I need everything about AKI and CkD and dialysis
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"acute kidney injury"[MeSH Terms] AND "chronic kidney disease"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"acute kidney injury"[MeSH Terms] AND management
Searching PubMed
"chronic kidney disease"[MeSH Terms] AND progression
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Here is a comprehensive, textbook-sourced guide to AKI, CKD, and Dialysis.
Acute Kidney Injury (AKI), Chronic Kidney Disease (CKD), and Dialysis
Sources: Harrison's Principles of Internal Medicine 22E, Brenner and Rector's The Kidney, Comprehensive Clinical Nephrology 7th Edition, Fischer's Mastery of Surgery 8th Edition, Textbook of Family Medicine 9e
Part 1: Acute Kidney Injury (AKI)
Definition
AKI is defined (KDIGO criteria) as any of the following:
- A rise in serum creatinine (SCr) ≥0.3 mg/dL within 48 hours, OR
- A rise in SCr to ≥1.5× baseline within 7 days, OR
- Urine output <0.5 mL/kg/h for ≥6 hours
AKI is distinguished from CKD by duration: CKD requires impaired function or structural damage for >3 months. An intermediate entity - Acute Kidney Disease (AKD) - applies when kidney dysfunction is present for <3 months but does not meet classic AKI criteria.
Staging (KDIGO / AKIN / RIFLE)
| System | Stage | SCr Criteria | Urine Output |
|---|---|---|---|
| KDIGO/AKIN | Stage 1 | ≥0.3 mg/dL or ≥50% rise | <0.5 mL/kg/h for >6 h |
| KDIGO/AKIN | Stage 2 | ≥100% rise (2× baseline) | <0.5 mL/kg/h for >12 h |
| KDIGO/AKIN | Stage 3 | ≥200% rise or need for RRT | <0.3 mL/kg/h for >24 h or anuria >12 h |
| RIFLE | Loss | Need for RRT >4 weeks | - |
| RIFLE | End-stage | Need for RRT >3 months | - |
- Brenner and Rector's The Kidney, Table 29.2
Etiology and Classification
AKI is divided into three broad categories:
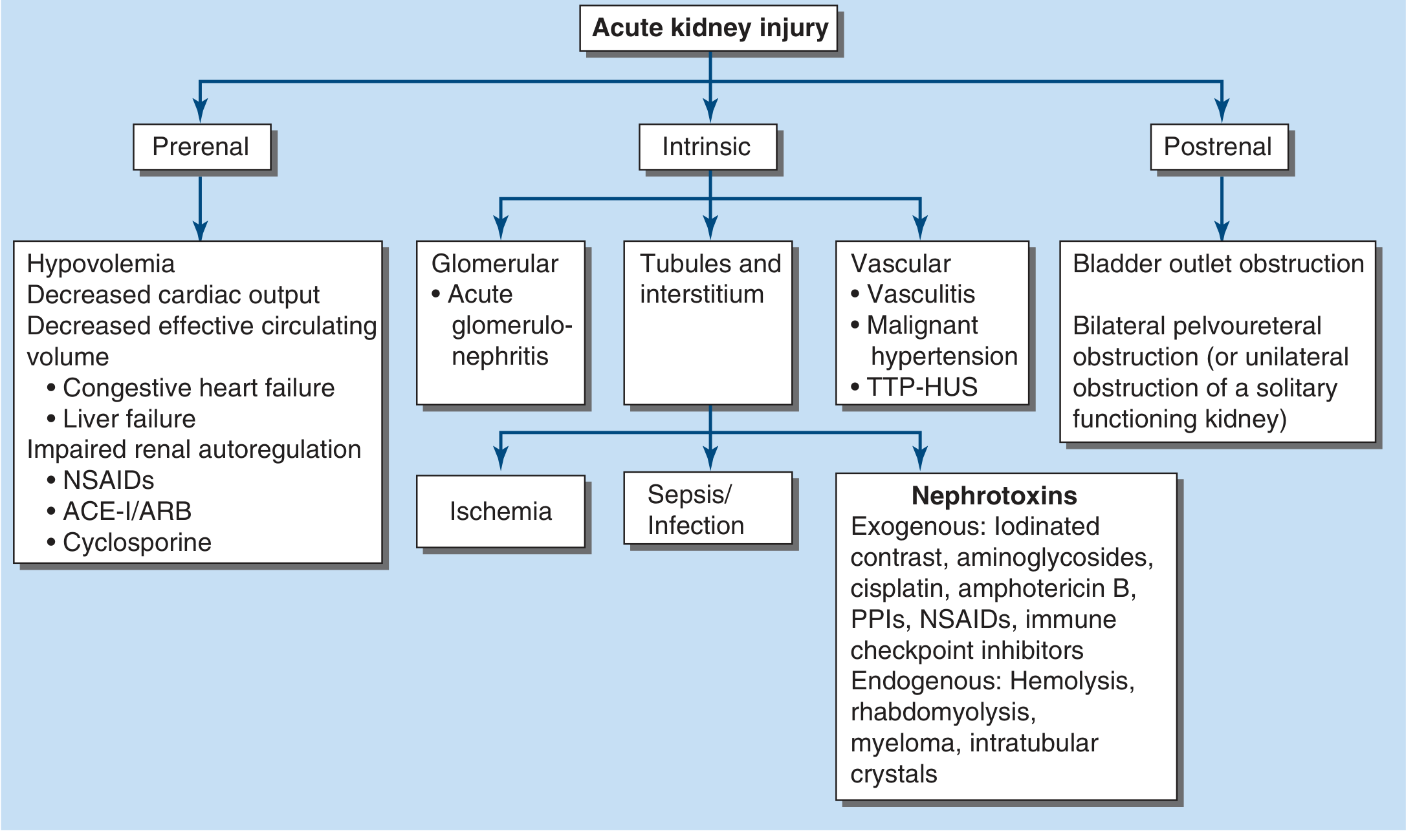
1. Prerenal Azotemia (most common)
- Results from inadequate renal plasma flow and reduced intraglomerular hydrostatic pressure
- Common causes: hypovolemia, decreased cardiac output (CHF, liver failure), medications impairing renal autoregulation (NSAIDs, ACE inhibitors, ARBs, cyclosporine)
- No parenchymal damage - rapidly reversible when perfusion restored
- Prolonged prerenal state -> ischemic tubular injury -> ATN
- Autoregulatory mediators involved: angiotensin II, norepinephrine, vasopressin, prostaglandins (prostacyclin, PGE2), nitric oxide
- Note: SGLT-2 inhibitors do not appear to increase AKI risk and may have a protective effect
- Harrison's Principles of Internal Medicine 22E, Ch. 321
2. Intrinsic Renal AKI
- Tubular (ATN): ischemia or nephrotoxins (aminoglycosides, cisplatin, contrast, amphotericin B, PPIs, NSAIDs, immune checkpoint inhibitors)
- Exogenous: iodinated contrast, cisplatin, aminoglycosides, amphotericin B
- Endogenous: hemolysis, rhabdomyolysis, myeloma, intratubular crystals
- SCr rise with aminoglycosides/cisplatin is characteristically delayed 3-5 days to 2 weeks
- Glomerular: acute glomerulonephritis
- Vascular: vasculitis, malignant hypertension, TTP-HUS
- Interstitial: acute interstitial nephritis (AIN) - drug-induced allergic reaction
3. Postrenal (Obstructive)
- Bladder outlet obstruction (benign prostatic hyperplasia most common in men)
- Bilateral pelvoureteral obstruction (or unilateral if solitary functioning kidney)
- Brenner and Rector's The Kidney, PATHOPHYSIOLOGY section
Evaluation
Clinical assessment:
- Volume status: orthostatic hypotension, JVP, mucous membrane dryness
- Drug history: NSAIDs, diuretics, ACE-I/ARBs, contrast agents
- Review of prior creatinine trends
Key urinalysis findings:
| AKI Cause | Urinary Findings | FENa | Other |
|---|---|---|---|
| Prerenal azotemia | Hyaline casts | <1% | UNa <10, SG >1.018 |
| ATN | Pigmented "muddy brown" granular casts, tubular epithelial cells | >2% | - |
| Glomerulonephritis | Dysmorphic RBCs, RBC casts | Variable | - |
| Interstitial nephritis | WBC casts | >1% | Eosinophiluria (limited specificity) |
| Rhabdomyolysis | Myoglobin, pigmented granular casts | - | Elevated CK |
- Brenner and Rector's The Kidney, Table 29.4
Blood tests: SCr, BUN, CBC (anemia, eosinophilia, thrombocytopenia), LDH, haptoglobin, ADAMTS13 (if TTP suspected), complement levels, ANCA, anti-GBM if glomerulonephritis suspected.
Imaging: Renal ultrasound - small echogenic kidneys suggest CKD; enlarged kidneys don't rule out CKD (diabetes, HIV, amyloidosis, polycystic disease).
Urinary cystatin C and α1-microglobulin are sensitive biomarkers of proximal tubule dysfunction. Urinary cystatin C and α1-microglobulin (AUC 0.86) are the strongest predictors of the need for RRT, while urinary α1-microglobulin in ER patients had AUC 0.88 with cutoff 35 mg/g (80% sensitivity, 81% specificity). - Brenner and Rector's The Kidney, block 15
Management
Prerenal AKI
- IV fluid resuscitation for hypovolemia (normal saline or balanced crystalloids)
- Discontinue NSAIDs, ACE-I, ARBs
- Optimize cardiac output in heart failure
- Hepatorenal syndrome: terlipressin (or norepinephrine) + midodrine + IV albumin (25-50 g, max 100 g/day)
Intrinsic AKI
- ATN: supportive care - no agent has proven efficacy (atrial natriuretic peptide, dopamine, erythropoietin, endothelin antagonists, growth factors all failed in trials)
- Glomerulonephritis/vasculitis: immunosuppressants, anti-complement therapy, plasmapheresis
- Allergic interstitial nephritis: stop offending drug; glucocorticoids used (not RCT-proven)
- Scleroderma renal crisis: ACE inhibitors
- TTP: plasma exchange (medical emergency); atypical HUS: complement blockade (eculizumab)
- Rhabdomyolysis: early aggressive volume repletion (up to 10 L/day); alkaline fluids (75 mmol/L NaHCO3 in 0.45% saline) to alkalinize urine and prevent cast formation
Postrenal AKI
- Bladder catheterization for urethral/bladder outlet obstruction
- Percutaneous nephrostomy or ureteric stent for ureteral obstruction
- Post-obstructive diuresis expected after relief; monitor and replace fluids/electrolytes
Supportive measures
- Volume management: restrict fluid/Na; loop diuretics (furosemide bolus 200 mg then IV drip 10-40 mg/h ± thiazide); no evidence that forced diuresis changes AKI natural history
- Hyperkalemia: calcium gluconate (cardiac protection), insulin/dextrose, sodium bicarbonate, kayexalate - then dialysis if refractory
- Nutrition: avoid protein restriction; standard enteral nutrition preferred
- Harrison's Principles of Internal Medicine 22E, Ch. 321
Part 2: Chronic Kidney Disease (CKD)
Definition
CKD is defined as kidney damage or decreased kidney function for ≥3 months, as defined by the NKF KDOQI guidelines. Markers include proteinuria, abnormal urine sediment, structural abnormalities on imaging, or reduced GFR.
- Textbook of Family Medicine 9e, Ch. 40
Staging (GFR-based)
| Stage | Description | GFR (mL/min/1.73 m²) |
|---|---|---|
| 1 | Kidney damage, normal GFR | ≥90 |
| 2 | Kidney damage, mildly decreased GFR | 60-89 |
| 3 | Moderately decreased GFR | 30-59 |
| 4 | Severely decreased GFR | 15-29 |
| 5 | Kidney failure (ESKD) | <15 (or dialysis) |
GFR estimation formulas:
- Cockcroft-Gault: CrCl = [(140 - age) × weight] / (72 × SCr), ×0.85 if female
- MDRD: GFR = 1.86 × (SCr)^-1.154 × (age)^-0.203 × 0.742 (female) × 1.210 (Black)
- Modern clinical practice uses CKD-EPI (not shown in older textbook editions)
Causes / Risk Factors
- Diabetic nephropathy (most common in developed world)
- Hypertension (hypertensive nephrosclerosis)
- Glomerulonephritis (IgA nephropathy, FSGS, membranous, lupus)
- Polycystic kidney disease (autosomal dominant)
- Obstructive uropathy
- Repeated episodes of AKI -> CKD progression
- HIV-associated nephropathy (associated with APOL1 variants)
Biomarker link: Elevated urinary α1-microglobulin in HIV-infected women associated with 2.1-fold increased risk of developing CKD and 2.7-fold risk of 10% eGFR decline. - Brenner and Rector's The Kidney, block 15
Complications by Stage
| Complication | When It Appears |
|---|---|
| Hypertension | Early (any stage) |
| Anemia (EPO deficiency) | Stage 3-4 |
| Metabolic acidosis | Stage 3-4 |
| Hyperphosphatemia, secondary hyperparathyroidism | Stage 3+ |
| Hyperkalemia | Stage 4-5 |
| Volume overload | Stage 4-5 |
| Uremic symptoms (nausea, pruritus, encephalopathy) | Stage 5 |
| Uremic pericarditis | Late Stage 5 |
Management
Slowing progression:
- BP control: target <130/80 mmHg; ACE inhibitors or ARBs first-line in proteinuric CKD (reduce intraglomerular pressure and proteinuria)
- Glycemic control in diabetics (HbA1c ~7%)
- SGLT-2 inhibitors (e.g., empagliflozin, dapagliflozin) - now a pillar of CKD management in diabetic and non-diabetic CKD; reduces progression and cardiovascular events
- Protein restriction: 0.6-0.8 g/kg/day in later stages
- Avoid nephrotoxins, NSAIDs, contrast without prehydration
- Smoking cessation
Managing complications:
- Anemia: erythropoiesis-stimulating agents (ESAs: epoetin alfa, darbepoetin); IV iron supplementation; target Hb 10-12 g/dL
- CKD-MBD (mineral-bone disease): phosphate binders (calcium carbonate, sevelamer, lanthanum), vitamin D analogs (calcitriol), calcimimetics (cinacalcet)
- Metabolic acidosis: sodium bicarbonate supplementation (target serum bicarb >22 mmol/L)
- Hyperkalemia: dietary K restriction, patiromer or sodium zirconium cyclosilicate (ZS-9)
- Hypertension/volume: loop diuretics, salt restriction
- Dyslipidemia: statins (though benefit in dialysis patients not clearly established)
Preparation for ESKD:
- Early referral to nephrology (GFR <30)
- AV fistula placement at least 6 months before anticipated dialysis start
- Peritoneal dialysis catheter placement 4-6 weeks before start
- Renal transplant evaluation (preferred modality if eligible)
Part 3: Dialysis
Indications for Renal Replacement Therapy (RRT)
Absolute Indications (initiate immediately):
- Volume overload unresponsive to diuretic therapy (most common indication in AKI)
- Persistent hyperkalemia despite medical therapy
- Severe metabolic acidosis
- Overt uremic symptoms: encephalopathy, pericarditis (late, urgent sign; can progress to tamponade), uremic bleeding diathesis
Relative Indications:
- Progressive azotemia without uremic manifestations
- Persistent oliguria
- BUN >60-100 mg/dL (no hard threshold; initiation before profound uremia is preferred)
"Uremic pericarditis can progress to tamponade if hemorrhage is seen. It is best to initiate RRT with elevated circulating nitrogen levels before clinical evidence of profound uremia." - Fischer's Mastery of Surgery 8e
Transplantation is a form of RRT for ESKD but plays no role in AKI management. - Brenner and Rector's The Kidney, block 16
Principles of Dialysis
Three physical mechanisms underlie all dialysis modalities:
-
Ultrafiltration: Water and solutes cross a semipermeable membrane via a transmembrane pressure gradient. Rate depends on membrane surface area, transmembrane pressure, and membrane permeability.
-
Diffusion: Solutes move from high to low concentration. Dialysate runs countercurrent to blood. The dialysate composition is adjusted to the patient's electrolytes (e.g., potassium in dialysate lower than plasma -> potassium moves out of blood).
-
Convection: Solutes are dragged through the membrane with water (solvent drag). Pore size of the membrane determines which solutes can pass (important for larger "middle molecules").
Modalities Comparison
| Feature | Intermittent HD (iHD) | CRRT | Peritoneal Dialysis (PD) |
|---|---|---|---|
| Session duration | 3-4 hours, 3×/week | Continuous (24h/day) | Continuous (4-6 exchanges/day) |
| Blood flow rate | High | Low | N/A |
| Solute removal | Rapid, by diffusion | Slow, steady | Slow, diffusion/convection |
| Volume removal | Rapid ultrafiltration | Gradual | Gradual |
| Best for | Stable patients, acute hyperkalemia, toxin removal | Hemodynamically unstable patients | Chronic ESKD, home setting |
| Anticoagulation need | Lower (high BFR) | Higher (lower BFR, filter clotting) | None |
| Risk | Hypotension, cerebral edema (disequilibrium) | Less BP perturbation | Peritonitis, technique failure |
| Use in AKI | Yes | Yes (preferred in ICU/shock) | Not used for AKI |
- Fischer's Mastery of Surgery 8e, p. 226-227; Comprehensive Clinical Nephrology 7e, Ch. 95
Hemodialysis (HD)
- Blood is pumped through an extracorporeal circuit at 300-500 mL/min, across a semipermeable dialyzer membrane
- Dialysate flows countercurrent at 500-800 mL/min
- Vascular access: AV fistula (preferred) > AV graft > central venous catheter (CVC; highest infection risk)
- AV fistula should be created ≥6 months before anticipated dialysis start
- Standard dose: Kt/V ≥1.2 per session (K = urea clearance, t = time, V = volume of distribution)
- Complications: hypotension (most common), muscle cramps, disequilibrium syndrome, infection (CVC-related bacteremia), cardiovascular events
Peritoneal Dialysis (PD)
- Uses the peritoneal membrane as the dialyzer
- Dialysate (glucose-based) is instilled into the peritoneal cavity and drained after a dwell time
- CAPD (continuous ambulatory PD): 4 manual exchanges/day
- APD (automated PD): overnight machine cycling
- Advantages: home-based, preserves residual renal function longer, no vascular access needed, better hemodynamic stability, superior health-related quality of life
- PD preferred as first choice in Hong Kong (75% of prevalent dialysis) unless absolute contraindications
- Technique failure causes: infection (peritonitis), mechanical problems, inadequate dialysis, social reasons
- Late technique failure primarily due to social factors; infection-related failure carries higher short-term mortality (mainly cardiac)
- Comprehensive Clinical Nephrology 7e, Ch. 95
PD vs HD survival: No consistent survival advantage for either modality in observational studies. Previous concern about PD inferiority in CHD/heart failure patients has not been confirmed in more recent evidence.
CRRT (Continuous Renal Replacement Therapy)
- Runs 24 hours/day at low blood flow rates (100-200 mL/min)
- Preferred in hemodynamically unstable ICU patients
- Subtypes:
- CVVH (continuous veno-venous hemofiltration) - convection only
- CVVHD (continuous veno-venous hemodialysis) - diffusion only
- CVVHDF (continuous veno-venous hemodiafiltration) - both
- Requires continuous anticoagulation (heparin or citrate)
- Less effective at rapid solute removal vs. iHD, but causes far less hemodynamic perturbation
- No evidence that CRRT is superior to iHD for survival in AKI
Timing of RRT in AKI: Early vs. Late
The IDEAL-ICU and STARRT-AKI trials showed no benefit to early initiation of RRT compared with a watchful waiting strategy. The STARRT-AKI trial found that accelerated (early) strategy was not superior and was associated with more adverse events. Similarly, the Cooper et al. IDEAL trial found no difference in mortality between early and late dialysis start in CKD patients (shown in the Kaplan-Meier curve in Comprehensive Clinical Nephrology 7e, Fig. 95.5).
Current guidance: Initiate RRT when absolute indications are present; avoid "prophylactic" initiation for azotemia alone without clinical signs.
Choice of Dialysis Modality for ESKD
Most patients are suitable for either HD or PD. The NECOSAD trial (Netherlands Cooperative Study on Adequacy of Dialysis) was stopped early due to low recruitment, underscoring the difficulty of RCTs in this field.
Factors favoring PD:
- Preference for home therapy
- Remote location / limited HD access
- Residual renal function to preserve
- Better QoL reported
- Vascular access difficulties
Factors favoring HD:
- Prior abdominal surgery / adhesions (relative contraindication to PD)
- Active IBD / abdominal hernias (relative contraindication to PD)
- Poor manual dexterity or social support (can't manage PD exchanges)
- Severe protein-energy malnutrition (PD causes protein loss)
Global access: PD is available in >90% of upper-middle and high-income countries but only 32% of low-income countries. - Comprehensive Clinical Nephrology 7e
AKI to CKD Progression
AKI is increasingly recognized as a major risk factor for CKD. The pathway involves:
- Incomplete tubular repair -> fibrosis and tubular atrophy
- ET-1/ET-A receptor upregulation after transient ischemia drives progressive injury
- ET-A receptor antagonism (but not ET-B) prevents progressive kidney injury in animal models - Brenner and Rector's The Kidney, block 6
Prevention of AKI-to-CKD transition involves:
- Aggressive early AKI management
- Avoiding nephrotoxin re-exposure after recovery
- Long-term nephrology follow-up after AKI episodes (SCr checks at 3 and 12 months)
Quick Reference Summary
| AKI | CKD | ESKD / Dialysis | |
|---|---|---|---|
| Duration | <3 months | ≥3 months | GFR <15 or on dialysis |
| Definition tool | KDIGO staging (SCr, UO) | GFR + albuminuria staging | Clinical |
| Reversible? | Yes (usually) | Partially (slow progression) | No (requires RRT or transplant) |
| Key biomarkers | SCr, BUN, cystatin C, NGAL, urinary α1-microglobulin | eGFR, urine ACR, cystatin C | Kt/V (dialysis adequacy) |
| Priority treatment | Treat cause, supportive care | RAAS blockade, SGLT-2i, BP/glycemic control | Fistula-first HD or home PD |
| RRT? | If absolute indications met | Prepare when GFR <30 | Initiate at GFR <10-15 |
This is a shared conversation. Sign in to Orris to start your own chat.