Occular tb full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ocular tuberculosis" diagnosis treatment
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive information. Let me compose the full MD exam answer:
Ocular Tuberculosis — Complete MD Exam Answer (15 Marks)
1. Introduction & Epidemiology
Tuberculosis (TB) is a chronic granulomatous infection caused by Mycobacterium tuberculosis (rarely M. bovis or atypical mycobacteria such as M. avium in immunocompromised patients). TB is primarily a pulmonary disease but spreads haematogenously to extrapulmonary sites — ocular involvement commonly occurs without clinically overt systemic disease, making it a great imitator. Immune deficiency (HIV, diabetes, malnutrition, immunosuppressive therapy) is a major risk factor.
2. Pathogenesis
Two mechanisms operate:
| Mechanism | Description |
|---|---|
| Direct infection | Haematogenous seeding of uveal tissue (choroid most vascular) → granuloma formation with caseating necrosis |
| Hypersensitivity | Immune-mediated reaction to mycobacterial antigens — explains many anterior uveitis episodes, phlyctenulosis, serpiginoid choroiditis, and possibly Eales disease |
3. Ocular Manifestations (Site-by-Site)
A. Eyelids
- Lupus vulgaris — reddish-brown nodules; a form of cutaneous TB
B. Conjunctiva
- Conjunctivitis — granulomatous, with associated preauricular lymphadenopathy (Parinaud oculoglandular syndrome)
- Phlyctenulosis — hypersensitivity-mediated; small, nodular, limbal or corneal lesions with intense injection; classic in children
C. Cornea
- Interstitial keratitis — stromal haze, vascularisation; less common than syphilis but well-documented
- Marginal ulcers (hypersensitivity)
D. Sclera
- Scleritis (anterior or posterior) — nodular or diffuse; can be necrotising
E. Anterior Uvea (Most Common Segment in TB Uveitis)
- Usually granulomatous anterior uveitis
- Mutton-fat keratic precipitates (KPs) on corneal endothelium
- Iris nodules (Koeppe at pupil margin, Busacca in iris stroma)
- Broad posterior synechiae (PS), peripheral anterior synechiae
- Secondary glaucoma, complicated cataract
F. Vitreous
- Viritis — very common; may be secondary to anterior, intermediate, or posterior primary foci
- Snowballs, snowbanking
- Macular complications: cystoid macular oedema (CMO), epiretinal membrane
G. Choroid (Most Characteristic Posterior Segment Lesion)
- Choroidal granuloma (tubercle) — focal, elevated, dome-shaped yellowish lesion; unilateral or bilateral; solitary or multiple. A large abscess-like lesion = tuberculoma
- Serpiginoid (multifocal serpiginous-like) choroiditis — multifocal lesions spreading centrifugally; tracking retinal vessels has reasonable specificity for TB; distinguished from true serpiginous choroiditis by distribution and response to ATT
- Miliary choroidal tubercles — pathognomonic of miliary TB; multiple tiny bilateral choroidal lesions; vital sign on ophthalmoscopy in suspected miliary TB
H. Retina & Retinal Vasculitis
- Retinal vasculitis, preferentially venous (periphlebitis/sheathing of retinal veins)
- Retinal haemorrhages
- Vascular occlusion → branch retinal artery/vein occlusion → extensive ischaemia
- Pre-retinal and disc neovascularisation (NVI/NVE) → vitreous haemorrhage
- Eales disease — recurrent vitreous haemorrhage in young males from idiopathic retinal periphlebitis; TB hypersensitivity is a leading aetiological hypothesis
- Exudative retinal detachment
I. Optic Nerve
- Optic neuritis / neuroretinitis — may be direct infiltration or para-infectious
- Optic atrophy (late)
4. Fundus Images (Kanski's Clinical Ophthalmology)
Fig. A — Choroidal granuloma (Tubercle): Solitary dome-shaped yellowish elevated lesion in posterior pole.
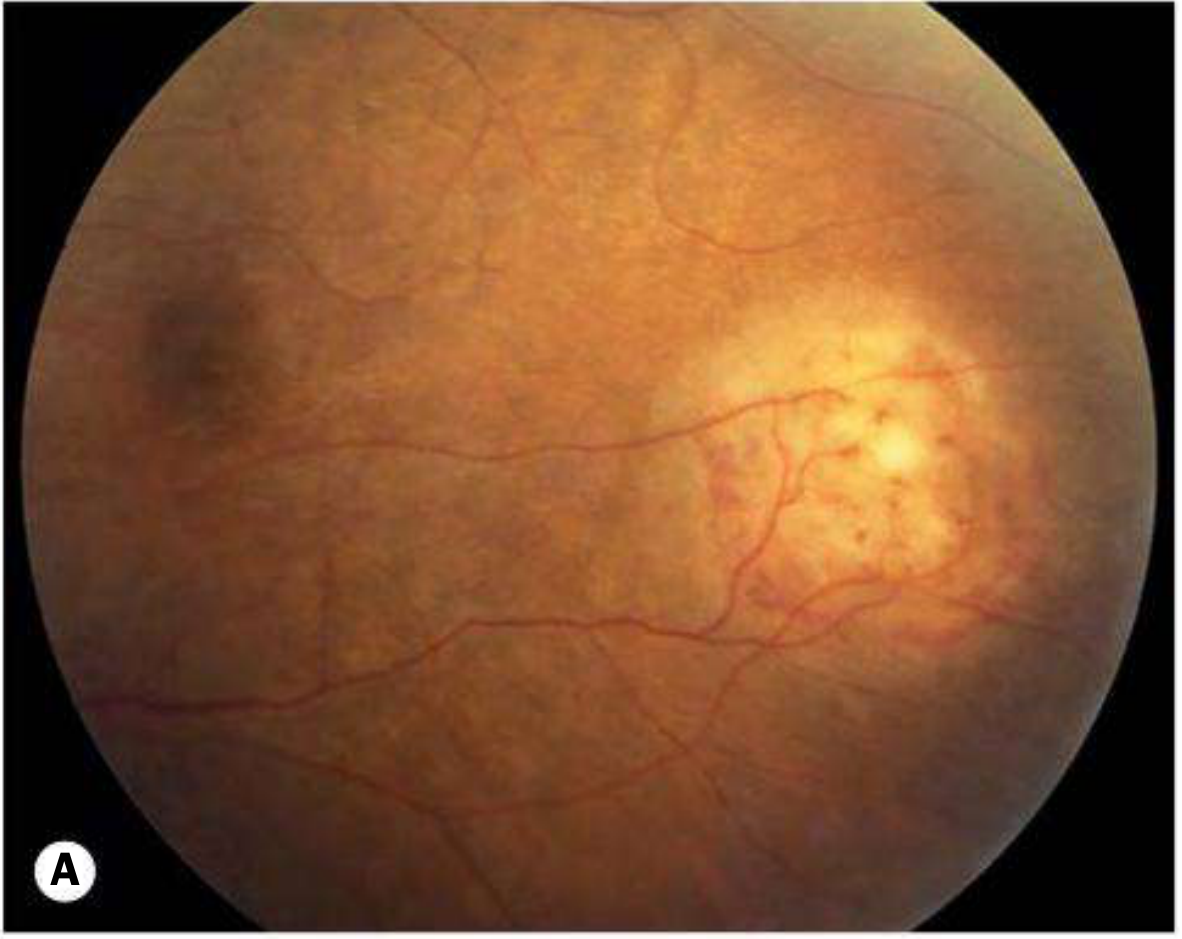
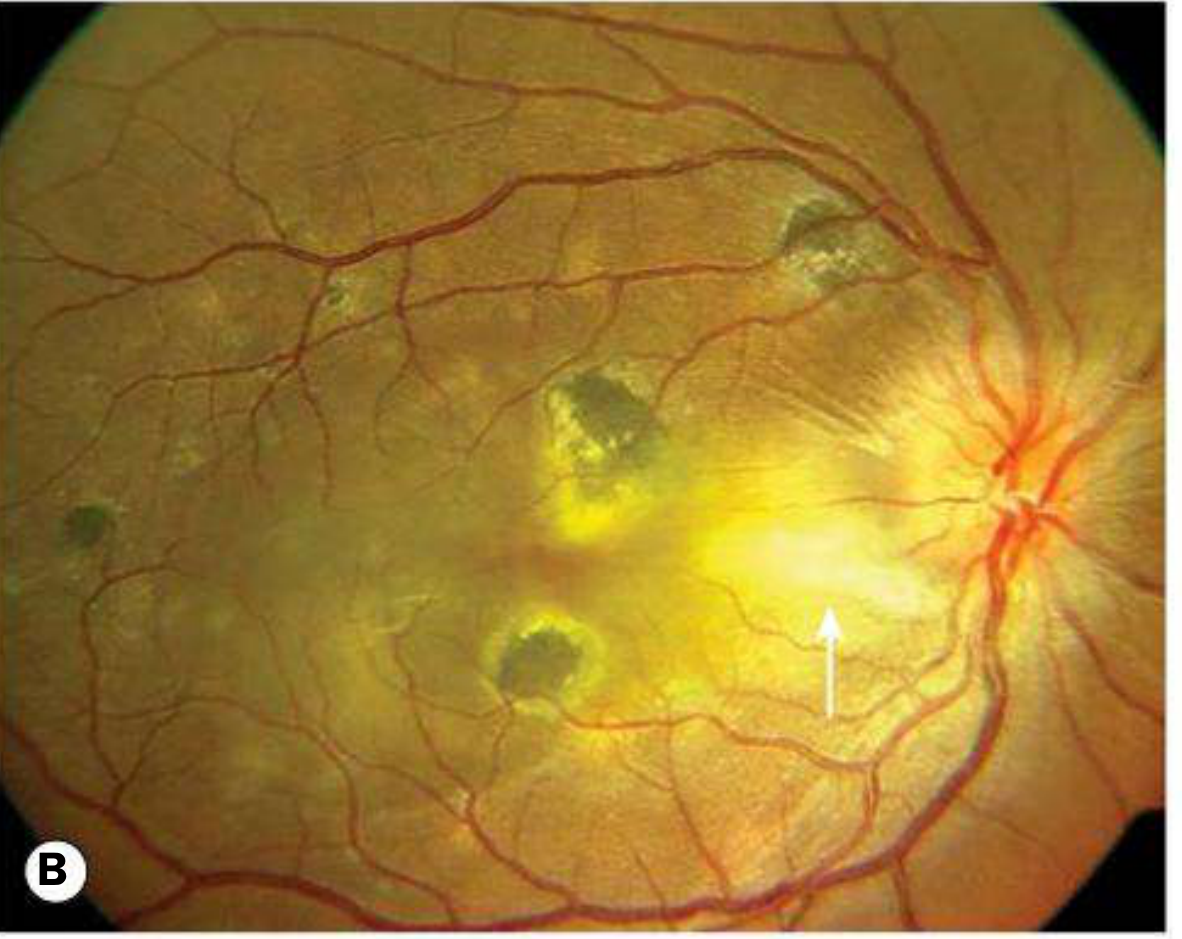
Fig. B — Active multifocal choroidal TB: Multiple pale-yellow lesions with arrow indicating confluent active foci; overlying exudate and disc oedema.
5. Diagnosis
Diagnosis of ocular TB is often clinical — based on clinical picture + evidence of TB exposure or latency + exclusion of other causes. A formal systemic assessment by an appropriate specialist is mandatory.
Systemic Investigations
| Test | Details |
|---|---|
| Tuberculin skin test (Mantoux) | Positive ≥48h; false-negatives in anergy (HIV, malnutrition); false-positives with BCG |
| IGRA — Interferon-Gamma Release Assay (QuantiFERON-TB Gold) | ~80% sensitivity in active disease; independent of BCG vaccination; preferred in BCG-vaccinated populations |
| T-SPOT.TB | Counts antimycobacterial effector T cells producing IFN-γ; can detect latent TB; sensitivity 81%, specificity 86% |
| Sputum — AFB smear + culture | Ziehl-Neelsen staining; Löwenstein-Jensen medium; PCR |
| Chest X-ray | Primary complex, Ghon's focus, apical fibronodular lesions, hilar lymphadenopathy |
| CT / PET-CT | Mediastinal nodes, pulmonary cavities, extrapulmonary TB |
| HIV status | Must be determined in all patients |
Ocular Investigations
| Test | Details |
|---|---|
| Aqueous/vitreous sampling | AFB smear + ZN stain; culture on Löwenstein-Jensen; PCR (highly specific, variable sensitivity — gold standard for ocular fluid) |
| Fundus fluorescein angiography (FFA) | Establishes choroidal activity; confirms preretinal NV; demonstrates ischaemia |
| Fundus autofluorescence (FAF) | Activity staging — lesions become progressively hypoautofluorescent with healing |
| OCT | Macular evaluation — CMO, subretinal fluid, ERM |
| B-scan ultrasonography | Posterior scleritis, choroidal thickening, retinal detachment |
Diagnostic criteria (Gupta et al. / SUN Workshop): Probable ocular TB = compatible ocular lesion + positive IGRA/TST + evidence of systemic TB (radiological or biopsy) + no alternative diagnosis. Confirmed = direct demonstration of AFB or positive PCR/culture from ocular fluids.
6. Treatment
Anti-Tubercular Therapy (ATT)
Prolonged multi-drug therapy, prescribed and monitored by a specialist with experience in systemic TB management.
Standard regimen (WHO):
- Intensive phase (2 months): Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) — 2HRZE
- Continuation phase (4–10 months): Isoniazid + Rifampicin — 4HR (extrapulmonary TB often treated for 9–12 months total)
Key drug ocular side effects:
- Ethambutol → optic neuropathy (monitor visual acuity, colour vision, fields regularly)
- Rifabutin (used in HIV co-infection in place of rifampicin) → anterior uveitis (often hypopyon)
- Isoniazid → optic neuritis (rare); supplement pyridoxine (B6)
Role of Corticosteroids
- Topical steroids: for anterior segment inflammation (cycloplegia also for posterior synechiae prevention)
- Systemic steroids: used concomitantly with ATT to reduce inflammation-induced damage, particularly in early weeks when paradoxical worsening of fundal appearance may occur
- Must NEVER be given without ATT cover
- Especially indicated for: optic neuritis, extensive choroiditis, CMO, exudative RD, orbital TB
Additional Ocular Treatment
| Indication | Treatment |
|---|---|
| Posterior synechiae | Cycloplegics (atropine) + topical steroids |
| Raised IOP / secondary glaucoma | IOP-lowering agents; trabeculectomy if refractory |
| Retinal neovascularisation | Laser photocoagulation to ischaemic retina |
| Vitreous haemorrhage | Observation → vitrectomy if non-clearing |
| Cataract | Phacoemulsification after inflammation controlled |
Evidence Update
Treatment with ATT in patients with uveitis associated with latent TB halves the risk of uveitis recurrence and delays first recurrence onset. (Kanski's 10th edition)
7. Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Sarcoidosis | ACE level, serum lysozyme, bilateral hilar adenopathy; "candle wax" retinal periphlebitis |
| Syphilis | Serological tests (VDRL, TPHA, FTA-ABS) |
| Toxoplasmosis | Focal retinochoroiditis adjacent to scar; IgG/IgM serology |
| Serpiginous choroiditis (idiopathic) | Geographic spread from disc, no response to ATT |
| Eales disease | Young males, peripheral retinal periphlebitis, vitreous haemorrhage; IGRA positive in many |
| Viral uveitis (CMV, HSV, VZV) | Viral serology; aqueous PCR |
| Lymphoma (PVRL) | Vitreous biopsy; IL-10/IL-6 ratio |
8. Complications
- Complicated cataract (steroid-induced or inflammatory)
- Secondary glaucoma (trabecular blockage, posterior synechiae → seclusio pupillae → iris bombé)
- Macular scarring, CMO → permanent visual loss
- Retinal detachment (exudative or tractional)
- Vitreous haemorrhage → opacification
- Phthisis bulbi (end-stage)
- Optic atrophy
9. Summary Table — Ocular TB at a Glance
| Feature | Key Points |
|---|---|
| Organism | M. tuberculosis (rarely M. bovis, atypical mycobacteria) |
| Mechanism | Haematogenous spread + hypersensitivity |
| Most common segment | Posterior (choroid) in developing countries; anterior (uveitis) also very common |
| Pathognomonic sign | Miliary choroidal tubercles (in miliary TB) |
| Specific posterior sign | Serpiginoid choroiditis tracking retinal vessels |
| Diagnostic test of choice (ocular fluid) | PCR for M. tuberculosis |
| Systemic test (preferred in BCG-vaccinated) | IGRA (QuantiFERON-TB Gold) |
| Treatment duration | Minimum 9 months (ATT) |
| Dangerous drug side effect | Ethambutol optic neuropathy; Rifabutin uveitis |
| Steroids | Use WITH ATT cover only |
References:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition, pp. 497–500
- Wills Eye Manual, 8th Edition — Retinal Periphlebitis / Uveitis sections
- Tintinalli's Emergency Medicine — Miliary TB, Choroidal Tubercles
This is a shared conversation. Sign in to Orris to start your own chat.