1. Umnl vs lmnl 2. Thrombotic vs embolic vs hemorrhagic stroke (HOPI, Clinical features, signs) 3. Corticospinal tract pathway and it's lesions 4. Facial nerve pathway and it umnl vs lmnl findings
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive answer. Let me compile everything.
1. UMN vs LMN - Complete Comparison
Upper Motor Neuron (UMN)
The UMN refers to any motor neuron that projects from the cortex (precentral gyrus, area 4; premotor cortex, area 6; supplementary motor cortex) down through the CNS to synapse onto the lower motor neuron. This includes the corticospinal tract, corticobulbar tract, and other descending pathways. UMN cell bodies are in the motor cortex; their axons travel through the corona radiata → internal capsule (posterior limb) → cerebral peduncle → pons → medullary pyramid → decussate at pyramidal decussation (85-90%) → lateral corticospinal tract in spinal cord.
Lower Motor Neuron (LMN)
The LMN is the "final common pathway." Cell bodies are in the anterior horn of the spinal cord (for the body) or cranial nerve motor nuclei (for the face/bulbar muscles). Their axons exit via anterior roots/cranial nerves to innervate skeletal muscle directly.
UMN vs LMN - Comparison Table
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness pattern | Groups of muscles (never individual); extensors/abductors of UL, flexors of LL | Individual muscles or myotome supplied by that nerve/root |
| Tone | Increased - spasticity (velocity-dependent, clasp-knife) | Decreased - flaccidity/hypotonia |
| Reflexes (DTR) | Hyperreflexia (may be absent acutely - spinal shock) | Hyporeflexia or areflexia |
| Plantar reflex | Extensor (Babinski sign) | Flexor (normal) or absent |
| Muscle bulk | Preserved (mild disuse atrophy only, late) | Wasting/atrophy (prominent, early) |
| Fasciculations | Absent | Present (spontaneous firing of dying motor units) |
| Fibrillations (EMG) | Absent | Present |
| Superficial reflexes | Absent (abdominal, cremasteric) | Preserved |
| Clonus | Present | Absent |
| Distribution | Hemiplegia, paraplegia, monoplegia | Specific nerve/root territory |
| Cause examples | Stroke, brain tumor, MS, spinal cord compression (above lesion) | Polio, GBS, ALS (LMN component), disc prolapse, peripheral neuropathy |
Sources: Harrison's Principles of Internal Medicine 22E; Adams and Victor's Principles of Neurology 12E; Neuroanatomy through Clinical Cases 3E
Key mnemonic: UMN = Upper = Unable to suppress (hyper-reflexia, hyper-tonia, Babinski). LMN = Lower = Limp, Lost reflexes, wasting.
2. Thrombotic vs Embolic vs Hemorrhagic Stroke
Overview
- Ischemic strokes account for ~87% of all strokes (thrombotic + embolic + hypoperfusion)
- Hemorrhagic strokes account for ~13% (ICH ~10%, SAH ~3%)
- Hemorrhagic stroke has far higher 30-day mortality (~50%, vs ~10% for ischemic)
Thrombotic Stroke
Mechanism: In situ narrowing/occlusion of a vessel lumen - typically from atherosclerotic plaque rupture with superimposed clot formation. Affects large arteries (carotid, MCA, basilar) or small arteries (lacunar).
HOPI (History of Presenting Illness):
- Onset: Gradual, stuttering, stepwise or waxing-and-waning ("stroke in evolution")
- Often occurs during sleep or on waking (decreased BP, sluggish flow)
- May be preceded by TIAs in the same vascular territory (same distribution = vascular disease)
- Slow progression over hours
Risk factors: Hypertension, diabetes mellitus, hypercholesterolaemia, smoking, coronary artery disease, peripheral vascular disease
Clinical features:
- Focal neurological deficit corresponding to affected territory (see vascular syndromes)
- Usually no headache (unlike hemorrhagic)
- No meningismus
- MCA territory most common: contralateral hemiplegia (face + arm > leg), hemisensory loss, homonymous hemianopia, aphasia (dominant) or neglect (non-dominant)
Signs: Signs of chronic atherosclerosis - carotid bruits, reduced peripheral pulses, signs of DM/HTN
Embolic Stroke
Mechanism: Material from a remote source travels and lodges in a cerebral artery. Sources: cardiac (AF, valvular vegetations, mural thrombus post-MI, myxoma), arterial-arterial (proximal plaque), paradoxical (PFO), fat/air emboli, septic emboli (endocarditis).
HOPI:
- Onset: Sudden, maximal at onset ("like a bolt from the blue")
- Patient typically awake and active
- TIAs in different vascular distributions (emboli scatter randomly)
- May have history of atrial fibrillation, recent MI, valvular disease, DVT/PE (paradoxical)
Clinical features:
- Sudden dense neurological deficit
- Seizures at onset (more common than thrombotic - cortical irritation from abrupt ischaemia)
- Headache may occur (especially with haemorrhagic transformation)
- Emboli more commonly affect cortical distribution (wedge-shaped infarcts on imaging)
- Haemorrhagic transformation more likely than thrombotic (emboli fragment/lyse spontaneously, reperfusing ischaemic tissue)
Signs: Irregular pulse (AF), prosthetic valves, cardiac murmur, stigmata of endocarditis (Osler nodes, Janeway lesions, splinter haemorrhages)
Hemorrhagic Stroke
Mechanism: Rupture of a vessel causing blood extravasation - either intracerebral haemorrhage (ICH) (intraparenchymal - usually hypertensive rupture of lenticulostriate arteries in basal ganglia/thalamus/pons/cerebellum) or subarachnoid haemorrhage (SAH) (rupture of berry aneurysm/AVM into subarachnoid space).
HOPI:
- Onset: Sudden, often during exertion or Valsalva (raised intracranial pressure trigger)
- Headache: Present and often severe ("worst headache of life" in SAH - thunderclap headache); ICH also gives headache at onset
- Rapid deterioration in consciousness (raised ICP)
- Nausea and vomiting (raised ICP)
- History of Valsalva (straining, coughing, coitus) preceding SAH
- No preceding TIAs
- Risk factors: Hypertension (ICH), amyloid angiopathy (elderly, lobar ICH), anticoagulant use, AVM, aneurysm
Clinical features (ICH):
- Rapidly progressive focal neurological deficit + decreased LOC
- Headache + vomiting at onset
- Seizures may occur
- Hypertensive signs
Clinical features (SAH):
- Thunderclap headache - sudden onset, maximal immediately
- Meningismus (neck stiffness, Kernig's, Brudzinski's signs)
- Photophobia
- ± Third nerve palsy (posterior communicating artery aneurysm compressing CN III → ptosis, mydriasis, "down and out" eye)
- ± Retinal (subhyaloid) haemorrhages - Terson's syndrome
- Decreased LOC; may present as sudden collapse
Signs: Hypertension, papilloedema, meningismus, focal deficits depending on haematoma location
Quick Comparison Table
| Feature | Thrombotic | Embolic | Hemorrhagic |
|---|---|---|---|
| Onset | Gradual, stuttering | Sudden, maximal at onset | Sudden, often during exertion |
| Activity at onset | Often during sleep/waking | During activity | During activity/exertion |
| Headache | Rare | Sometimes (haemorrhagic transformation) | Prominent (esp. SAH - thunderclap) |
| LOC change | Usually preserved initially | Usually preserved initially | Often reduced (raised ICP) |
| Vomiting | Rare | Rare | Common (raised ICP) |
| Meningismus | Absent | Absent | Present (SAH) |
| Preceding TIAs | Same territory | Different territories | Absent |
| Risk factors | HTN, DM, atherosclerosis | AF, valvular disease, recent MI | HTN, aneurysm, AVM, anticoagulants |
| Seizures | Rare | More common | Possible |
| CSF | Clear | Clear | Xanthochromic / bloody (SAH) |
| CT findings | Hypodense area (may be normal early) | Wedge-shaped cortical infarct | Hyperdense (white) blood |
Sources: Tintinalli's Emergency Medicine; Adams and Victor's Principles of Neurology 12E; Frameworks for Internal Medicine
3. Corticospinal Tract - Pathway and Lesions
Pathway
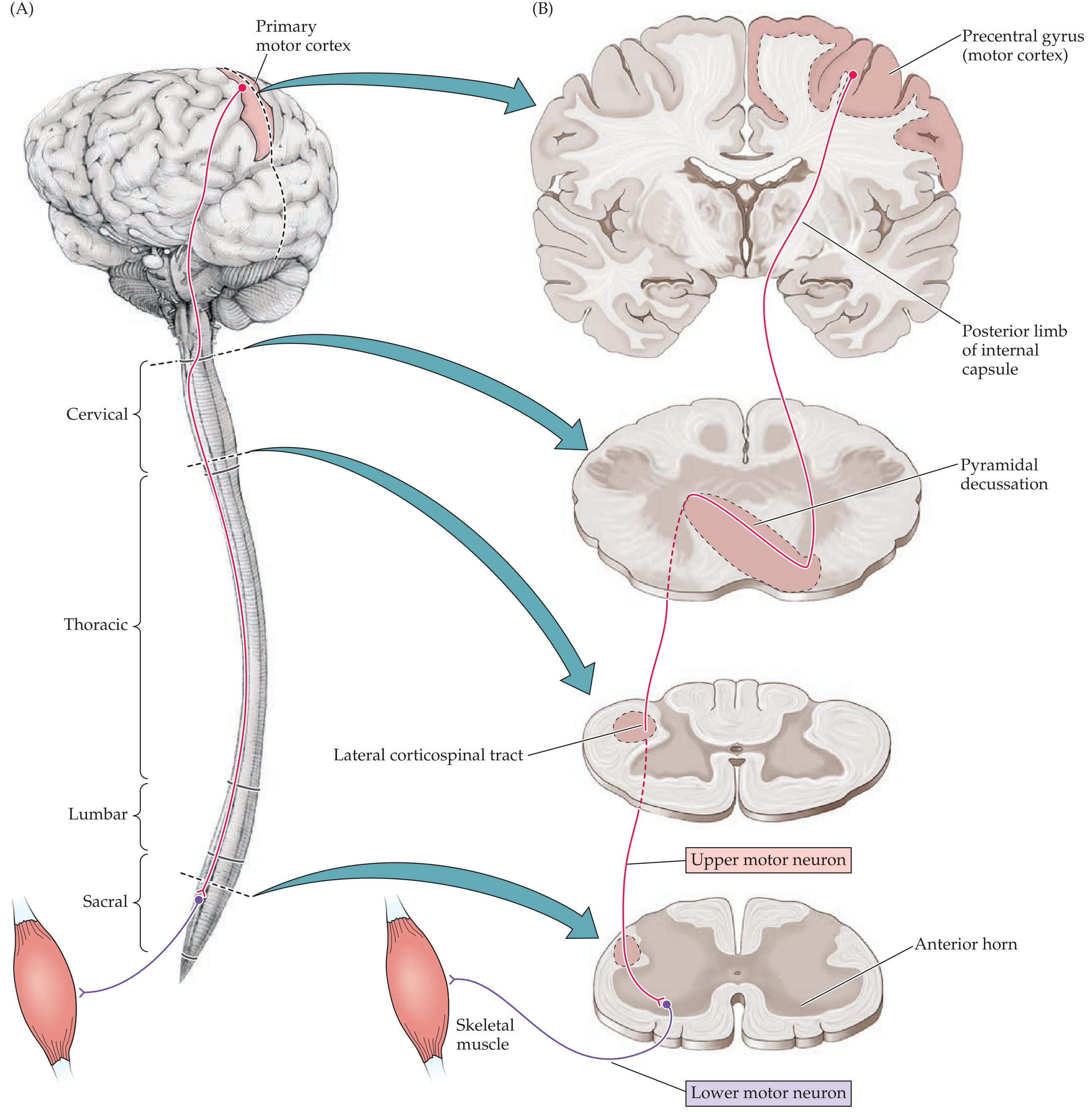
The corticospinal tract is the most important voluntary motor pathway in humans. Its course:
-
Origin: Primary motor cortex (precentral gyrus, Brodmann area 4) - mainly Betz cells (large pyramidal neurons). Also contributions from premotor cortex (area 6) and supplementary motor cortex. The motor homunculus is somatotopically arranged: face most inferior on lateral surface; leg/foot in paracentral lobule on medial surface.
-
Corona radiata: Fibres converge through cerebral white matter
-
Internal capsule (posterior limb): Corticospinal fibres travel in the posterior limb. Here they are intermingled with corticostriate, corticothalamic, corticopontine, and thalamocortical fibres. This is why an internal capsule lesion (e.g. capsular infarction) causes a dense hemiplegia affecting face + arm + leg, and the weakness is technically "UMN" (multiple descending systems involved, not purely pyramidal).
-
Cerebral peduncle (midbrain): Fibres occupy the middle three-fifths
-
Pons: Fibres broken up by pontine nuclei and transverse pontocerebellar fibres
-
Medullary pyramid: The ONLY place where corticospinal fibres are isolated from other systems. Lesion here = flaccid hemiplegia (no spasticity, because corticoreticulospinal fibres responsible for spasticity travel separately).
-
Pyramidal decussation (lower medulla): ~85-90% of fibres cross contralaterally and descend as the lateral corticospinal tract in the posterolateral white matter of the spinal cord. ~10-15% remain ipsilateral as the anterior corticospinal tract (cross at segmental level).
-
Spinal cord: Lateral corticospinal tract runs in the dorsolateral funiculus. Terminates mainly on interneurons in the intermediate zone of spinal grey matter (NOT directly on anterior horn cells in most cases). Only 10-20% of the fast-conducting Betz cell axons synapse directly on anterior horn cells.
-
Lower motor neuron (LMN): Anterior horn cell → anterior root → peripheral nerve → neuromuscular junction → skeletal muscle.
Lesions of the Corticospinal Tract
| Level of Lesion | Deficit |
|---|---|
| Motor cortex (area 4 alone) | Hypotonia + weakness of distal limb muscles. If areas 4+6 affected: weakness + spasticity |
| Subcortical white matter / corona radiata | Contralateral hemiplegia (face, arm, leg - arm often more affected) |
| Internal capsule | Dense contralateral hemiplegia (face + arm + leg equally affected) - all UMN signs |
| Midbrain (cerebral peduncle) | Weber's syndrome: contralateral hemiplegia + ipsilateral CN III palsy (ptosis, mydriasis, "down and out") |
| Pons | Millard-Gubler: contralateral hemiplegia + ipsilateral CN VI (lateral rectus palsy) + ipsilateral CN VII (LMN facial palsy) |
| Medullary pyramid | Contralateral flaccid hemiplegia (sparing face), with good recovery - NO spasticity initially |
| Spinal cord above C5 | Ipsilateral UMN signs below lesion, ipsilateral LMN signs at the level (anterior horn) |
| Cervical cord (C1-C4) | Quadriplegia (UMN) |
| Thoracic cord | Ipsilateral paraplegia (UMN below), with possible LMN signs at level |
Key feature of brainstem lesions (crossed/alternating syndromes): Ipsilateral cranial nerve palsy (LMN) + contralateral hemiplegia (UMN). This is because the cranial nerve nucleus/fascicles are at the level of lesion (below decussation = LMN ipsilateral), while corticospinal tract at that level has not yet decussated (or has just decussated = UMN contralateral).
Sources: Neuroanatomy through Clinical Cases 3E; Adams and Victor's Principles of Neurology 12E; Localization in Clinical Neurology 8E
4. Facial Nerve Pathway and UMN vs LMN Findings
Facial Nerve (CN VII) - Complete Pathway
CN VII has 5 functional components:
-
SVE (Special Visceral Efferent) - Branchial motor: Supplies muscles of facial expression, orbicularis oculi, orbicularis oris, buccinator, platysma, stapedius, posterior belly of digastric, stylohyoid
-
GVE (General Visceral Efferent) - Parasympathetic:
- Submandibular/sublingual glands via chorda tympani → lingual nerve
- Lacrimal gland + nasal/palatine glands via greater petrosal nerve → pterygopalatine ganglion
-
SVA (Special Visceral Afferent) - Taste: Anterior 2/3 of tongue via chorda tympani → geniculate ganglion → nucleus tractus solitarius
-
GVA (General Visceral Afferent) - minor sensory from middle ear
-
GSA (General Somatic Afferent) - Somatic sensation: Small area behind ear / external auditory meatus (Ramsay Hunt zone)
Motor Pathway (SVE):
Motor cortex (UMN)
↓ corticobulbar fibres
↓ bilateral to upper facial nucleus (forehead/orbicularis oculi)
↓ only contralateral to lower facial nucleus
↓
Facial nucleus (PONS - LMN cell bodies)
↓ nerve fibres loop around CN VI nucleus
(forming the facial colliculus = surface landmark of floor of 4th ventricle)
↓
Exits pons at cerebellopontine angle (CPA)
↓
Internal auditory meatus → Facial canal (petrous temporal bone)
↓
Geniculate ganglion (first genu)
↙ Greater petrosal nerve (parasympathetic to lacrimal gland)
↓
Second genu → Nerve to stapedius → Chorda tympani
↓
Stylomastoid foramen (exits skull)
↓
Parotid gland (divides into 5 branches):
Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical
CN VII: UMN vs LMN Lesion Findings
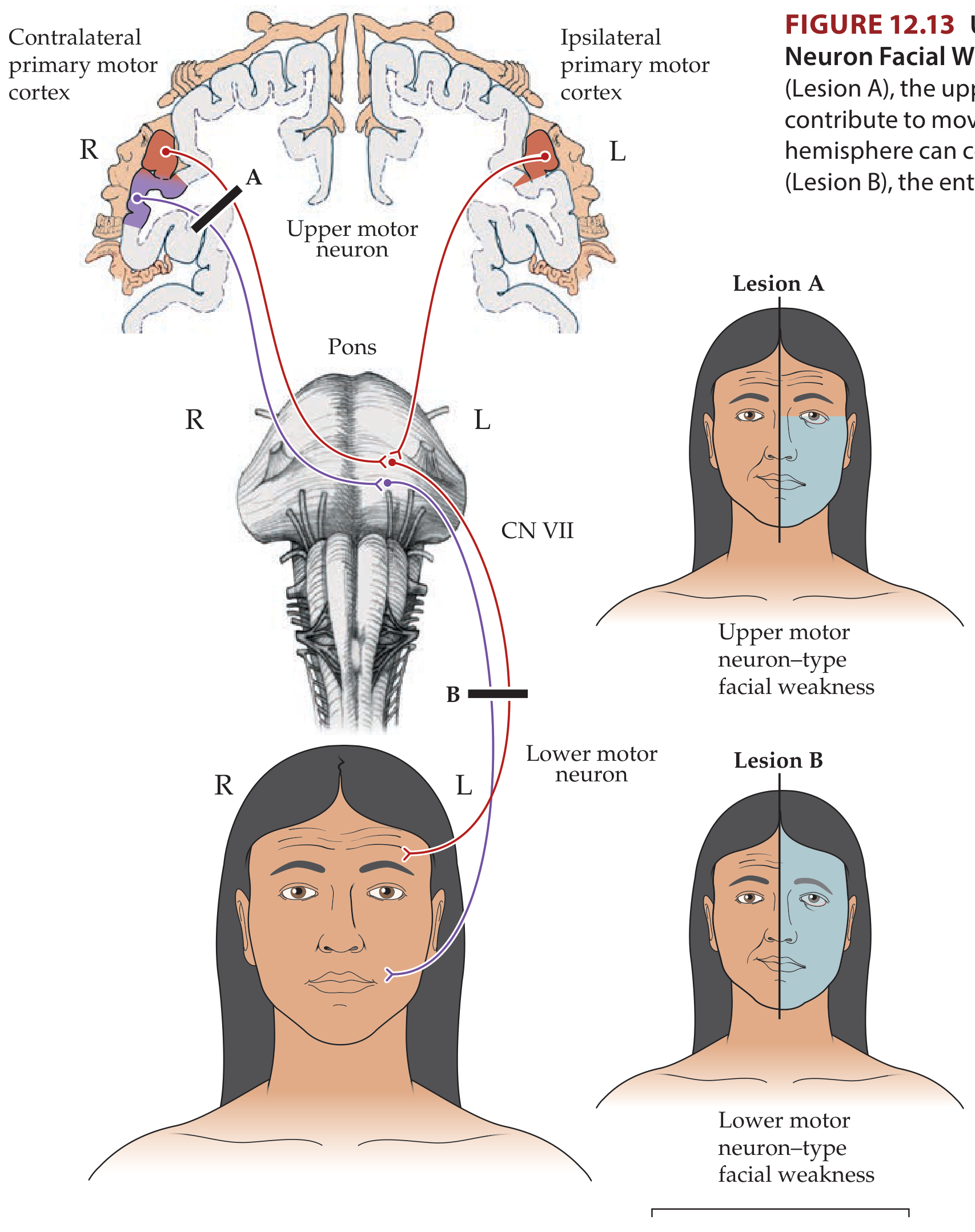
Why is the forehead spared in UMN lesions?
The upper motor neurons from both hemispheres innervate the upper facial nucleus (controlling forehead, orbicularis oculi). So if one hemisphere is damaged by a UMN lesion (e.g. stroke), the unaffected hemisphere still drives the upper face bilaterally. However, the lower facial nucleus only receives contralateral UMN input - so a UMN lesion on one side causes weakness of the contralateral lower face only.
| Feature | UMN Facial Palsy (Central) | LMN Facial Palsy (Peripheral) |
|---|---|---|
| Forehead | Spared (bilateral cortical input) | Affected (entire face weak) |
| Orbicularis oculi | Mildly affected (slight widening of palpebral fissure) | Severely affected - inability to close eye (lagophthalmos), Bell's phenomenon |
| Lower face | Weak contralateral (nasolabial fold flattening, drooping mouth) | Weak ipsilateral (entire half of face) |
| Side of weakness | Contralateral to lesion | Ipsilateral to lesion |
| Lacrimation | Normal | May be reduced (if geniculate involvement - greater petrosal nerve) |
| Hyperacusis | Absent | Present (if stapedius branch affected - intratemporal lesion) |
| Taste (ant. 2/3 tongue) | Normal | Impaired (if chorda tympani affected - before stylomastoid foramen) |
| Salivation | Normal | Reduced (chorda tympani) |
| Emotional/volitional dissociation | May be present (UMN lesion can selectively affect volitional OR emotional movements) | Both affected equally |
| Associated findings | Hemiplegia, aphasia, sensory loss, dysarthria | Retroauricular pain (Bell's palsy), Ramsay Hunt rash (zoster), parotid mass |
| Bell's phenomenon | Absent (eye closure preserved) | Present (eyeball rolls upward on attempted eye closure) |
| Corneal reflex | Afferent intact; efferent (eye closure) may be mildly diminished contralaterally | Reduced/absent ipsilaterally (efferent limb damaged) |
Common Causes
UMN facial palsy: Stroke (MCA territory), brain tumour, MS, head injury
LMN facial palsy:
- Bell's palsy (most common - idiopathic, viral/inflammatory, entire CN VII)
- Ramsay Hunt syndrome (herpes zoster of geniculate ganglion)
- Parotid tumour / surgery
- Petrous temporal bone fracture
- Acoustic neuroma (CPA) - compresses CN VII before it enters facial canal
- Pontine lesions (Millard-Gubler syndrome, MS)
- Lyme disease (bilateral LMN facial palsy is classic)
- Sarcoidosis, GBS
Localizing LMN Lesions by Clinical Features:
| Location | Features |
|---|---|
| Pontine nucleus/fascicle | LMN facial palsy + ipsilateral CN VI palsy (+ contralateral hemiplegia = Millard-Gubler) |
| CPA (internal auditory meatus) | LMN palsy + sensorineural deafness + tinnitus (CN VIII affected) |
| Geniculate ganglion | Facial palsy + hyperacusis + loss of taste + reduced lacrimation + ear pain/vesicles (Ramsay Hunt) |
| Above chorda tympani, below stapedius | Facial palsy + loss of taste + reduced lacrimation, NO hyperacusis |
| Below chorda tympani (near stylomastoid foramen) | Facial palsy alone (no taste, lacrimation, or hyperacusis lost) |
| After parotid | Partial palsy (individual branch distribution) |
Sources: Neuroanatomy through Clinical Cases 3E; Goldman-Cecil Medicine; Rosen's Emergency Medicine; Adams and Victor's Principles of Neurology 12E; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.