Kussmul sign and kussmul breathing
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a detailed breakdown of both Kussmaul eponyms:
Kussmaul Sign vs. Kussmaul Breathing
These are two completely separate clinical findings named after the same physician, Adolf Kussmaul. They involve different organ systems and different diseases.
1. Kussmaul Sign (Cardiovascular)
Definition: A paradoxical rise in jugular venous pressure (JVP) on inspiration, or at minimum a failure of JVP to fall with inspiration (which is the normal expected response).
Normal physiology: During inspiration, intrathoracic pressure falls, which increases venous return to the right heart and causes JVP to decrease.
Why Kussmaul sign occurs: When the pericardium is scarred and non-compliant (constrictive pericarditis), the right ventricle cannot expand to accommodate the increased venous return on inspiration. Blood backs up into the jugular veins, causing JVP to rise instead of fall - a paradoxical response.
Classic associations:
- Constrictive pericarditis - the hallmark cause; also associated with Friedreich's sign (sharp, deep Y descent) and a pericardial knock (early, loud S3)
- Cardiac tamponade - though classic teaching is that tamponade does NOT show Kussmaul sign (unlike constrictive pericarditis)
- Right ventricular infarction
- Restrictive cardiomyopathy
Clinical context: Look for it alongside elevated JVP, hepatomegaly, ascites, and peripheral edema (right heart failure features) in a patient with prior pericarditis (viral, TB, radiation, post-cardiac surgery).
Here is the right atrial pressure tracing showing Kussmaul sign vs. normal:
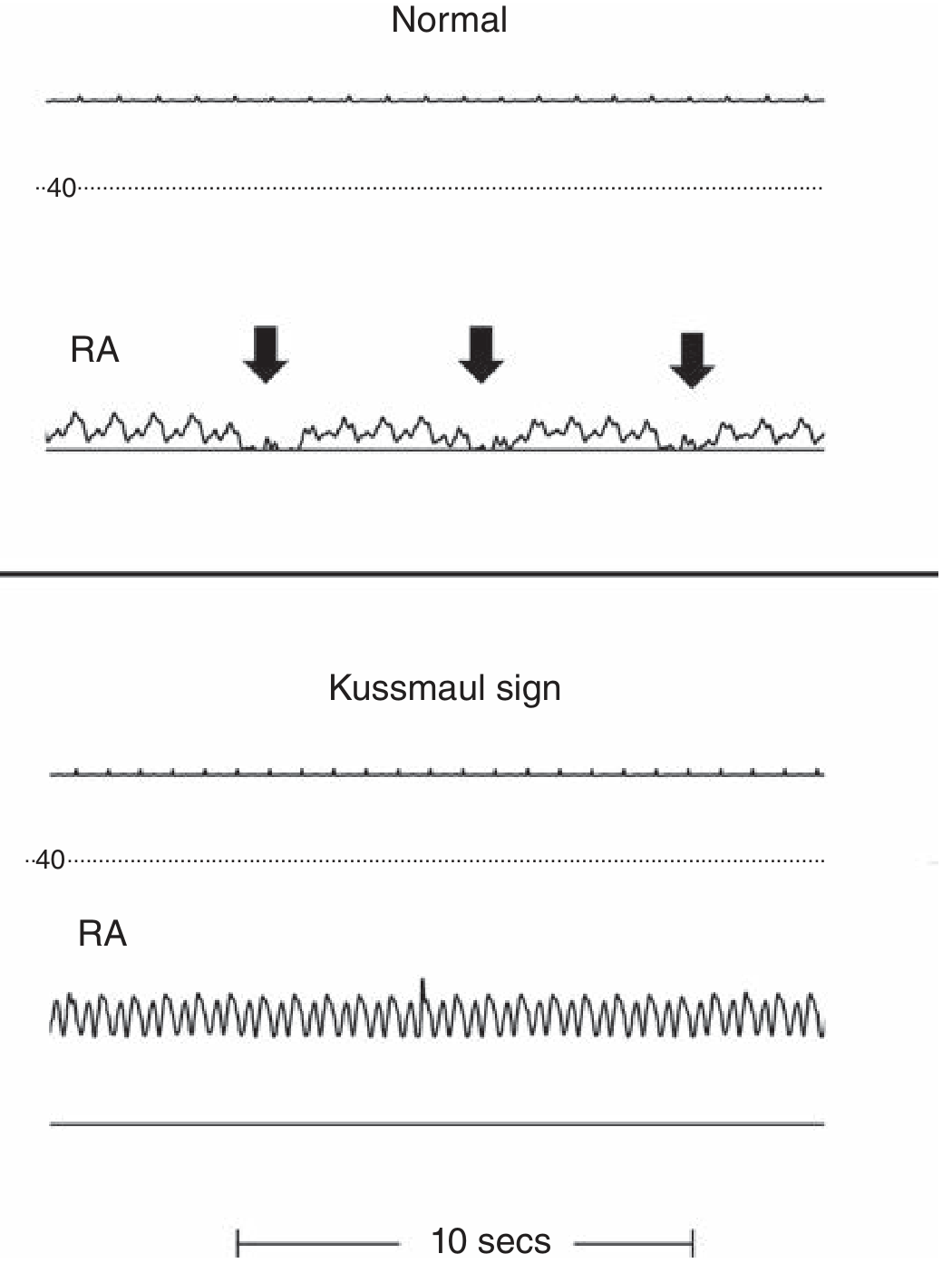
Figure: Normal RA pressure drops with each inspiration (arrows, top). In Kussmaul sign (bottom), RA pressure fails to fall on inspiration - seen in constrictive pericarditis. - Fuster and Hurst's The Heart, 15th Ed.
2. Kussmaul Breathing (Respiratory/Metabolic)
Definition: A pattern of deep, labored, and regular respirations - described originally as "air hunger" - driven by severe metabolic acidosis.
Historical origin: First described by Kussmaul in 1874 in three patients with diabetic ketoacidosis (DKA), who were breathing with large tidal volumes with virtually no pause between breaths - "as though exercising at rest." - Fishman's Pulmonary Diseases and Disorders
Mechanism:
- In metabolic acidosis (e.g., DKA), falling plasma bicarbonate and rising H+ ions stimulate peripheral and central chemoreceptors
- This drives a compensatory hyperventilation to blow off CO2
- The result is deep, regular, rapid (or sometimes slow) respirations that lower pCO2 and partially compensate for the metabolic acidosis
- The body is trying to maintain pH via the Henderson-Hasselbalch relationship: pH = 6.1 + log([HCO3−]/0.03 × pCO2)
Classic associations:
- Diabetic ketoacidosis (DKA) - prototype cause; fruity breath (ketones) + Kussmaul breathing are the classic exam pairing
- Alcoholic ketoacidosis
- Renal failure / uremic acidosis
- Ethylene glycol or methanol poisoning
- Any severe metabolic acidosis
Character of the breathing:
- Deep and regular (distinguishes it from Cheyne-Stokes or Biot breathing)
- Plum and Posner describe it as "deep but slow rhythmic breaths" in comatose acidotic patients
- Other sources emphasize it can be rapid and deep ("air hunger")
- Accomplished with little apparent effort despite being dramatic in appearance
Neurological note: Kussmaul breathing can also appear with pontomesencephalic structural lesions (though metabolic acidosis is by far the more common cause) - Harrison's Principles of Internal Medicine, 22E
Key Comparison Table
| Feature | Kussmaul Sign | Kussmaul Breathing |
|---|---|---|
| System | Cardiovascular | Respiratory/Metabolic |
| Finding | Paradoxical rise in JVP on inspiration | Deep, regular, labored respirations |
| Mechanism | Decreased RV compliance (rigid pericardium) → backed-up venous return | Metabolic acidosis → compensatory hyperventilation |
| Classic cause | Constrictive pericarditis | Diabetic ketoacidosis |
| Other causes | RV infarct, tamponade*, restrictive CM | Alcoholic ketoacidosis, renal failure, toxins |
| Associated findings | Pericardial knock, Friedreich's sign | Fruity breath, elevated ketones/anion gap |
Note: Kussmaul sign is classically absent in pure cardiac tamponade and is one clinical feature that helps distinguish constrictive pericarditis from tamponade.
Sources: Frameworks for Internal Medicine; Fuster and Hurst's The Heart, 15th Ed.; Washington Manual of Medical Therapeutics; Fishman's Pulmonary Diseases; Plum and Posner's Stupor and Coma; Harrison's Principles of Internal Medicine 22E
What are the sequence of questions to be asked for pt presented with haemorrhoids
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Now I have enough material from the textbooks to compile a comprehensive, well-structured answer.
History Taking for a Patient Presenting with Haemorrhoids
Important clinical pearl: Always verify the patient's self-diagnosis. The majority of patients who present with "haemorrhoids" have another explanation - anal fissure, pruritus ani, warts, abscess, or even colorectal cancer. Many patients attribute all perianal symptoms to haemorrhoids. - Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Sequence of Questions
1. PRESENTING COMPLAINT - Open Question
Start broad:
- "What has brought you in today? Tell me about your symptoms in your own words."
2. RECTAL BLEEDING (Most Common Presenting Symptom)
Bleeding is the typical symptom that first brings patients to the physician. Ask:
- Is there any blood? (Never assume they will volunteer this)
- Colour: Bright red, dark red, or maroon? (Haemorrhoidal blood is typically bright red)
- Where is the blood? On the toilet paper when wiping? Dripping into the toilet bowl? Coating the stool? Or mixed within the stool?
- Blood coating the outside or on paper = haemorrhoids/fissure (lower source)
- Blood mixed within stool = higher source, red flag for malignancy or IBD
- How much blood? Spots, streaks, or significant amounts?
- When does it occur? During defecation only, or at other times?
- How long has the bleeding been going on?
- Is it getting worse, better, or staying the same?
3. PAIN
- Is there any anal or rectal pain?
- When is the pain worst? During bowel movements? Afterward? When sitting? Straining?
- Internal haemorrhoids are typically painless (above dentate line, insensate mucosa)
- External or thrombosed haemorrhoids are painful
- Severe pain with bleeding points more to anal fissure
- Character of pain: Aching, sharp, throbbing?
- Duration: Does it go away quickly after passing stool, or persist for hours?
4. PROLAPSE / LUMP
This determines the grade of haemorrhoids and guides management:
- Do you notice anything coming down or out of your back passage?
- When does it happen? Only with straining/defecation, or at other times?
- Does it go back in on its own, or do you have to push it back in, or does it stay out permanently?
| Answer | Grade |
|---|---|
| No prolapse (bleeding only) | Grade I |
| Prolapse, reduces spontaneously | Grade II |
| Prolapse, requires manual reduction | Grade III |
| Irreducible prolapse | Grade IV |
5. PRURITUS AND DISCHARGE / SOILING
- Do you have itching or soreness around the anus?
- Prolapsed haemorrhoids cause perianal moisture which leads to pruritus ani
- Any mucus or discharge? Blood or mucus on underwear?
- Any soiling or faecal leakage?
- Chronic prolapse can impair sphincter continence
6. BOWEL HABITS
This is essential both for risk factors and to exclude serious pathology:
- What are your normal bowel habits?
- Any change in bowel habits recently? Change in frequency, consistency, or urgency?
- A change in bowel habits is a red flag for colorectal cancer
- Are your stools hard or soft? Constipation is a major risk factor
- Do you strain at stool? How long do you typically sit on the toilet?
- Prolonged toilet sitting and straining are key precipitating factors
- Any diarrhoea? (Loose stools also worsen haemorrhoids)
7. RED FLAG SYMPTOMS (Must Not Miss)
Always screen for features that would mandate urgent investigation to exclude colorectal cancer:
- Any unintentional weight loss?
- Any change in appetite?
- Feeling of incomplete evacuation (tenesmus)?
- Blood mixed in with the stool (as opposed to coating it)?
- Any dark/tarry stools (melaena)?
- Mucus mixed with stool?
- Abdominal pain or bloating?
Studies show that 24% of patients presenting with rectal bleeding have serious disease (polyps 13%, colon cancer 6.5%, IBD 4%). Even patients with a clear anorectal source like haemorrhoids can also have coincidental polyps or cancer. - Symptom to Diagnosis, 4th Ed.
8. PAST MEDICAL AND SURGICAL HISTORY
- Any previous haemorrhoids or anal surgery?
- Previous colonoscopy - when, and what did it show?
- Known inflammatory bowel disease?
- Liver disease / portal hypertension? (causes rectal varices, often mistaken for haemorrhoids)
- History of colorectal cancer or polyps?
- Bleeding disorders or clotting problems?
- Any chronic conditions: obesity, cardiac disease (relevant if surgery is considered)?
9. DRUG HISTORY
- Anticoagulants (warfarin, DOACs) or antiplatelets (aspirin, clopidogrel)? - will worsen bleeding and affect management
- Opioids or iron supplements - cause constipation, worsen haemorrhoids
- NSAIDs - can worsen GI bleeding
- Any topical preparations already being used?
- Laxatives - what has the patient already tried?
10. DIET AND LIFESTYLE
- Fibre intake - fruit, vegetables, wholegrain? Low-fibre diet is the principal dietary risk factor
- Fluid intake - adequate water intake softens stools
- Alcohol intake? (contributes to portal hypertension and dehydration)
- Physical activity level? (sedentary lifestyle is a risk factor)
- Occupation - prolonged sitting (e.g., truck drivers, office workers)
11. OBSTETRIC AND GYNAECOLOGICAL HISTORY (Women)
- Pregnancies and deliveries? Haemorrhoids occur in up to 85% of multiparous women due to vena cava compression, increased intra-abdominal pressure, and hormonal effects (progesterone/motilin)
- Current pregnancy?
- Mode of delivery - any perineal trauma?
12. FAMILY HISTORY
- Family history of colorectal cancer?
- Family history of IBD or polyposis syndromes (FAP, Lynch syndrome)?
- Haemorrhoids can have a genetic/familial predisposition
13. SOCIAL HISTORY
- Smoking - risk factor for IBD and colon cancer
- Occupation and activity level
- Ability to manage conservative treatments at home (sitz baths, diet changes)
- Any concerns or fears about surgery?
Summary Framework (SOCRATES + RED FLAGS)
| Domain | Key Questions |
|---|---|
| Bleeding | Colour, volume, location relative to stool, timing |
| Pain | Presence, timing, character (suggests fissure vs. haemorrhoids) |
| Prolapse | Occurs? Self-reducing? Manual? Irreducible? (grades I-IV) |
| Itch/Discharge | Pruritus ani, soiling, mucus |
| Bowel habits | Constipation, diarrhoea, change in habit, straining |
| Red flags | Weight loss, change in habit, blood mixed in stool, tenesmus |
| PMH/drugs | Anticoagulants, prior bowel disease, liver disease |
| Diet/lifestyle | Fibre, fluids, activity, pregnancy |
| Family history | CRC, IBD, polyposis |
Sources: Sleisenger and Fordtran's GI and Liver Disease; Textbook of Family Medicine 9e; Symptom to Diagnosis 4th Ed.; Yamada's Textbook of Gastroenterology 7th Ed.; Clinical GI Endoscopy 3e; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.