bradycardia algorithm according to ACLS
Reading File
Finding Sources
Searching the Web
ACLS bradycardia algorithm 2024 AHA steps atropine pacing
Loading Image
Finding Sources
Reading File
Here is the complete ACLS Adult Bradycardia Algorithm (2025/2026 AHA Guidelines):
AHA ACLS Adult Bradycardia Algorithm
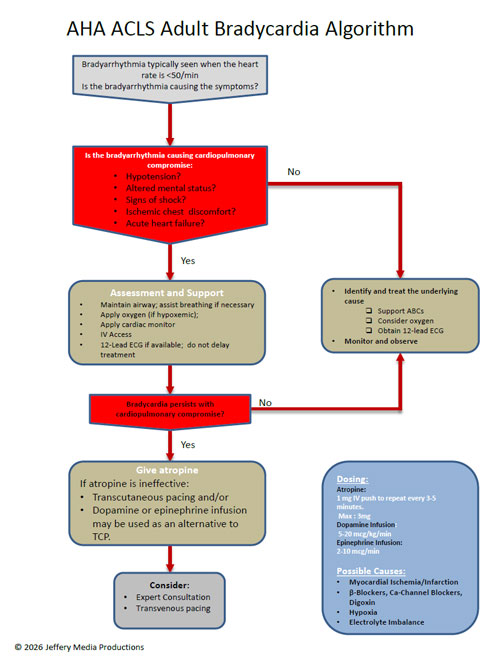
Definition and Trigger
Bradycardia = HR < 60 bpm. The algorithm activates when the rate is typically < 50 bpm AND symptoms are present. The key question is: "Is the bradyarrhythmia causing the symptoms?"
Step 1 - Initial Assessment
Regardless of stability, all patients get:
- Maintain patent airway; assist breathing if needed
- Supplemental oxygen (if hypoxic - SpO2 < 94%)
- Continuous cardiac monitoring (identify rhythm)
- IV/IO access
- 12-lead ECG (do not delay treatment to obtain it)
- Frequent blood pressure and SpO2 monitoring
Step 2 - Is the Patient Stable or Unstable?
Signs of cardiopulmonary compromise (unstable):
| Sign | Detail |
|---|---|
| Hypotension | SBP < 90 mmHg or symptomatic |
| Acute altered mental status | Confusion, agitation, reduced consciousness |
| Signs of shock | Cool/clammy skin, diaphoresis, poor perfusion |
| Ischemic chest discomfort | New chest pain or pressure |
| Acute heart failure | Pulmonary edema, dyspnea, elevated JVP |
If NO symptoms/stable → Identify and treat the underlying cause, support ABCs, obtain 12-lead ECG, monitor and observe.
Step 3 - Unstable Patient: Pharmacologic and Electrical Treatment
First-Line: Atropine
| Detail | Value |
|---|---|
| Dose | 1 mg IV push |
| Repeat | Every 3-5 minutes |
| Maximum total dose | 3 mg |
| Caution | Ineffective in heart transplant patients (no vagal innervation) |
| Caution | Use with care in AMI (increased HR raises O2 demand) |
| Caution | Avoid doses < 0.5 mg (paradoxical bradycardia) |
Second-Line (if atropine ineffective): Choose one or combine
| Intervention | Dose | Notes |
|---|---|---|
| Transcutaneous Pacing (TCP) | Set rate ~60-80 bpm; titrate energy to capture | Immediate bridge; confirm electrical AND mechanical capture; use femoral pulse (not carotid) to check circulation |
| Dopamine infusion | 5-20 mcg/kg/min IV | Chronotropic and vasopressor effect |
| Epinephrine infusion | 2-10 mcg/min IV | Equal alternative to dopamine |
Per the 2015 AHA update, dopamine/epinephrine infusions are equally effective alternatives to TCP when atropine fails.
Step 4 - Expert Consultation and Transvenous Pacing
Consider when:
- Initial treatments are ineffective
- High-degree AV block (Mobitz II / complete heart block)
- Persistent symptoms despite drug therapy
- Long-term pacemaker evaluation may be needed
TCP is a bridge to transvenous pacing - it is not a definitive treatment.
Possible Reversible Causes (H's and T's relevant to bradycardia)
| Cause | Example |
|---|---|
| Myocardial ischemia/infarction | Inferior MI - RCA involvement - SA/AV node ischemia |
| Beta-blockers / Ca-channel blockers | Drug overdose or excess |
| Digoxin toxicity | Especially with hypokalemia |
| Hypoxia | Correct first - may resolve bradycardia |
| Electrolyte imbalance | Hyperkalemia |
| Hypothermia | Osborne J-waves on ECG |
| Increased vagal tone | Vasovagal, bowel distention, ocular/ICP pressure |
Key Clinical Pearls
- Atropine is vagolytic - it works on the SA node and AV node via muscarinic blockade. It will NOT work in infranodal (His-Purkinje) blocks such as Mobitz Type II or complete heart block - go straight to pacing in these cases.
- Mobitz II and 3rd degree AV block are high-risk rhythms. Do not rely on atropine alone; prepare for TCP immediately.
- TCP confirmation: always confirm mechanical capture using femoral pulse palpation (TCP muscle twitching can mimic a carotid pulse).
- Heart transplant patients: atropine is ineffective - use dopamine, epinephrine, or TCP.
- Hypothermia: TCP is contraindicated.
Sources: AHA 2025 Guidelines for CPR and ECC; Miller's Anesthesia 10e, p. 11608-11609; ACLS.net Bradycardia Algorithm; ACLS-Algorithms.com 2026
metabolism of vecuronium
Finding Sources
Searching the Web
vecuronium metabolism pharmacokinetics 3-desacetyl metabolite
Reading File
Reading File
Reading File
Reading File
Here is a detailed account of the metabolism of vecuronium:
Vecuronium - Metabolism and Pharmacokinetics
Structure
Vecuronium is a monoquaternary aminosteroid (pancuronium minus one quaternary methyl group). It is a non-depolarizing neuromuscular blocking agent (NMBA). The monoquaternary structure - compared to pancuronium's bisquaternary structure - makes it more lipid-soluble and is the basis for its predominantly hepatic (rather than renal) elimination.
Metabolic Pathway
Vecuronium undergoes partial hepatic deacetylation at three positions on the steroidal ring, producing three metabolites:
| Metabolite | Potency vs. Vecuronium | Clinical Significance |
|---|---|---|
| 3-desacetyl-vecuronium (ORG 7268) | ~80% of parent | Most potent; accumulates with long-term infusion; main cause of prolonged ICU paralysis |
| 17-desacetyl-vecuronium | ~50% of parent | Moderate activity |
| 3,17-desacetyl-vecuronium | Weak | Minimal clinical significance |
The 3-desacetyl metabolite is the most clinically important. It has been shown to be a potent neuromuscular blocker in its own right and is responsible for episodes of prolonged paralysis seen after long-term vecuronium infusions in ICU patients.
Routes of Elimination
| Route | Proportion | Notes |
|---|---|---|
| Biliary (fecal) | ~40-50% | Primary route; parent drug excreted unchanged |
| Renal (urine) | ~20-25% | Secondary route |
| Hepatic metabolism | Small fraction | Deacetylation to active metabolites |
Key points from the textbooks:
- "Vecuronium is metabolized to a small extent by the liver. It depends primarily on biliary excretion and secondarily (25%) on renal excretion." - Morgan & Mikhail's Clinical Anesthesiology, 7e
- "The elimination of vecuronium is primarily hepatic, but up to 20% of the drug is eliminated in urine." - Morgan & Mikhail's Clinical Anesthesiology, 7e (kidney disease chapter)
Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Elimination half-life | ~60-80 minutes (shorter than pancuronium) |
| Duration of action | Intermediate (~25-40 min at intubating doses) |
| Volume of distribution | ~0.27 L/kg |
| Clearance | ~3-5 mL/kg/min (higher than pancuronium - explains shorter duration) |
Vecuronium's shorter duration vs. pancuronium is explained by its shorter elimination half-life and greater clearance, not by a fundamentally different metabolic route.
Clinical Implications of Metabolism
1. Liver Disease
- Duration is usually not significantly prolonged in cirrhosis at standard doses
- At doses > 0.15 mg/kg, prolongation may occur
- Requirements are reduced during the anhepatic phase of liver transplantation (no biliary excretion)
2. Kidney Failure
- Satisfactory to use, but duration is moderately prolonged (active metabolites are renally excreted)
- Effects of large doses (>0.1 mg/kg) are only modestly prolonged
3. Prolonged ICU Infusion - Critical Warning
After long-term vecuronium infusions in ICU patients, prolonged neuromuscular blockade lasting days may occur after discontinuation. Mechanism:
- Accumulation of the active 3-desacetyl-vecuronium metabolite
- Changing drug clearance over time
- Can progress to critical illness polyneuropathy/myopathy
Risk factors for prolonged blockade:
- Female gender
- Kidney failure
- Long-term or high-dose corticosteroid therapy
- Sepsis
4. Infants < 1 year
- Vecuronium behaves as a long-acting agent (unlike intermediate in adults) due to hepatic immaturity and longer half-life
- Active metabolites depend on renal excretion, which is also immature
5. Pregnancy/Postpartum
- Duration may be further prolonged due to alterations in hepatic blood flow and liver uptake
6. Comparison with Rocuronium
- Rocuronium (a structural analogue) undergoes no hepatic metabolism and has no active metabolites - making it preferable over vecuronium for prolonged ICU infusions
Reversal
- Neostigmine/glycopyrrolate (anticholinesterase route)
- Sugammadex - encapsulates vecuronium (and rocuronium) and eliminates the complex renally; rapid and complete reversal even of dense block. Note: not recommended when creatinine clearance < 30 mL/min or in patients on renal replacement therapy.
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e, p. 401-402; Barash Clinical Anesthesia 9e, p. 3467; Caldwell et al., 1994 - 3-desacetylvecuronium pharmacodynamics
This is a shared conversation. Sign in to Orris to start your own chat.