Guidelines for using statins
Reading File
Finding Sources
Searching PubMed
"statin" AND "guidelines" AND "cardiovascular"
Searching the Web
statin therapy guidelines 2024 2025 ACC AHA indications intensity
Reading File
Reading File
Reading Article
PMID: 41824590
Reading File
Reading Web Page
https://www.tctmd.com/news/lower-ldl-levels-starting-earlier…
Loading Image
Loading Image
I now have comprehensive, high-quality information from multiple authoritative sources including the brand-new 2026 ACC/AHA guideline. Here is a complete, well-organized answer.
Guidelines for Using Statins
Statins (HMG-CoA reductase inhibitors) are the cornerstone of lipid-lowering pharmacotherapy. The most current guidance comes from the 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia (Blumenthal et al., JACC 2026 - PMID 41824590), which replaces the 2018 guideline.
Mechanism of Action
Statins competitively inhibit HMG-CoA reductase, blocking the rate-limiting step in hepatic cholesterol synthesis. This leads to:
- Upregulation of LDL receptors on hepatocytes -> increased LDL-C clearance
- Reduced VLDL production -> lower triglycerides at high doses
- A ~22% reduction in ASCVD events per 1 mmol/L (39 mg/dL) reduction in LDL-C
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Statin Intensity Categories
| Intensity | LDL-C Reduction | Examples |
|---|---|---|
| High | ≥50% | Atorvastatin 40-80 mg, Rosuvastatin 20-40 mg |
| Moderate | 30-49% | Atorvastatin 10-20 mg, Rosuvastatin 5-10 mg, Simvastatin 20-40 mg, Pravastatin 40-80 mg, Pitavastatin 1-4 mg |
| Low | <30% | Fluvastatin 20-40 mg, Lovastatin 20 mg |
Note: Rosuvastatin is roughly twice as potent per mg as atorvastatin, which is roughly twice as potent as simvastatin.
Who Should Receive Statins
Automatic High-Intensity Statin (no risk calculation needed)
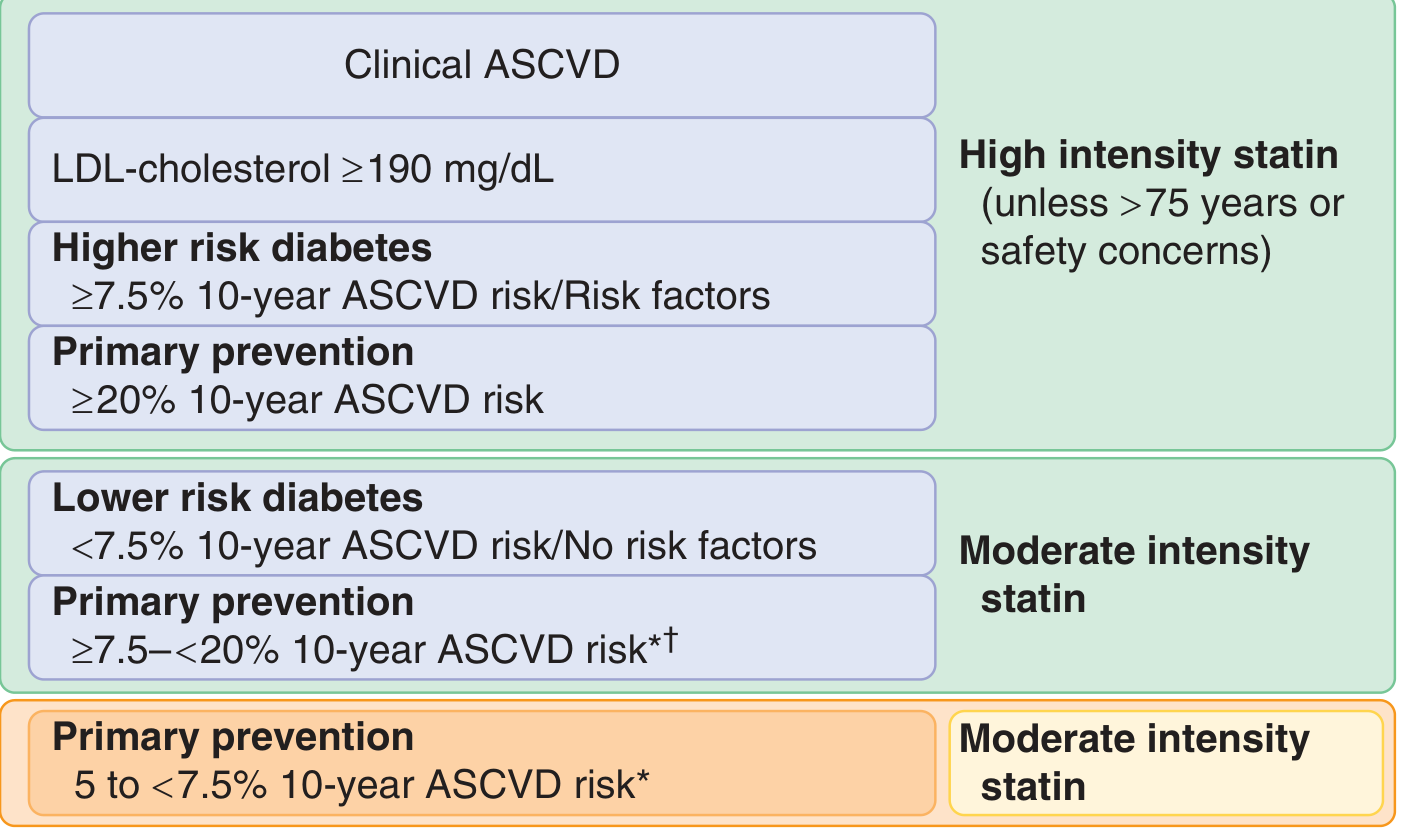
- Clinical ASCVD (prior MI, stroke, TIA, stable angina, revascularization, PAD)
- LDL-C ≥ 190 mg/dL (familial hypercholesterolemia pattern)
- Higher-risk diabetes (≥7.5% 10-year ASCVD risk or with risk factors)
- Primary prevention with ≥20% 10-year ASCVD risk
Exception: consider moderate-intensity if age >75 years or safety concerns exist.
Moderate-Intensity Statin (after clinician-patient discussion)
- Lower-risk diabetes (<7.5% 10-year ASCVD risk, no major risk factors)
- Primary prevention with 7.5-<20% 10-year ASCVD risk
- Evidence also supports considering statins at 5-<7.5% 10-year risk
Risk Calculator
The PREVENT-ASCVD equations (updated in 2026, replacing Pooled Cohort Equations) classify risk as: low (<3%), borderline (3-<5%), intermediate (5-<10%), high (≥10%). The ACC ASCVD Risk Estimator is freely available.
2026 Guideline Key Updates
The 2026 ACC/AHA guideline introduced several important changes from 2018:
-
LDL-C treatment targets are back - The guideline re-introduces specific LDL goals (abandoned in 2013-2018):
- Very high risk / established ASCVD: LDL-C <55 mg/dL
- High risk (10-year risk ≥10%): LDL-C <70 mg/dL
- Borderline/intermediate risk on treatment: LDL-C <100 mg/dL
-
CAC-guided treatment targets:
- CAC 100-999 AU: treat to LDL-C <70 mg/dL and non-HDL-C <100 mg/dL (Class I)
- CAC ≥1,000 AU: aim for ≥50% LDL-C reduction and target <55 mg/dL (Class I)
- CAC = 0 may allow deferring statin in borderline/intermediate-risk patients
-
30-year risk is now incorporated, encouraging earlier treatment in younger patients with high lifetime risk
-
Special populations now get explicit Class I recommendations:
- CKD stage 3-4: intensive therapy to LDL-C <55 mg/dL
- HIV patients aged 40-75 on stable ART
- Cancer survivors with ASCVD risk factors
- ACS: high-intensity statin + option to add ezetimibe concurrently at discharge
Adding Non-Statin Therapy
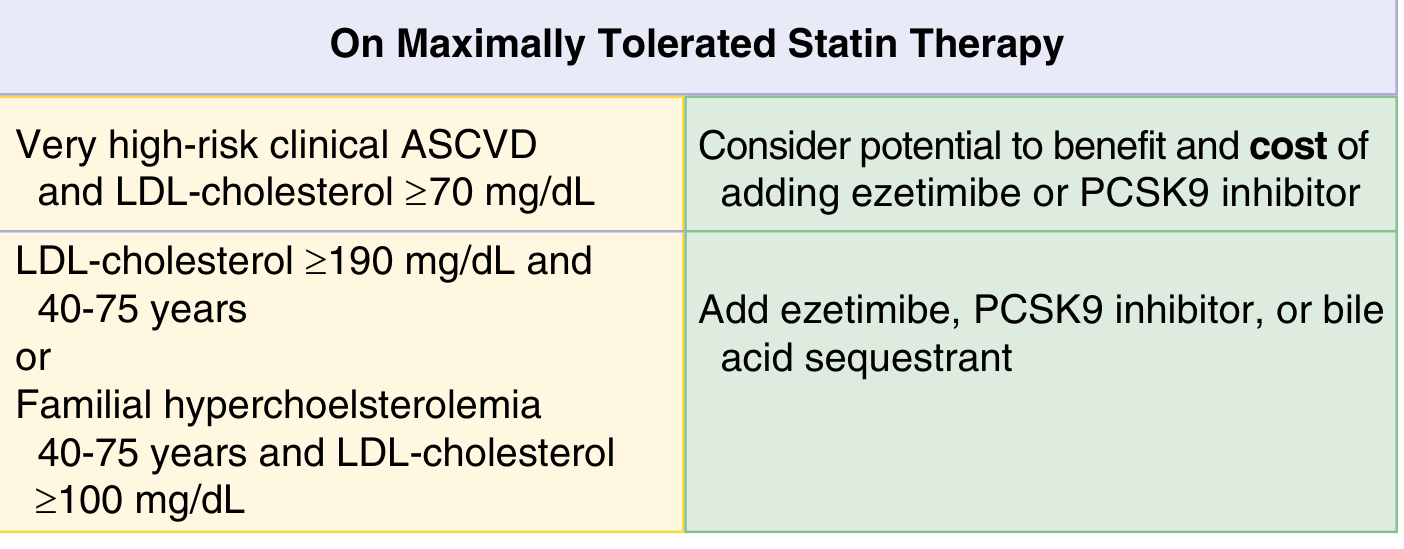
When patients are on maximally tolerated statin therapy but LDL-C remains elevated:
| Situation | Action |
|---|---|
| Very high-risk ASCVD + LDL-C ≥70 mg/dL | Add ezetimibe or PCSK9 inhibitor (weigh cost) |
| LDL-C ≥190 mg/dL (age 40-75) or FH with LDL-C ≥100 mg/dL | Add ezetimibe, PCSK9 inhibitor, or bile acid sequestrant |
| ACS, already on max statin + LDL-C ≥70 mg/dL | Non-statin agent recommended (Class I) |
A 2025 meta-analysis (PMID 40126455) confirmed that statin + ezetimibe combination reduces major CV events beyond statin monotherapy.
Monitoring Statin Therapy
(Goldman-Cecil Medicine)
- Fasting lipid panel: at baseline, 4-12 weeks after initiation/dose change, then every 3-12 months
- Hepatic transaminases: No routine ongoing monitoring needed if baseline is <2x ULN. If 2-3x ULN, recheck in 3 months. If >3x ULN, investigate for other causes before starting/continuing.
- CK: Not routinely checked; only if muscle symptoms develop
Safety Profile
Muscle symptoms are the most common concern, but >90% of reported symptoms in statin users are not actually caused by the statin (nocebo effect is significant). Steps for managing symptoms:
| Severity | Action |
|---|---|
| Mild-moderate pain | Stop, wait for resolution, rechallenge with lower dose or different statin |
| Severe pain or weakness | Stop, check CK/creatinine/myoglobin; hospitalize if CK >10x ULN with renal impairment |
| Jaundice or persistent transaminases >5x ULN | Stop, evaluate for other causes |
| New-onset diabetes | Continue statin, encourage lifestyle modification, treat diabetes |
Key safety notes:
- Pregnancy/lactation: CONTRAINDICATED. Counsel women of childbearing potential.
- Diabetes risk: statins slightly accelerate diabetes onset by ~2 months in those already predisposed - the ASCVD benefit far outweighs this risk (CTT meta-analysis, Lancet Diabetes Endocrinol 2024 - PMID 38554713)
- No clinically meaningful hepatotoxicity from statins
- Drug interactions: potent inhibitors of CYP3A4 (e.g., certain antifungals, macrolides, HIV protease inhibitors) can raise simvastatin/lovastatin levels markedly - prefer pravastatin or rosuvastatin in these situations
Special Situations
| Situation | Recommendation |
|---|---|
| Age >75 years | Moderate-intensity generally preferred; individualize based on benefit vs. risk |
| Heart failure (ischemic, HFrEF, reasonable life expectancy) | May consider moderate-intensity statin |
| Hemodialysis | Not routinely started; can continue if already initiated |
| Perioperative (non-cardiac surgery) | Continue statins perioperatively if already on them |
| CKD stage 3-4 | Intensive therapy targeting LDL-C <55 mg/dL (2026 Class I) |
Sources:
- Goldman-Cecil Medicine, International Edition - Chapters 190, 40
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Chapter 37
- 2026 ACC/AHA Dyslipidemia Guideline (Blumenthal et al., JACC/Circulation, Apr-May 2026)
- CTT Collaboration, Lancet Diabetes Endocrinol 2024 [PMID 38554713]
- Banach et al., Mayo Clin Proc 2025 [PMID 40126455]
Create a statin dosing reference table with all intensities and drug comparisons
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have all the data I need from multiple textbooks. Here is the comprehensive statin dosing reference table:
Statin Dosing Reference Table
Table 1: Statin Intensity by Drug and Dose
| Drug | High Intensity (LDL-C ↓ ≥50%) | Moderate Intensity (LDL-C ↓ 30-49%) | Low Intensity (LDL-C ↓ <30%) |
|---|---|---|---|
| Atorvastatin | 40-80 mg | 10-20 mg | - |
| Rosuvastatin | 20-40 mg | 5-10 mg | - |
| Simvastatin | - | 20-40 mg | 10 mg |
| Pravastatin | - | 40-80 mg | 10-20 mg |
| Lovastatin | - | 40 mg | 20 mg |
| Fluvastatin | - | 80 mg XL or 40 mg BID | 20-40 mg |
| Pitavastatin | - | 2-4 mg | 1 mg |
Note: Only atorvastatin and rosuvastatin achieve high-intensity effect. All other statins cap at moderate intensity.
(Sources: Washington Manual of Medical Therapeutics, Table 3-10; Henry's Clinical Diagnosis & Management by Laboratory Methods, Table 18.9)
Table 2: Drug-by-Drug Comparison
| Property | Atorvastatin | Rosuvastatin | Simvastatin | Pravastatin | Lovastatin | Fluvastatin | Pitavastatin |
|---|---|---|---|---|---|---|---|
| Max dose | 80 mg | 40 mg | 40 mg* | 80 mg | 80 mg | 80 mg XL | 4 mg |
| Max intensity | High | High | Moderate | Moderate | Moderate | Moderate | Moderate |
| Metabolism | CYP3A4 | Minimal CYP | CYP3A4 | Not CYP | CYP3A4 | CYP2C9 | CYP2C9 (minor) |
| Lipophilicity | Lipophilic | Hydrophilic | Lipophilic | Hydrophilic | Lipophilic | Lipophilic | Lipophilic |
| Renal excretion | <2% | ~10% | <13% | ~20% | ~10% | ~5% | ~15% |
| Half-life | ~14 h | ~19 h | ~3 h | ~2-3 h | ~3 h | ~3 h | ~12 h |
| Dosing | Any time | Any time | Evening | Any time | With evening meal | Any time | Any time |
| CKD-friendly | Yes | Caution (dose limit 10 mg in severe CKD) | Yes | Yes | Yes | Yes | Yes (preferred in CKD) |
| Drug interactions (CYP3A4) | High risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Crosses BBB | Yes | No | Yes | No | Yes | No | No |
*Simvastatin 80 mg is no longer recommended due to myopathy risk - FDA restricts new initiations at this dose.
Table 3: Which Intensity for Which Patient?
| Clinical Situation | Recommended Intensity | Preferred Agents |
|---|---|---|
| Clinical ASCVD (secondary prevention), age ≤75 | High | Atorvastatin 40-80 mg or Rosuvastatin 20-40 mg |
| Clinical ASCVD, age >75 | Moderate (individualize) | Atorvastatin 10-20 mg or Rosuvastatin 5-10 mg |
| ACS (acute coronary syndrome) | High (initiate at admission) | Atorvastatin 80 mg or Rosuvastatin 40 mg |
| LDL-C ≥190 mg/dL (FH) | High | Atorvastatin 40-80 mg or Rosuvastatin 20-40 mg |
| Diabetes + ≥7.5% 10-yr ASCVD risk | High | Atorvastatin 40-80 mg or Rosuvastatin 20-40 mg |
| Diabetes + <7.5% 10-yr ASCVD risk | Moderate | Any moderate-intensity agent |
| Primary prevention, 10-yr risk ≥20% | High | Atorvastatin 40-80 mg or Rosuvastatin 20-40 mg |
| Primary prevention, 10-yr risk 7.5-<20% | Moderate | Any moderate-intensity agent |
| Primary prevention, 10-yr risk 5-<7.5% | Moderate (after discussion) | Any moderate-intensity agent |
| CKD stage 3-4 (2026 guideline, target LDL <55) | High | Atorvastatin 40-80 mg (preferred) |
| On dialysis | Not routinely started | - |
| Drug interaction risk (e.g., calcineurin inhibitors, azole antifungals, HIV PIs) | Moderate with low-interaction statin | Pravastatin, Fluvastatin, or Pitavastatin |
| Heart failure (ischemic, HFrEF, not on statin) | Moderate (may consider) | Rosuvastatin 5-10 mg |
Table 4: LDL-C Targets (2026 ACC/AHA Guideline)
| Risk Category | LDL-C Target |
|---|---|
| Very high-risk ASCVD (multiple events or event + high-risk conditions) | <55 mg/dL |
| High-risk ASCVD / CAC ≥1,000 AU | <55 mg/dL (≥50% reduction from baseline) |
| High 10-yr risk (≥10%) or CAC 100-999 AU | <70 mg/dL |
| Intermediate risk / on statin therapy | <100 mg/dL |
| Borderline risk (3-<5%), if treatment chosen | <100 mg/dL |
| LDL-C ≥190 mg/dL on statin alone | Add non-statin if LDL-C remains >100 mg/dL |
Table 5: When to Add Non-Statin Therapy
| Situation | Add-on Agent(s) |
|---|---|
| Very high-risk ASCVD + LDL-C ≥70 on max statin | Ezetimibe first, then PCSK9 inhibitor |
| LDL-C ≥190 on max statin, LDL-C still >100 | Ezetimibe, then PCSK9 inhibitor or bile acid sequestrant |
| ACS, on max statin + LDL-C ≥70 mg/dL | Ezetimibe or PCSK9 inhibitor (Class I) |
| FH, homozygous | Lomitapide, mipomersen, LDL apheresis |
Quick Reference: High-Intensity Dosing Only
| Drug | Dose | Expected LDL-C Reduction |
|---|---|---|
| Atorvastatin | 40 mg daily | ~47-50% |
| Atorvastatin | 80 mg daily | ~55-60% |
| Rosuvastatin | 20 mg daily | ~52-55% |
| Rosuvastatin | 40 mg daily | ~55-63% |
Rosuvastatin is approximately twice as potent per mg as atorvastatin, which is twice as potent as simvastatin. (Goodman & Gilman's)
Key clinical pearls:
- Avoid simvastatin 80 mg - FDA restricted due to myopathy risk; downgrade to 40 mg max or switch agent
- Pitavastatin is preferred in patients with high drug-interaction burden (metabolized minimally by CYP2C9, not CYP3A4)
- Rosuvastatin dose should not exceed 10 mg in patients with severe renal impairment (eGFR <30) or those on cyclosporine
- Pravastatin and pitavastatin are preferred when statin is needed during organ transplant (minimal interaction with calcineurin inhibitors)
- Pregnancy: all statins are contraindicated (Category X)
Sources: Washington Manual of Medical Therapeutics (Table 3-10); Henry's Clinical Diagnosis & Management by Laboratory Methods (Table 18.9); Goldman-Cecil Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; 2026 ACC/AHA Dyslipidemia Guideline [PMID 41824590]
Create a downloadable PDF reference card of this dosing table
Reading File
Running Command
mkdir -p /home/daytona/workspace/statin-reference && ls /home/daytona/workspace/statin-reference
Writing File
~/statin-reference/generate_pdf.py
from reportlab.lib.pagesizes import A4, landscape
from reportlab.lib import colors
from reportlab.lib.units import mm
from reportlab.platypus import (
SimpleDocTemplate, Table, TableStyle, Paragraph, Spacer,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_RIGHT
from reportlab.platypus import Flowable
OUTPUT = "/home/daytona/workspace/statin-reference/Statin_Dosing_Reference_Card.pdf"
# ── Colour palette ─────────────────────────────────────────────────────────────
C_NAVY = colors.HexColor("#1a3a5c")
C_TEAL = colors.HexColor("#1a7a8a")
C_HIGH = colors.HexColor("#c0392b") # high intensity rows
C_HIGH_LT = colors.HexColor("#fdecea")
C_MOD = colors.HexColor("#1a7a8a") # moderate intensity rows
C_MOD_LT = colors.HexColor("#e8f6f8")
C_LOW = colors.HexColor("#7f8c8d") # low intensity rows
C_LOW_LT = colors.HexColor("#f4f4f4")
C_HEADER = colors.HexColor("#1a3a5c")
C_HDR_TEXT = colors.white
C_ALT = colors.HexColor("#f0f4f8")
C_WARN = colors.HexColor("#fff3cd")
C_WARN_BRD = colors.HexColor("#e6a817")
C_BLACK = colors.HexColor("#1a1a1a")
C_GREY = colors.HexColor("#555555")
C_LIGHT_GREY= colors.HexColor("#e0e0e0")
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=12*mm, rightMargin=12*mm,
topMargin=12*mm, bottomMargin=12*mm,
title="Statin Dosing Reference Card",
author="Orris Medical Reference",
subject="Statin therapy guidelines 2026 ACC/AHA"
)
W, H = A4
usable_w = W - 24*mm
styles = getSampleStyleSheet()
# ── Custom paragraph styles ────────────────────────────────────────────────────
def ps(name, parent="Normal", **kwargs):
return ParagraphStyle(name, parent=styles[parent], **kwargs)
title_style = ps("Title2", fontSize=18, textColor=C_HDR_TEXT, alignment=TA_CENTER,
fontName="Helvetica-Bold", spaceAfter=2)
subtitle_style= ps("Sub", fontSize=9, textColor=colors.HexColor("#b0c4de"),
alignment=TA_CENTER, fontName="Helvetica", spaceAfter=0)
section_style = ps("Sect", fontSize=10, textColor=C_HDR_TEXT, fontName="Helvetica-Bold",
alignment=TA_LEFT, spaceBefore=4, spaceAfter=2)
cell_style = ps("Cell", fontSize=7.5, textColor=C_BLACK, fontName="Helvetica",
leading=10)
cell_bold = ps("CellB", fontSize=7.5, textColor=C_BLACK, fontName="Helvetica-Bold",
leading=10)
cell_hdr = ps("CellH", fontSize=7.5, textColor=C_HDR_TEXT, fontName="Helvetica-Bold",
leading=10, alignment=TA_CENTER)
cell_center = ps("CellC", fontSize=7.5, textColor=C_BLACK, fontName="Helvetica",
leading=10, alignment=TA_CENTER)
cell_red = ps("CellR", fontSize=7.5, textColor=C_HIGH, fontName="Helvetica-Bold",
leading=10, alignment=TA_CENTER)
cell_teal = ps("CellT", fontSize=7.5, textColor=C_MOD, fontName="Helvetica-Bold",
leading=10, alignment=TA_CENTER)
cell_grey = ps("CellG", fontSize=7.5, textColor=C_LOW, fontName="Helvetica",
leading=10, alignment=TA_CENTER)
note_style = ps("Note", fontSize=6.5, textColor=C_GREY, fontName="Helvetica-Oblique",
leading=8.5, spaceBefore=1)
source_style = ps("Src", fontSize=6, textColor=C_GREY, fontName="Helvetica",
leading=7.5, spaceBefore=2)
pearl_style = ps("Pearl", fontSize=7, textColor=C_BLACK, fontName="Helvetica",
leading=9.5, spaceBefore=0)
def P(txt, style=cell_style): return Paragraph(txt, style)
def PH(txt): return Paragraph(txt, cell_hdr)
def PC(txt): return Paragraph(txt, cell_center)
def PB(txt): return Paragraph(txt, cell_bold)
# ── Table helper ───────────────────────────────────────────────────────────────
def base_style(has_header=True):
s = [
("GRID", (0,0), (-1,-1), 0.4, C_LIGHT_GREY),
("ROWBACKGROUNDS", (0, 1 if has_header else 0), (-1,-1), [colors.white, C_ALT]),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING",(0,0), (-1,-1), 4),
]
if has_header:
s += [
("BACKGROUND", (0,0), (-1,0), C_HEADER),
("ROWBACKGROUNDS", (0,0), (-1,0), [C_HEADER]),
]
return s
# ── Section banner ─────────────────────────────────────────────────────────────
def section_banner(text, color=C_NAVY):
data = [[Paragraph(text, section_style)]]
t = Table(data, colWidths=[usable_w])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), color),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING",(0,0), (-1,-1), 4),
("ROUNDEDCORNERS", [3]),
]))
return t
# ── Header banner ──────────────────────────────────────────────────────────────
def header_block():
data = [
[Paragraph("STATIN DOSING REFERENCE CARD", title_style)],
[Paragraph("Based on 2026 ACC/AHA/AACVPR Dyslipidemia Guideline | Goldman-Cecil Medicine | Goodman & Gilman's", subtitle_style)],
]
t = Table(data, colWidths=[usable_w])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_NAVY),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING",(0,0),(-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING",(0,0), (-1,-1), 8),
]))
return t
# ── Legend strip ───────────────────────────────────────────────────────────────
def legend_strip():
items = [
(C_HIGH, C_HIGH_LT, "HIGH intensity ≥50% LDL↓"),
(C_MOD, C_MOD_LT, "MODERATE intensity 30-49% LDL↓"),
(C_LOW, C_LOW_LT, "LOW intensity <30% LDL↓"),
]
cells = []
for fg, bg, label in items:
p = Paragraph(f'<font color="#{fg.hexval()[1:]}"><b>{label}</b></font>',
ps("leg", fontSize=7, fontName="Helvetica-Bold", alignment=TA_CENTER, leading=9))
cells.append(p)
t = Table([cells], colWidths=[usable_w/3]*3)
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (0,0), C_HIGH_LT),
("BACKGROUND", (1,0), (1,0), C_MOD_LT),
("BACKGROUND", (2,0), (2,0), C_LOW_LT),
("BOX", (0,0), (0,0), 0.6, C_HIGH),
("BOX", (1,0), (1,0), 0.6, C_MOD),
("BOX", (2,0), (2,0), 0.6, C_LOW),
("TOPPADDING", (0,0),(-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1), 4),
]))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# TABLE 1: Intensity by Drug & Dose
# ═══════════════════════════════════════════════════════════════════════════════
def table1():
cw = [usable_w*0.20, usable_w*0.25, usable_w*0.30, usable_w*0.25]
hdr = [PH("Drug"), PH("High Intensity\n(LDL-C ↓ ≥50%)"), PH("Moderate Intensity\n(LDL-C ↓ 30–49%)"), PH("Low Intensity\n(LDL-C ↓ <30%)")]
rows = [
[PB("Atorvastatin"), Paragraph("<b>40–80 mg</b>", cell_red), PC("10–20 mg"), PC("—")],
[PB("Rosuvastatin"), Paragraph("<b>20–40 mg</b>", cell_red), PC("5–10 mg"), PC("—")],
[PB("Simvastatin"), PC("—"), PC("20–40 mg"), PC("10 mg")],
[PB("Pravastatin"), PC("—"), PC("40–80 mg"), PC("10–20 mg")],
[PB("Lovastatin"), PC("—"), PC("40 mg"), PC("20 mg")],
[PB("Fluvastatin"), PC("—"), PC("80 mg XL\n40 mg BID"), PC("20–40 mg")],
[PB("Pitavastatin"), PC("—"), PC("2–4 mg"), PC("1 mg")],
]
data = [hdr] + rows
t = Table(data, colWidths=cw, repeatRows=1)
style = base_style()
# Colour HIGH intensity cells
style += [
("BACKGROUND", (1,1), (1,2), C_HIGH_LT),
("BACKGROUND", (2,1), (2,7), C_MOD_LT),
("BACKGROUND", (3,1), (3,7), C_LOW_LT),
# dash cells neutral
("TEXTCOLOR", (1,3), (1,7), C_GREY),
]
t.setStyle(TableStyle(style))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# TABLE 2: High-Intensity Quick Reference
# ═══════════════════════════════════════════════════════════════════════════════
def table2():
cw = [usable_w*0.25, usable_w*0.25, usable_w*0.50]
hdr = [PH("Drug"), PH("Dose"), PH("Expected LDL-C Reduction")]
rows = [
[PB("Atorvastatin"), Paragraph("<b>40 mg</b>", cell_red), Paragraph("~47–50%", cell_red)],
[PB("Atorvastatin"), Paragraph("<b>80 mg</b>", cell_red), Paragraph("~55–60% (max dose)", cell_red)],
[PB("Rosuvastatin"), Paragraph("<b>20 mg</b>", cell_red), Paragraph("~52–55%", cell_red)],
[PB("Rosuvastatin"), Paragraph("<b>40 mg</b>", cell_red), Paragraph("~55–63% (max dose)", cell_red)],
]
data = [hdr] + rows
t = Table(data, colWidths=cw, repeatRows=1)
style = base_style()
style += [("BACKGROUND", (0,1), (-1,-1), C_HIGH_LT)]
t.setStyle(TableStyle(style))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# TABLE 3: Drug Comparison
# ═══════════════════════════════════════════════════════════════════════════════
def table3():
props = ["Max dose", "Max intensity", "Metabolism", "Lipophilicity",
"Half-life", "Dosing time", "Drug interactions\n(CYP3A4 risk)", "CKD note"]
drugs = ["Atorva-\nstatin", "Rosuva-\nstatin", "Simva-\nstatin", "Prava-\nstatin",
"Lova-\nstatin", "Fluva-\nstatin", "Pitava-\nstatin"]
values = [
["80 mg", "40 mg", "40 mg*", "80 mg", "80 mg", "80 mg XL", "4 mg"],
["HIGH", "HIGH", "Mod.", "Mod.", "Mod.", "Mod.", "Mod."],
["CYP3A4", "Minimal", "CYP3A4", "Non-CYP", "CYP3A4", "CYP2C9", "CYP2C9\n(minor)"],
["Lipophilic","Hydro-\nphilic","Lipophilic","Hydro-\nphilic","Lipophilic","Lipophilic","Lipophilic"],
["~14 h", "~19 h", "~3 h", "~2-3 h", "~3 h", "~3 h", "~12 h"],
["Any time","Any time","Evening", "Any time","w/ evening\nmeal","Any time","Any time"],
["HIGH", "LOW", "HIGH", "LOW", "HIGH", "LOW", "LOW"],
["OK", "≤10 mg if\neGFR<30", "OK", "OK (preferred)","OK","OK","Preferred\nin CKD"],
]
tiny = ps("Tiny", fontSize=6.5, fontName="Helvetica", leading=8.5, alignment=TA_CENTER)
tiny_b = ps("TinyB", fontSize=6.5, fontName="Helvetica-Bold", leading=8.5, alignment=TA_CENTER)
tiny_hdr = ps("TinyH", fontSize=6.5, fontName="Helvetica-Bold", leading=8.5,
alignment=TA_CENTER, textColor=C_HDR_TEXT)
tiny_prop = ps("TinyP", fontSize=6.5, fontName="Helvetica-Bold", leading=8.5,
alignment=TA_LEFT, textColor=C_HDR_TEXT)
prop_w = usable_w * 0.155
drug_w = (usable_w - prop_w) / 7
hdr_row = [Paragraph("Property", tiny_prop)] + [Paragraph(d, tiny_hdr) for d in drugs]
data = [hdr_row]
for i, prop in enumerate(props):
row = [Paragraph(prop, ps(f"tp{i}", fontSize=6.5, fontName="Helvetica-Bold",
leading=8.5, alignment=TA_LEFT))]
for j, val in enumerate(values[i]):
if val in ("HIGH", "HIGH\n(risk)"):
row.append(Paragraph(val, ps(f"hv{i}{j}", fontSize=6.5, fontName="Helvetica-Bold",
leading=8.5, alignment=TA_CENTER, textColor=C_HIGH)))
elif val in ("Mod.", "LOW"):
clr = C_MOD if val == "Mod." else colors.HexColor("#27ae60")
row.append(Paragraph(val, ps(f"mv{i}{j}", fontSize=6.5, fontName="Helvetica-Bold",
leading=8.5, alignment=TA_CENTER, textColor=clr)))
else:
row.append(Paragraph(val, tiny))
data.append(row)
cw = [prop_w] + [drug_w]*7
t = Table(data, colWidths=cw, repeatRows=1)
style = base_style()
style += [
("BACKGROUND", (0,0), (0,-1), C_TEAL),
("BACKGROUND", (0,0), (-1,0), C_HEADER),
("ROWBACKGROUNDS", (1,1), (-1,-1), [colors.white, C_ALT]),
]
t.setStyle(TableStyle(style))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# TABLE 4: Who Gets What Intensity
# ═══════════════════════════════════════════════════════════════════════════════
def table4():
cw = [usable_w*0.40, usable_w*0.22, usable_w*0.38]
hdr = [PH("Clinical Situation"), PH("Intensity"), PH("Preferred Agent(s)")]
data_rows = [
("Clinical ASCVD, age ≤75 (secondary prevention)", "HIGH",
"Atorvastatin 40–80 mg\nRosuvastatin 20–40 mg"),
("Clinical ASCVD, age >75", "MODERATE",
"Atorvastatin 10–20 mg\nRosuvastatin 5–10 mg"),
("ACS — initiate at admission", "HIGH",
"Atorvastatin 80 mg or Rosuvastatin 40 mg"),
("LDL-C ≥190 mg/dL (familial hypercholesterolaemia)", "HIGH",
"Atorvastatin 40–80 mg\nRosuvastatin 20–40 mg"),
("Diabetes + 10-yr ASCVD risk ≥7.5%", "HIGH",
"Atorvastatin 40–80 mg\nRosuvastatin 20–40 mg"),
("Diabetes + 10-yr ASCVD risk <7.5%", "MODERATE",
"Any moderate-intensity agent"),
("Primary prevention, 10-yr risk ≥20%", "HIGH",
"Atorvastatin 40–80 mg\nRosuvastatin 20–40 mg"),
("Primary prevention, 10-yr risk 7.5–<20%", "MODERATE",
"Any moderate-intensity agent"),
("Primary prevention, 10-yr risk 5–<7.5%", "MODERATE\n(after discussion)",
"Any moderate-intensity agent"),
("CKD stage 3–4 (target LDL <55 mg/dL)", "HIGH",
"Atorvastatin 40–80 mg (preferred)"),
("High drug-interaction risk (calcineurin inhibitors, azoles, HIV PIs)", "MODERATE",
"Pravastatin or Pitavastatin"),
("Ischaemic HFrEF, not already on statin", "MODERATE (consider)",
"Rosuvastatin 5–10 mg"),
("Dialysis", "NOT routinely started",
"Continue if previously initiated"),
]
rows = [hdr]
for sit, inten, agent in data_rows:
if "HIGH" in inten and "NOT" not in inten:
ip = Paragraph(f'<b>{inten}</b>', ps("iph", fontSize=7.5, fontName="Helvetica-Bold",
alignment=TA_CENTER, textColor=C_HIGH, leading=10))
bg = C_HIGH_LT
elif "MODERATE" in inten:
ip = Paragraph(f'<b>{inten}</b>', ps("ipm", fontSize=7.5, fontName="Helvetica-Bold",
alignment=TA_CENTER, textColor=C_MOD, leading=10))
bg = C_MOD_LT
else:
ip = Paragraph(inten, ps("ipn", fontSize=7.5, fontName="Helvetica",
alignment=TA_CENTER, textColor=C_LOW, leading=10))
bg = C_LOW_LT
rows.append([P(sit), ip, P(agent)])
t = Table(rows, colWidths=cw, repeatRows=1)
style = base_style()
# Colour intensity column cells per row
for i, (_, inten, _) in enumerate(data_rows, start=1):
if "HIGH" in inten and "NOT" not in inten:
style.append(("BACKGROUND", (1, i), (1, i), C_HIGH_LT))
elif "MODERATE" in inten:
style.append(("BACKGROUND", (1, i), (1, i), C_MOD_LT))
else:
style.append(("BACKGROUND", (1, i), (1, i), C_LOW_LT))
t.setStyle(TableStyle(style))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# TABLE 5: LDL-C Targets (2026 Guideline)
# ═══════════════════════════════════════════════════════════════════════════════
def table5():
cw = [usable_w*0.55, usable_w*0.45]
hdr = [PH("Risk Category"), PH("LDL-C Target")]
rows_data = [
("Very high-risk ASCVD (multiple events or 1 event + high-risk conditions)", "<b><font color='#c0392b'><55 mg/dL</font></b>"),
("High-risk ASCVD / CAC ≥1,000 AU", "<b><font color='#c0392b'><55 mg/dL</font></b> (or ≥50% reduction)"),
("High 10-yr risk (≥10%) or CAC 100–999 AU", "<b><font color='#e67e22'><70 mg/dL</font></b>"),
("Primary prevention, high risk (10-yr ≥10%)", "<b><font color='#e67e22'><70 mg/dL</font></b> (Class IIa)"),
("Intermediate risk / on statin therapy", "<b><font color='#1a7a8a'><100 mg/dL</font></b>"),
("Borderline risk (3–<5%), if treatment chosen", "<b><font color='#1a7a8a'><100 mg/dL</font></b>"),
("LDL-C ≥190 on statin alone (LDL-C still >100)", "Add non-statin therapy"),
]
data = [hdr] + [[P(r), Paragraph(t, cell_center)] for r, t in rows_data]
t = Table(data, colWidths=cw, repeatRows=1)
t.setStyle(TableStyle(base_style()))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# TABLE 6: Non-statin Add-on
# ═══════════════════════════════════════════════════════════════════════════════
def table6():
cw = [usable_w*0.52, usable_w*0.48]
hdr = [PH("Situation (on maximally tolerated statin)"), PH("Add-on Agent")]
rows_data = [
("Very high-risk ASCVD + LDL-C ≥70 mg/dL", "Ezetimibe first → then PCSK9 inhibitor"),
("LDL-C ≥190 mg/dL, LDL-C still >100 on statin", "Ezetimibe → PCSK9 inhibitor or bile acid sequestrant"),
("ACS + LDL-C ≥70 mg/dL (Class I)", "Ezetimibe or PCSK9 inhibitor"),
("Familial hypercholesterolaemia (homozygous)", "Lomitapide, mipomersen, or LDL apheresis"),
]
data = [hdr] + [[P(r), P(a)] for r, a in rows_data]
t = Table(data, colWidths=cw, repeatRows=1)
t.setStyle(TableStyle(base_style()))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# TABLE 7: Muscle Symptom Management
# ═══════════════════════════════════════════════════════════════════════════════
def table7():
cw = [usable_w*0.25, usable_w*0.75]
hdr = [PH("Presentation"), PH("Management Steps")]
rows_data = [
("Mild–moderate muscle pain",
"1. Stop statin 2. Wait for resolution 3. Rechallenge with lower dose or different statin 4. Uptitrate as tolerated"),
("Severe pain or weakness",
"1. Stop statin 2. Check CK, creatinine/GFR, urine myoglobin 3. Admit + hydrate if CK >10× ULN with renal impairment 4. Evaluate predisposing factors 5. Refer to lipidologist before restarting"),
("Jaundice or AST/ALT >5× ULN",
"1. Stop statin 2. Evaluate for other hepatitis causes 3. Reinitiate once resolved"),
("New-onset diabetes",
"Continue statin. Encourage lifestyle modification. Treat diabetes."),
]
data = [hdr] + [[P(r), P(a)] for r, a in rows_data]
t = Table(data, colWidths=cw, repeatRows=1)
t.setStyle(TableStyle(base_style()))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# Clinical Pearls box
# ═══════════════════════════════════════════════════════════════════════════════
def pearls_box():
pearls = [
("⚠", "CONTRAINDICATED in pregnancy and lactation (Category X). Counsel all women of childbearing potential."),
("⚠", "Simvastatin 80 mg is no longer recommended (FDA restriction — myopathy risk). Max 40 mg; consider switching."),
("ℹ", "Diabetes risk: statins accelerate diabetes onset by ~2 months in predisposed patients. ASCVD benefit far outweighs this risk (CTT meta-analysis, Lancet Diabetes Endocrinol 2024)."),
("ℹ", "CYP3A4 inhibitors (azole antifungals, macrolides, HIV protease inhibitors) increase levels of atorvastatin, simvastatin, lovastatin — use pravastatin or pitavastatin instead."),
("ℹ", "Rosuvastatin dose ≤10 mg in severe CKD (eGFR <30) or patients on cyclosporine."),
("ℹ", "Pitavastatin and pravastatin are preferred in transplant patients (minimal calcineurin inhibitor interaction)."),
("ℹ", ">90% of reported muscle symptoms in statin users are not caused by the statin (nocebo effect significant)."),
("ℹ", "Liver monitoring: routine ongoing AST/ALT not needed if baseline <2× ULN. Statins do NOT cause hepatotoxicity."),
]
cells = []
for icon, text in pearls:
clr = "#c0392b" if icon == "⚠" else "#1a3a5c"
cells.append(Paragraph(
f'<font color="{clr}"><b>{icon}</b></font> {text}',
ps("pearlx", fontSize=7, fontName="Helvetica", leading=9.5, spaceBefore=0)
))
# 2-column layout
mid = (len(cells) + 1) // 2
left_col = cells[:mid]
right_col = cells[mid:]
# pad to equal length
while len(right_col) < len(left_col):
right_col.append(Paragraph("", pearl_style))
rows = [[l, r] for l, r in zip(left_col, right_col)]
col_w = (usable_w - 4*mm) / 2
t = Table(rows, colWidths=[col_w, col_w])
t.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING",(0,0), (-1,-1), 4),
("LINEAFTER", (0,0), (0,-1), 0.4, C_LIGHT_GREY),
]))
# Outer box
outer = Table([[t]], colWidths=[usable_w])
outer.setStyle(TableStyle([
("BOX", (0,0), (-1,-1), 0.8, C_WARN_BRD),
("BACKGROUND", (0,0), (-1,-1), C_WARN),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING",(0,0), (-1,-1), 4),
]))
return outer
# ═══════════════════════════════════════════════════════════════════════════════
# Build story
# ═══════════════════════════════════════════════════════════════════════════════
SP = lambda n=3: Spacer(1, n*mm)
story = []
# ── Page 1 ─────────────────────────────────────────────────────────────────────
story.append(header_block())
story.append(SP(2))
story.append(legend_strip())
story.append(SP(3))
story.append(section_banner("TABLE 1 — Statin Intensity by Drug & Dose"))
story.append(SP(1))
story.append(table1())
story.append(SP(1))
story.append(Paragraph("* Simvastatin 80 mg no longer recommended (FDA restriction). † Doses in parentheses have moderate evidence for that intensity tier.",
note_style))
story.append(SP(3))
story.append(section_banner("TABLE 2 — High-Intensity Statin Quick Reference"))
story.append(SP(1))
story.append(table2())
story.append(SP(1))
story.append(Paragraph("Rosuvastatin is ~2× more potent per mg than atorvastatin, which is ~2× more potent than simvastatin.",
note_style))
story.append(SP(3))
story.append(section_banner("TABLE 3 — Drug Pharmacology Comparison"))
story.append(SP(1))
story.append(table3())
story.append(SP(1))
story.append(Paragraph("BBB = blood-brain barrier; CKD = chronic kidney disease; CYP = cytochrome P450.",
note_style))
# ── Page 2 ─────────────────────────────────────────────────────────────────────
story.append(PageBreak())
story.append(header_block())
story.append(SP(3))
story.append(section_banner("TABLE 4 — Statin Intensity by Clinical Indication"))
story.append(SP(1))
story.append(table4())
story.append(SP(3))
story.append(section_banner("TABLE 5 — LDL-C Treatment Targets (2026 ACC/AHA Guideline)"))
story.append(SP(1))
story.append(table5())
story.append(SP(1))
story.append(Paragraph("CAC = coronary artery calcium; ASCVD = atherosclerotic cardiovascular disease. Class I = strong recommendation.",
note_style))
story.append(SP(3))
story.append(section_banner("TABLE 6 — When to Add Non-Statin Therapy"))
story.append(SP(1))
story.append(table6())
story.append(SP(3))
story.append(section_banner("TABLE 7 — Managing Adverse Effects During Statin Therapy"))
story.append(SP(1))
story.append(table7())
story.append(SP(3))
story.append(section_banner("CLINICAL PEARLS & SAFETY NOTES", color=colors.HexColor("#7d6608")))
story.append(SP(1))
story.append(pearls_box())
story.append(SP(3))
story.append(HRFlowable(width=usable_w, thickness=0.4, color=C_LIGHT_GREY))
story.append(SP(1))
story.append(Paragraph(
"Sources: Goldman-Cecil Medicine International Edition (Ch. 190) · Goodman & Gilman's Pharmacological Basis of Therapeutics (Ch. 37) · "
"Washington Manual of Medical Therapeutics (Table 3-10) · Henry's Clinical Diagnosis & Management by Laboratory Methods (Table 18.9) · "
"2026 ACC/AHA/AACVPR Dyslipidemia Guideline (Blumenthal et al., JACC/Circulation 2026, PMID 41824590) · "
"CTT Collaboration, Lancet Diabetes Endocrinol 2024 (PMID 38554713) · Banach et al., Mayo Clin Proc 2025 (PMID 40126455)",
source_style
))
doc.build(story)
print("PDF generated:", OUTPUT)
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Guidelines for using antiplatelet drugs in pad case
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.