Fundamentals of forensic medical procedure, its organization and structure; forensic medical thanatology - dying and death, forensic medical classification of death, corpse events, determination of the post mortem interval;
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from the textbooks. Let me compile the full, detailed answer.
Forensic Medical Thanatology: A Comprehensive Guide
Sources: The Essentials of Forensic Medicine and Toxicology, 36th ed. (2026); P.C. Dikshit Textbook of Forensic Medicine and Toxicology; Parikh's Textbook of Medical Jurisprudence
Part 1: Fundamentals of Forensic Medicine - Organization and Structure
Definitions and Branches
Forensic Medicine (Latin: forensic = of or used in courts of law) is the application of medical and paramedical knowledge to aid in the administration of justice. It is used by legal authorities for the solution of legal problems - injuries, murder, suicide, accidents, sexual offences, poisoning, etc. In short, it deals with the medical aspects of law.
The field has several distinct sub-disciplines:
| Branch | Definition |
|---|---|
| Forensic Medicine | Application of medical knowledge to legal problems |
| Clinical Forensic Medicine | Medicolegal examination of living persons involved in violence or other legally relevant events |
| Forensic Pathology | Study of effects of violence or unnatural disease on the body; determining cause and manner of death in violent, suspicious, unexplained, unexpected, sudden, or medically unattended deaths |
| Medical Jurisprudence (juris = law; prudentia = knowledge) | Legal responsibilities of physicians - negligence, consent, rights and duties, professional misconduct, medical ethics |
| State Medicine | Legal aspects of medical practice: regulation of professionals, medical education standards, community and environmental health |
| Medical Ethics | Moral principles guiding members of the medical profession in their dealings with each other, patients, and the State |
Historical Development
The interface of medicine and law dates to antiquity:
- ~3000 BC: Law-medicine problems in Egypt, Sumer, Babylon, India and China; Chinese Materia Medica contains information on poisons
- ~2200 BC: Code of Hammurabi (oldest known medicolegal code)
- 7th century BC: Charaka Samhita - duties of physicians and classification of poisons
- 4th-3rd century BC: Arthashastra of Kautilya - examination of dead bodies in unnatural deaths; Manu Smriti - mental incapacity due to intoxication
- 460-377 BC: Hippocrates discussed lethality of wounds
- 200-300 AD: Sushruta Samhita - wounds, fractures, poisons classified
- 6th century AD: Justinian Code - established function of the medical expert for legal procedure
Part 2: Forensic Medical Thanatology
Thanatology (Greek: thanatos = death) is the branch of science dealing with death in all its aspects, including the changes that occur with and after death.
2.1 Dying and Death - Definitions
The definition of death posed little problem for centuries until organ transplantation in the 1960s demanded precise scrutiny.
Key Legal and Medical Definitions:
- Section 2(6) Bharatiya Nyaya Sanhita / Section 46 IPC: Death denotes the death of a human being unless the contrary appears from the context.
- Registration of Births and Deaths Act, 1969, Section 2(b): Death = permanent disappearance of all evidence of life at any time after live birth has taken place.
- Black's Law Dictionary (1951): "The cessation of life, the ceasing to exist" - defined by physicians as total stoppage of circulation and cessation of vital functions such as respiration and pulsation.
- Shapiro (1969): The irreversible loss of the properties of living matter.
- Rentoul and Smith (1973): Complete and persistent cessation of respiration and circulation.
- Calne (1970): When destruction of the brain has been established, the individual has died - regardless of the state of the rest of the body.
The living body depends on three principal interdependent systems: circulation, respiration, and enervation (nervous system). Failure of any one of these ultimately causes the other two to fail.
2.2 Forensic Medical Classification of Death
A. Somatic (Clinical/Systemic) Death
This is the irreversible cessation of the integrated functioning of the organism as a whole - the failure of the three core systems (circulation, respiration, central nervous system). This is the legal definition of death.
Signs of somatic death:
- Insensibility and loss of voluntary movement - the earliest sign; must be interpreted with caution (may occur in epilepsy, trance, narcosis, vagal inhibitory phenomenon, electrocution)
- Cessation of respiration - must be complete and continuous; >5 minutes usually causes death; confirmed by stethoscope over lungs/larynx; historical tests (feather, mirror, Winslow's) are now obsolete
- Cessation of circulation - stethoscope over precordial area; >5 minutes stoppage accepted as evidence of death; Magnus test, Icard's test, diaphanous test have historical interest only
B. Molecular (Cellular) Death
Occurs 1-2 hours after somatic death. Tissues die individually depending on their metabolic activity and tolerance to anoxia:
| Tissue | Survival after somatic death |
|---|---|
| Vital centers of brain | ~5 minutes |
| Neurons generally | Minutes to ~30 min |
| Muscles (mechanical excitability) | 1-2 hours (Zasko's phenomenon) |
| Pupil reaction to atropine (dilatation) | Up to 4 hours |
| Pupil reaction to eserine (contraction) | Up to 1 hour |
| Cornea (transplantable) | Up to 6 hours |
| Blood (transfusable) | Up to 6 hours |
This has immense significance for organ transplantation: there is a narrow window after somatic death when tissues still have biological viability. As Dikshit notes: "We die in bits and pieces."
C. Brain Death
Defined as the irreversible cessation of all functions of the entire brain, including the brainstem.
Calne's criteria (1970):
- Deep, irreversible coma with fixed, dilated pupils and absent cranial nerve reflexes
- No spontaneous respiration
- Absence of electrical brain activity (flat EEG)
- Cessation of circulation through the retina
Cortical death: Loss of higher cerebral functions while brainstem continues to function - the "persistent vegetative state."
Brainstem death: Cessation of all brainstem functions (respiratory center, cardiovascular regulation, cranial nerve reflexes) - the UK standard for legal death.
D. Suspended Animation
A death-like state where vital functions are at such a low pitch they cannot be detected by ordinary clinical examination.
Causes: severe shock following accident, electrical shock, barbiturate poisoning, drowning in cold water, hypothermia, yoga practitioners (voluntary). Importantly, this is NOT death.
2.3 Classification of Death by Manner
| Category | Description |
|---|---|
| Natural | Due to disease, aging, natural causes |
| Violent/Unnatural | Due to external causes: homicide, suicide, accident |
| Sudden Death | Unexpected death in a previously healthy-appearing person |
| Suspicious/Unknown | Requires medico-legal investigation |
ICD-11 Causal Sequence for Cause of Death:
- Immediate cause - final disease/injury directly leading to death
- Intermediate cause(s) - linking conditions in sequence
- Underlying cause - disease/event initiating the chain (this is the ICD-11 coded cause)
- Other contributing conditions - not part of the direct causal chain
Example: Septicemia (immediate) → Extensive burns (intermediate) → Assault by burning in a dowry case (underlying) → ICD-11 code PK80.1.
Part 3: Corpse Events (Postmortem Changes)
Forensic Taphonomy is the interdisciplinary study of postmortem biological changes of human remains in the dispositional context - the chronological changes following death.
Sequential Postmortem Changes
| Stage | Key Changes |
|---|---|
| Immediate (somatic death) | Insensibility, loss of voluntary power; cessation of respiration; cessation of circulation |
| Early (cellular death) | Pallor and loss of elasticity of skin; changes in the eye; primary flaccidity of muscles; algor mortis; livor mortis; rigor mortis |
| Late (decomposition/decay) | Putrefaction; adipocere formation; mummification |
3.1 Algor Mortis (Postmortem Cooling)
After death, body temperature falls as heat is lost by conduction, convection, and radiation - called algor mortis (dead body chill).
Physiological basis: After circulation stops, convectional heat transport inside the body stops. Residual heat is produced briefly by glycogenolysis in dying tissues and intestinal bacterial metabolism, causing an initial plateau. Heat then flows by conduction from core to surface.
Postmortem Cooling Pattern:
- First 0.5-1 hour: Temperature falls little or not at all (isothermic/plateau phase)
- Next 12-16 hours: Linear cooling at ~0.4-0.6°C per hour
- Thereafter: Cooling rate slows as body approaches ambient temperature
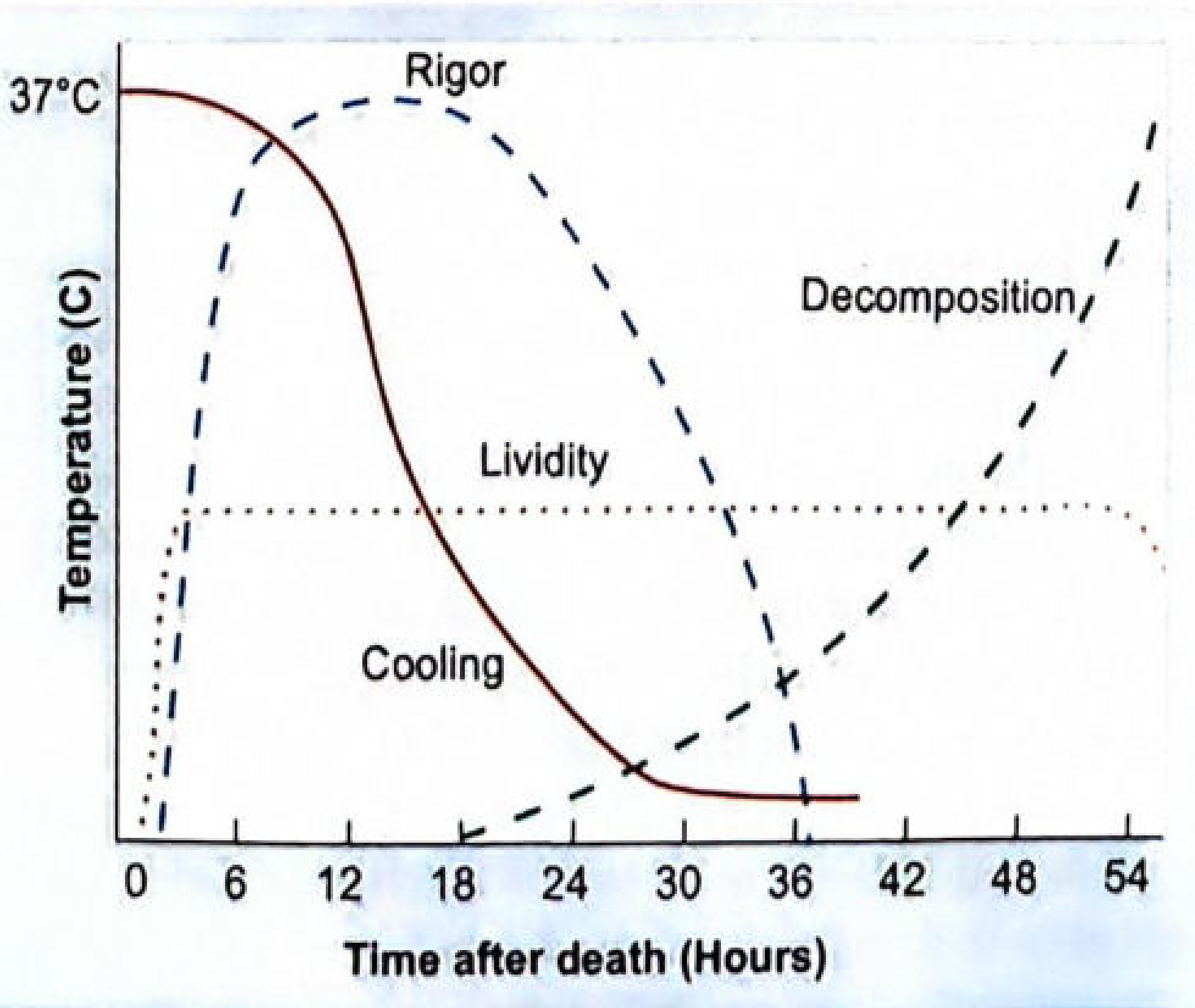
Fig: The major postmortem changes plotted against time. Cooling follows a sigmoid curve from 37°C. Rigor peaks around 12-18 hours then resolves by ~36 hours. Lividity begins in the first few hours. Decomposition begins after rigor resolves.
Factors accelerating cooling: thin build, wet clothing, cold/windy environment, prior fever resolving, low ambient temperature.
Factors slowing cooling: obesity, warm/humid environment, thick clothing, high ambient temperature.
PMI estimation formula (Henssge nomogram): Uses rectal temperature, ambient temperature, and body weight.
3.2 Livor Mortis (Postmortem Lividity / Hypostasis)
Also called: postmortem staining, livor mortis, cadaveric lividity, suggillations, vibices, subcutaneous hypostasis.
Mechanism: After circulation stops, blood stagnates and sinks by gravity into the dependent capillaries and venules, producing a bluish-purple discoloration of the overlying skin.
Development Timeline (Mallach's data):
| Stage | Lower limit (HPM) | Upper limit (HPM) |
|---|---|---|
| Beginning | 0.25 hrs | 3 hrs |
| Confluence | 1.0 hr | 4 hrs |
| Maximum | 3.0 hrs | 16 hrs |
| Thumb pressure blanches | 1.0 hr | 20 hrs |
| Complete shifting (on repositioning) | 2.0 hrs | 6 hrs |
| Incomplete shifting | 4.0 hrs | 24 hrs |
HPM = hours postmortem
Forensic significance:
- Position: Lividity is fixed in the dependent parts - inconsistency with the position of the body suggests the body was moved
- Shifting: If the body is repositioned within the first 6-8 hours, lividity will shift; after 8-12 hours it becomes fixed
- Color provides important clues: cherry-red (CO poisoning), bright pink (cyanide, hypothermia), brown/chocolate (methemoglobin-forming poisons), dark purple (asphyxia)
3.3 Rigor Mortis
Stiffening of muscles after death due to failure of the ATP-dependent actin-myosin relaxation cycle.
Biochemical basis: After death, ATP production ceases. Actin-myosin cross-bridges cannot be broken, causing irreversible muscle contraction. Lactic acid accumulation also contributes to the stiffening.
Sequence: Rigor starts in the small muscles of the eyelids and face, progresses to the neck, trunk, and upper limbs, then lower limbs (Nysten's law - in order of small to large muscle groups). It resolves in the same order as decomposition sets in.
Timeline (temperate conditions):
- Onset: 2-6 hours after death
- Complete/maximum: 12 hours
- Begins to pass off: 24-36 hours
- Completely resolved: 36-48 hours
Special forms:
- Cadaveric spasm (Instantaneous rigor): Immediate stiffening at the moment of death, without primary flaccidity - seen in violent deaths (drowning, gunshot, wounds). The hand may grip an object at the time of death, important forensic evidence.
- Cold stiffening: Freezing of tissues in cold environments - not true rigor; resolves on warming.
- Heat stiffening: Seen in burning deaths - due to protein coagulation; does not resolve.
3.4 Changes in the Eyes
- Corneal clouding: Begins within 1-2 hours; fully cloudy by 12-24 hours (faster without eyelids closed)
- Tache noire sclérotique: Black/brown patches on the sclera at the exposed portions when eyelids are open - due to drying
- Flattening of the eyeball: Due to intraocular pressure loss
- Kayser-Fleischer-like ring: Loss of fundus reflex
- Vitreous potassium: Rises predictably at ~1.6 mmol/L per 10 hours - used for PMI estimation in later stages
3.5 Putrefaction (Decomposition)
Decomposition of soft tissues through microbial action.
Sequence:
- Fresh stage - somatic death to onset of decomposition
- Bloat - gas accumulation (H₂S, methane, CO₂) by intestinal bacteria; abdomen distends; skin turns greenish-brown, starting at the right iliac fossa (caecum)
- Active decay - tissue liquefaction; strong odor; skin slippage
- Advanced decay / Skeletonization
Casper's dictum on rate of decomposition:
"If all conditions are equal, a body decomposes twice as fast in air as in water, and eight times as fast in water as in earth."
Factors affecting decomposition rate: temperature (main factor - warmth accelerates, cold retards), humidity, access by insects (entomology), depth of burial, clothing, body composition.
3.6 Special Postmortem Changes
Adipocere (Saponification): Transformation of body fat into a soapy, waxy substance (hydroxy fatty acids) in moist, warm, anaerobic environments. Begins in 3 weeks; preserves body contours for years. Important for long-term PMI estimation and identification.
Mummification: Desiccation of body tissues in hot, dry, arid conditions with good air circulation. Skin becomes hard, dry, brownish-black parchment-like. Body contours preserved. Seen in deserts, attics, enclosed coffins.
Part 4: Determination of the Postmortem Interval (PMI)
The postmortem interval (PMI) is the time elapsed since death - the central question in forensic thanatology.
Methods for PMI Estimation
Stage 1: Early PMI (0-24 hours) - Temperature-Based
Algor Mortis (Rectal Temperature Method):
- Henssge Nomogram is the gold standard
- Formula basis: PMI ≈ (37 - rectal temperature) / cooling rate
- The cooling rate depends on body weight and environmental temperature
- Accuracy: ±2.8 hours (95% confidence interval in ideal conditions)
Stage 2: Early-Mid PMI - Postmortem Changes (Integrated Assessment)
| Change | Approximate timing |
|---|---|
| Pallor of skin | Minutes |
| Algor mortis begins | ~30 min |
| Livor mortis visible | 30 min - 3 hrs |
| Livor mortis fixed | 8-12 hrs |
| Rigor mortis begins | 2-6 hrs |
| Rigor mortis complete | ~12 hrs |
| Rigor mortis resolves | 36-48 hrs |
| Early putrefaction (greenish discoloration) | ~24-48 hrs (temperate climate) |
Stage 3: Mid-Late PMI - Biochemical Methods
| Marker | Specimen | Application |
|---|---|---|
| Vitreous potassium (K⁺) | Vitreous humor | Most reliable chemical method; ~1.6 mmol/L per 10 hours after death |
| Vitreous sodium, chloride | Vitreous humor | Supplementary |
| CSF potassium | Cerebrospinal fluid | Less reliable than vitreous |
| Creatinine, urea | Vitreous | Supplementary |
| Hypoxanthine | Vitreous | Useful in first 24-72 hours |
Why vitreous humor? The vitreous is isolated from rapid decomposition and contamination, making it the most stable and reliable postmortem biochemical specimen.
Stage 4: Late PMI - Entomology and Botanical Evidence
- Forensic entomology: Succession of insect species on the corpse follows predictable patterns. The development stage of blowfly (Calliphora, Lucilia spp.) larvae is the most useful - minimum PMI can be calculated from the oldest larval stage.
- Botanical evidence: Root growth through skeletal remains, pollen analysis
- Skeletal analysis: Bone weathering stages for long-term PMI (months to years)
Factors Affecting Accuracy of PMI Estimation
- Environmental temperature (most important)
- Humidity and air circulation
- Clothing and body covering
- Body size and composition
- Cause of death (fever at time of death elevates starting temperature; hypothermic deaths may lower it)
- Site of discovery (shaded vs. sun-exposed; water vs. soil)
Summary Table: Forensic PMI Timeline
| PMI | Key Finding(s) |
|---|---|
| 0-30 min | Pallor, flaccidity, cessation of vital signs |
| 30 min - 3 hrs | Early lividity appears; body begins cooling |
| 2-6 hrs | Rigor mortis begins; corneal clouding |
| 8-12 hrs | Lividity fixed; rigor complete |
| 12-16 hrs | Body at near-ambient temperature |
| 24-36 hrs | Rigor begins to resolve; early putrefaction signs |
| 36-48 hrs | Rigor fully resolved; greenish discoloration present |
| >48 hrs | Progressive putrefaction; insect activity |
| Weeks-months | Adipocere/mummification; skeletonization |
Key textbook references:
- The Essentials of Forensic Medicine and Toxicology, 36th ed. (2026) - Chapters 1 and 7
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology - Chapters on Thanatology (pp. 44-49)
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology - Chapters 11-12
This is a shared conversation. Sign in to Orris to start your own chat.