Give case presentation on tonsillitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
tonsillitis management
Reading File
Reading File
Reading File
Searching Images
tonsillitis inflamed tonsils throat
Reading File
Reading File
I have comprehensive data. Let me now compile the full case presentation.
Case Presentation: Tonsillitis
🏥 Case Vignette
Patient: Ethan M., 7-year-old male
Presenting Complaint: Sore throat, fever, and difficulty swallowing for 3 days
Referred by: Mother, who noted he has barely eaten or drunk fluids in 2 days
History of Presenting Illness
Ethan presents with a 3-day history of sudden-onset severe sore throat, associated with high-grade fever (measured at 39.2°C at home), odynophagia, and mild dysphagia. His mother reports he complained of ear pain (otalgia) and headache on day 2. There is no rhinorrhea, cough, hoarseness, or oral ulcers. He has no history of recent travel or sick contacts. He has had two prior similar episodes in the past 12 months, both treated with antibiotics.
Past Medical History
- Two prior episodes of pharyngotonsillitis in the past year
- Fully vaccinated, including diphtheria toxoid
- No known drug allergies
- No prior hospitalizations or surgeries
Review of Systems
| System | Findings |
|---|---|
| ENT | Severe sore throat, odynophagia, otalgia |
| Systemic | High fever, malaise, anorexia |
| GI | Reduced oral intake, nausea |
| Respiratory | No cough, no stridor |
| Neurological | Headache, no neck stiffness |
Physical Examination
Vitals:
- Temperature: 39.4°C (102.9°F)
- HR: 112 bpm, RR: 20/min, SpO₂: 98% on room air
General: Ill-appearing child, reluctant to swallow, no drooling
Oropharynx:
- Bilateral tonsillar enlargement (grade III — nearly touching midline)
- Bilateral tonsillar erythema with purulent white/yellow exudates
- Palatal petechiae at the hard-soft palate junction
- Uvula midline, no deviation
Neck: Bilateral tender anterior cervical lymphadenopathy, largest node ~1.5 cm on the right
Skin: No rash (no scarlatiniform rash)
Abdomen: No hepatosplenomegaly
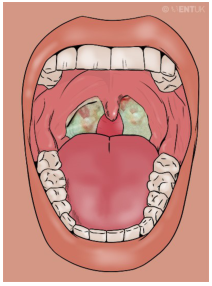
Bilateral tonsillar inflammation with white-greenish exudate, characteristic of acute exudative tonsillitis
Centor/McIsaac Score (GABHS Risk Stratification)
| Criterion | Present? | Points |
|---|---|---|
| Tonsillar exudate | ✅ Yes | +1 |
| Tender anterior cervical adenopathy | ✅ Yes | +1 |
| Fever > 38°C | ✅ Yes | +1 |
| Absence of cough | ✅ Yes | +1 |
| Age 3–14 years | ✅ Yes | +1 |
| Total Score | 5 |
Score ≥ 4 → High probability of GABHS; antibiotic treatment recommended.
Differential Diagnosis
| Condition | Supporting Features | Against |
|---|---|---|
| Acute bacterial tonsillitis (GABHS) ✅ | Exudate, fever, adenopathy, no cough, age 5–6 peak | — |
| Infectious mononucleosis (EBV) | High fever, exudate, adenopathy | No hepatosplenomegaly, no malaise, monospot not yet done |
| Viral pharyngitis | Common in children | Exudate and high fever are atypical; cough absent |
| Peritonsillar abscess | Prior tonsillitis | No trismus, uvula midline, no unilateral bulge |
| Diphtheria | Sore throat, high fever | Fully immunized; no grayish pseudomembrane |
| Herpangina (Coxsackie A) | Oropharyngeal infection | Herpangina causes vesicular ulcers, not exudative tonsillitis |
Investigations
Immediate
| Test | Expected Finding |
|---|---|
| Rapid Antigen Detection Test (RADT) — Rapid Strep Test | Positive for Group A Streptococcus |
| Throat swab culture | GABHS if RADT negative |
| CBC | Leukocytosis with neutrophilia (GABHS); lymphocytosis with atypical lymphocytes (EBV) |
| ESR/CRP | Elevated |
Additional (if EBV suspected)
| Test | Significance |
|---|---|
| Monospot (heterophile antibody test) | 85% sensitivity (less reliable in first 2 weeks) |
| EBV serology (VCA-IgM) | If monospot negative after 6 weeks |
| LFTs | If hepatosplenomegaly develops |
ASO titres are not recommended for acute diagnosis — they indicate prior infection only. — K.J. Lee's Essential Otolaryngology
Diagnosis
Acute Exudative Bacterial Tonsillitis — Group A Beta-Hemolytic Streptococcus (GABHS)
Pathophysiology
The palatine tonsils are lymphoid aggregates in the lateral oropharynx that serve as immunologic sentinels. GABHS (Streptococcus pyogenes) causes direct mucosal invasion, triggering an acute inflammatory response with:
- Tonsillar hyperemia, edema, and cryptal exudate formation
- Lymphadenopathy from reactive lymph node enlargement
- Systemic features (fever, malaise) from cytokine release and streptococcal toxins
Untreated GABHS can trigger non-suppurative sequelae (rheumatic fever, post-streptococcal glomerulonephritis) via molecular mimicry and immune complex deposition. — Cummings Otolaryngology
Management
1. Antibiotic Therapy (First-line)
| Drug | Dose | Duration |
|---|---|---|
| Amoxicillin (preferred in children) | 50 mg/kg/day divided Q12h (max 500 mg/dose) | 10 days |
| Penicillin V | 250–500 mg Q8–12h PO | 10 days |
| Azithromycin (if penicillin allergic) | 12 mg/kg/day once daily | 5 days |
| Cephalexin (if penicillin allergic, non-anaphylactic) | 25–50 mg/kg/day ÷ Q12h | 10 days |
2. Symptomatic Relief
- Analgesics/Antipyretics: Paracetamol (acetaminophen) or ibuprofen
- Adequate hydration: Encourage cold fluids, ice chips, popsicles
- Salt water gargles (older children/adults)
- Avoid aspirin in children (Reye's syndrome risk)
3. Indications for Hospital Admission
- Airway compromise
- Severe dehydration
- Inability to swallow oral antibiotics
- Suspected peritonsillar abscess
Complications
Suppurative
| Complication | Key Features |
|---|---|
| Peritonsillar abscess | Trismus (best indicator), unilateral palatal bulge, uvula deviation to contralateral side, "hot potato" voice |
| Parapharyngeal abscess | Rupture of peritonsillar abscess through superior constrictor |
| Retropharyngeal abscess | Especially in children < 5 years |
| Lemierre's syndrome | Fusobacterium necrophorum, septic thrombophlebitis of internal jugular vein |
| Otitis media | Via Eustachian tube |
| Sinusitis | Local spread |
| Mediastinitis | Rare, descending necrotizing infection |
Non-suppurative (Post-Streptococcal)
| Complication | Mechanism |
|---|---|
| Acute Rheumatic Fever | Molecular mimicry → cardiac valve damage |
| Post-streptococcal glomerulonephritis | Immune complex deposition in glomeruli |
| PANDAS | Pediatric autoimmune neuropsychiatric disorder associated with streptococcal infection |
| PFAPA syndrome | Periodic Fever, Aphthous stomatitis, Pharyngitis, Cervical Adenitis (recurs every ~3 weeks, each episode ~3 days) |
Tonsillectomy Indications (Paradise Criteria)
Surgical referral is indicated when recurrences meet these thresholds:
| Threshold | Criteria |
|---|---|
| 7 or more episodes of tonsillitis in 1 year | OR |
| 5 or more episodes per year for 2 consecutive years | OR |
| 3 or more episodes per year for 3 consecutive years |
Additional indications:
- Peritonsillar abscess
- Obstructive sleep apnea from tonsillar hypertrophy ("kissing tonsils")
- Suspected malignancy (asymmetric enlargement)
— K.J. Lee's Essential Otolaryngology; KJ Lee's block 5, line 7692–7750; Cummings Otolaryngology
Outcome of This Case
Ethan was started on amoxicillin 500 mg Q12h for 10 days, ibuprofen for fever and pain, and instructed to maintain oral hydration. RADT returned positive. He defervesced within 48 hours and resumed normal oral intake. He is scheduled for follow-up in 2 weeks. Given this is his 3rd episode in 2 years, he will be monitored for the Paradise criteria threshold for tonsillectomy.
Key Teaching Points
- Viruses cause the majority of tonsillitis — rhinovirus is most common overall; GABHS is the most important bacterial cause (10–23% of cases).
- The Centor/McIsaac score guides empiric antibiotic use: score ≥ 4 warrants treatment without waiting for culture.
- RADT is first-line for bacterial confirmation; if negative, send a throat culture.
- Amoxicillin/Penicillin for 10 days remains the gold standard — shorter courses have higher relapse rates.
- The most feared complication is peritonsillar abscess — trismus is the best clinical indicator.
- Always consider infectious mononucleosis in adolescents with exudative tonsillitis before prescribing amoxicillin (causes a florid maculopapular rash with amoxicillin in EBV).
- Non-suppurative complications (rheumatic fever, GN) are the primary reason to treat GABHS promptly with antibiotics.
Sources: K.J. Lee's Essential Otolaryngology (9th ed.), Cummings Otolaryngology Head and Neck Surgery, Tintinalli's Emergency Medicine, Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.