definition of RND: En bloc removal of levels I-V + SCM + IJV + CN XI ipsilaterally, from inferior border of mandible to clavicle, from contralateral anterior belly of digastric/lateral strap muscles to anterior border of trapezius
- Crile (1906) is the father of RND; Bocca described functional (nerve/vessel-sparing) neck dissection
- Rationale: Predictable lymphatic drainage patterns, >15-20% occult metastasis risk, ECS as key prognostic indicator
- Incisions: Hockey stick, McFee, boomerang - avoid trifurcations over carotid sheath
- Key steps: Positioning → incision → flap elevation → level I dissection → SCM division → IJV ligation → posterior triangle clearance → en bloc removal → drain placement → two-layer closure
- Most important complication: Shoulder syndrome (SAN sacrifice) - requiring mandatory physiotherapy
- Chylous fistula: Left-side neck, thoracic duct injury, milky drain fluid post-feed
- Recent trend: RND is now rarely performed; MRND and SND have replaced it in most clinical scenarios because they reduce morbidity without compromising oncological control
- PET-CT is the recommended imaging modality post-CRT (at 3 months)
- Robotic/endoscopic approaches represent the frontier of minimally invasive neck dissection
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery (6th Ed.), Ch. 118 - Ronen O, Samant S, Robbins KT, pp. 2286-2312
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (8th Ed.), Vols 1 & 2 - Neck Dissection chapters
- Dhingra PL - Diseases of Ear, Nose and Throat, Ch. on Neck Dissection
- Hazarika P - Textbook of ENT and Head & Neck Surgery
- Zakir Hussain - Clinical ENT
- Stell and Maran's Head and Neck Surgery - Neck dissection sections
- Chan PLC et al. "Robotic Surgery for Head and Neck Tumors." Curr Oncol Rep 2024 Jul. [PMID: 38777980]
- Chia C, Key S, Hasan Z. "Systematic review of cervical metastases in oral maxillary SCC." Cancer Rep 2021. [PMID: 33963809]
- AHNS Classification System, 2008 (updated 2019)
RGUHS Exam Tip: For a 50-mark answer, always include: (a) historical background with Crile, (b) anatomy + level diagram, (c) classification table, (d) rationale/indications, (e) detailed numbered steps of the operation, (f) structures removed, (g) complications table, and (h) recent advances including robotic/endoscopic approaches and de-escalation trends. The shoulder syndrome and chylous fistula are the most commonly examined complications.
This is a shared conversation. Sign in to Orris to start your own chat.