Double sequential defibrillator
Reading File
Searching PubMed
double sequential defibrillation refractory ventricular fibrillation
Finding Sources
Reading Article
PMID: 37482919
Reading Article
PMID: 39127020
Reading File
Reading Article
PMID: 38522736
Reading File
Finding Sources
Loading Image
Here is a complete overview of double sequential defibrillation (DSED).
Double Sequential Defibrillation (DSED)
What It Is
Double sequential defibrillation - also called dual sequential external defibrillation (DSED) - is a rescue technique that uses two separate defibrillators with two sets of pads to deliver two rapid successive shocks in patients with shock-refractory ventricular fibrillation (VF). The goal is to dramatically increase total delivered energy and overcome the failure of standard single-shock defibrillation.
- Tintinalli's Emergency Medicine, p. 198 & 202
- Braunwald's Heart Disease, p. 3341
Indication
DSED is considered for shock-refractory VF, defined as:
- VF persisting despite 3 or more successive standard shocks, plus adequate CPR and antiarrhythmic drugs (epinephrine, amiodarone, or lidocaine)
- Some definitions also include: 3+ sustained episodes of VT/VF or ICD shocks within 24 hours
It is a last-resort escalation, not a first-line strategy.
Technique
- Standard pad position (anterior-lateral): first defibrillator pads placed in the usual apex-sternum orientation.
- Second pad position (anterior-posterior): second defibrillator pads placed anteriorly and posteriorly - creating two orthogonal shock vectors.
- Both defibrillators are charged to maximal output simultaneously.
- Shocks are delivered in rapid succession (nearly simultaneously), requiring coordination between two operators.
The anterior-posterior second pad placement ensures that the two electrical vectors traverse different myocardial territories, theoretically depolarizing a larger total mass of fibrillating myocardium.
Proposed Mechanism
The exact mechanism is debated. Leading theories include:
- Reduced VF threshold: the combined energy lowers the threshold needed to terminate VF
- Overriding the relative refractory period: the second shock finds previously refractory myocardium now excitable, completing depolarization of the entire ventricular mass
- Increased current through untreated fibrillating tissue: the orthogonal vectors cover myocardial regions missed by a single vector
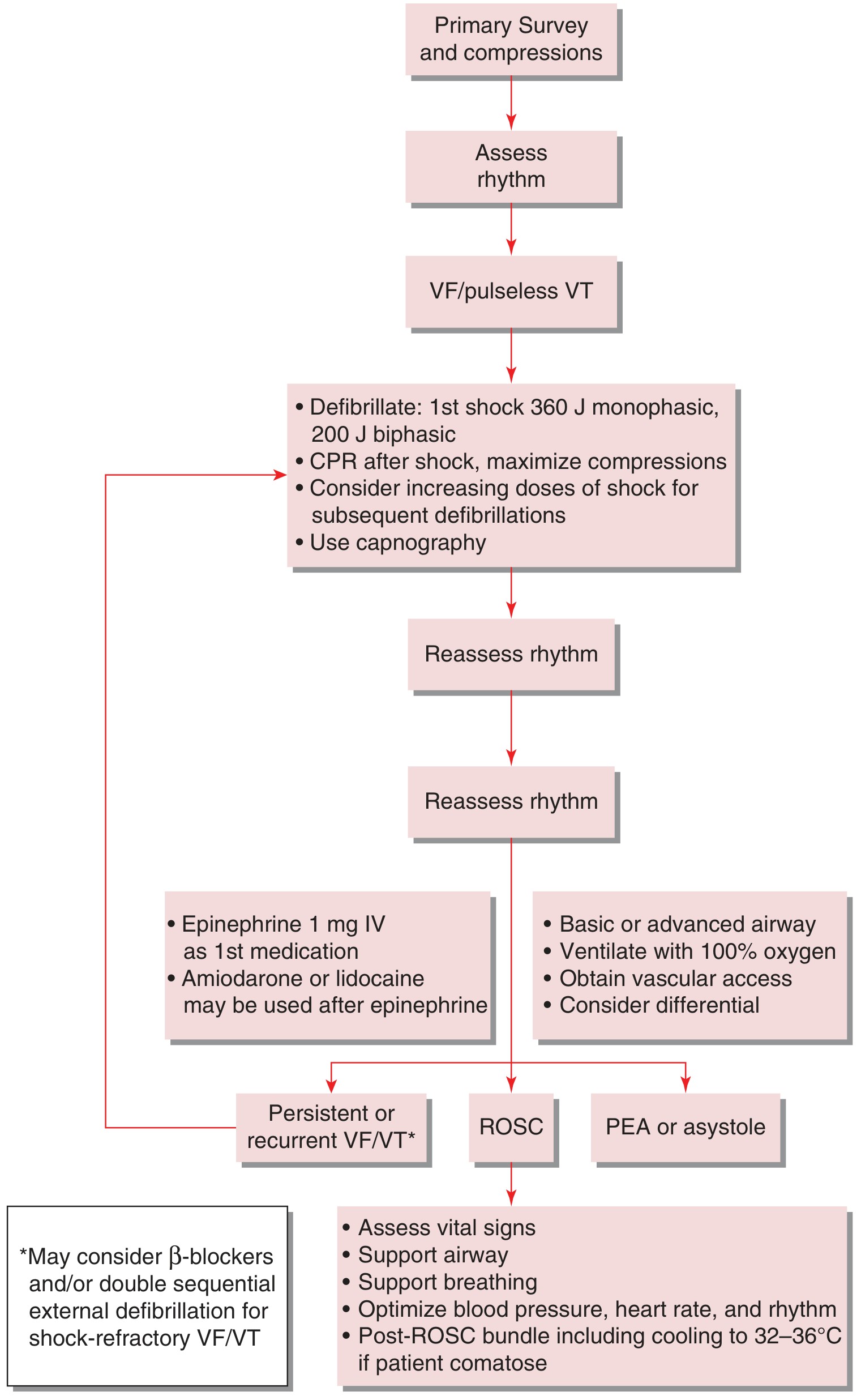
VF/pulseless VT Management Algorithm
The flowchart below (from Tintinalli's) shows where DSED fits - as a consideration at the "persistent or recurrent VF/VT" branch, alongside beta-blockers:
Clinical Evidence
DOSE VF Trial (the key RCT)
The DOSE VF cluster RCT (Cheskes et al.) is the landmark trial. A 2024 secondary analysis (PMID 38522736) of 345 patients found:
- DSED was superior to standard defibrillation for survival, ROSC, and neurologically favorable outcome
- The benefit applied to both shock-refractory VF (0% vs 28.6% survival, p=0.041) and recurrent VF
- Vector-change (VC) defibrillation improved VF termination but was not superior for survival or ROSC
Recent Systematic Reviews and Meta-analyses
Two high-quality meta-analyses published 2023-2024 reached more cautious conclusions:
| Study | Finding |
|---|---|
| Abuelazm et al., 2023 - network meta-analysis, 7 studies, n=1632 (PMID 37482919) | DSED not significantly superior to standard defibrillation for survival, ROSC, or neurological outcome - evidence still inconclusive |
| Yu et al., 2024 - meta-analysis, 6 trials, n=1360 (PMID 39127020) | The single RCT favored DSED, but pooled cohort studies showed no benefit. Double simultaneous (not sequential) defibrillation was associated with lower ROSC rates - caution advised |
Bottom line from evidence: The DOSE VF RCT supports DSED benefit, but pooled observational data do not. An important distinction is that simultaneous double defibrillation appears potentially harmful - the "sequential" (rapid succession, not true simultaneous) approach is preferred.
DSED vs. Vector-Change Defibrillation
These are two distinct strategies often studied together:
| Feature | DSED | Vector-Change (VC) |
|---|---|---|
| Equipment | Two defibrillators | One defibrillator |
| Mechanism | Higher total energy, dual vector | New current vector through previously resistant tissue |
| Evidence | Best data from DOSE VF RCT | Good for VF termination, less clear for survival |
| Complexity | Higher (requires two operators) | Lower |
Vector-change simply repositions the pads (e.g., anterior-posterior instead of anterior-lateral) before a repeat shock and is logistically easier.
Safety and Practical Concerns
- Equipment damage: Manufacturers have raised concerns about electrical damage to defibrillators when two units fire in close proximity.
- Operator safety: Risk of inadvertent rescuer electrocution is low with proper precautions (double gloves or electrically safe gloves), but must be considered. No rescuer deaths have been reported in published literature.
- Coordination: Requires two trained operators and two defibrillators - not always available in the field.
- Not in standard ACLS guidelines as a primary recommendation - it is a "may consider" option for refractory cases.
Summary
DSED is a reasonable escalation option for refractory VF after standard defibrillation and antiarrhythmics have failed. The DOSE VF trial provides the best evidence in its favor, particularly for true shock-refractory VF. Meta-analyses pooling observational data are less favorable, which likely reflects the generally dire prognosis of refractory VF overall. The technique is logistically demanding and carries device damage risk, but offers a potentially life-saving option when nothing else has worked.
Evidence note: The 2026 DOSE VF secondary analysis (PMID 41856454, May 2026) examining defibrillation current and pad position on ROSC may further refine pad positioning guidance - that is the most current RCT data available.
This is a shared conversation. Sign in to Orris to start your own chat.