ECMO - MD ANAESTHESIA PG EXAM - 30 marks major answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed to write a comprehensive 30-mark PG anaesthesia exam answer on ECMO. Let me compose this detailed answer now.
EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO)
MD Anaesthesia PG Examination - 30 Marks
DEFINITION AND INTRODUCTION
Extracorporeal membrane oxygenation (ECMO) is a form of prolonged extracorporeal life support that provides mechanical respiratory and/or circulatory support to patients with severe, refractory cardiorespiratory failure when conventional therapies have failed. Blood is drained from the venous system, pumped through an artificial membrane oxygenator (where O2 is added and CO2 removed), and returned either to the venous system (for respiratory support) or the arterial system (for combined cardiac and respiratory support).
Historical landmarks:
-
1953: Dr. John Gibbon - first heart-lung machine for open heart surgery
-
1972: Dr. J.D. Hill - first successful prolonged extracorporeal support in an adult (75 hours) for post-trauma respiratory failure
-
1975: Dr. Robert Bartlett ("father of modern ECMO") - saved a neonate with meconium aspiration syndrome
-
2009: H1N1 influenza pandemic - landmark expansion of adult ECMO use; CESAR trial demonstrated 63% vs 47% survival with ECMO vs standard therapy
-
Miller's Anesthesia, 10e; Sabiston Textbook of Surgery
CIRCUIT COMPONENTS
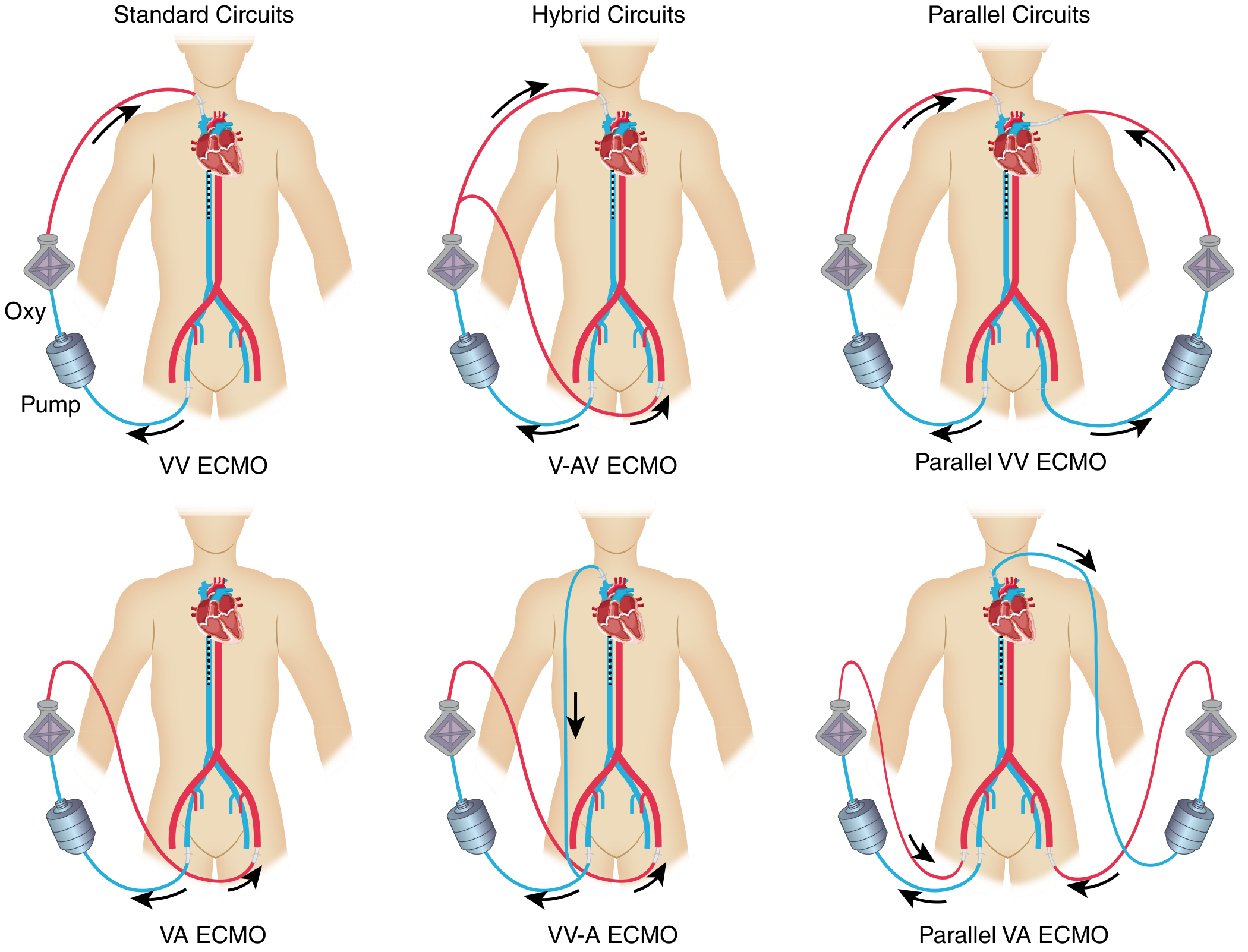
Fig. 1: Various ECMO configurations including standard, hybrid, and parallel circuits (Sabiston Textbook of Surgery)
The ECMO circuit consists of:
| Component | Function |
|---|---|
| Drainage cannula | Withdraws deoxygenated blood from venous system |
| Centrifugal pump | Creates non-occlusive flow (preferred over older roller pumps - less blood trauma) |
| Membrane oxygenator | Hollow-fibre polymethylpentene (PMP) membrane; adds O2, removes CO2 |
| Heat exchanger | Maintains blood temperature to prevent hypothermia |
| Return cannula | Returns oxygenated blood to venous (VV) or arterial (VA) circulation |
| Sweep gas | Oxygen-air blend passed across oxygenator membrane - controls CO2 removal (sweep rate) and oxygenation (FiO2) |
Key technological advances: Shift from roller pump to centrifugal pump technology; transition from silicone membrane to polymethylpentene oxygenator - reduced blood trauma and improved gas exchange. - Sabiston Textbook of Surgery, p. 2650
TYPES / CONFIGURATIONS OF ECMO
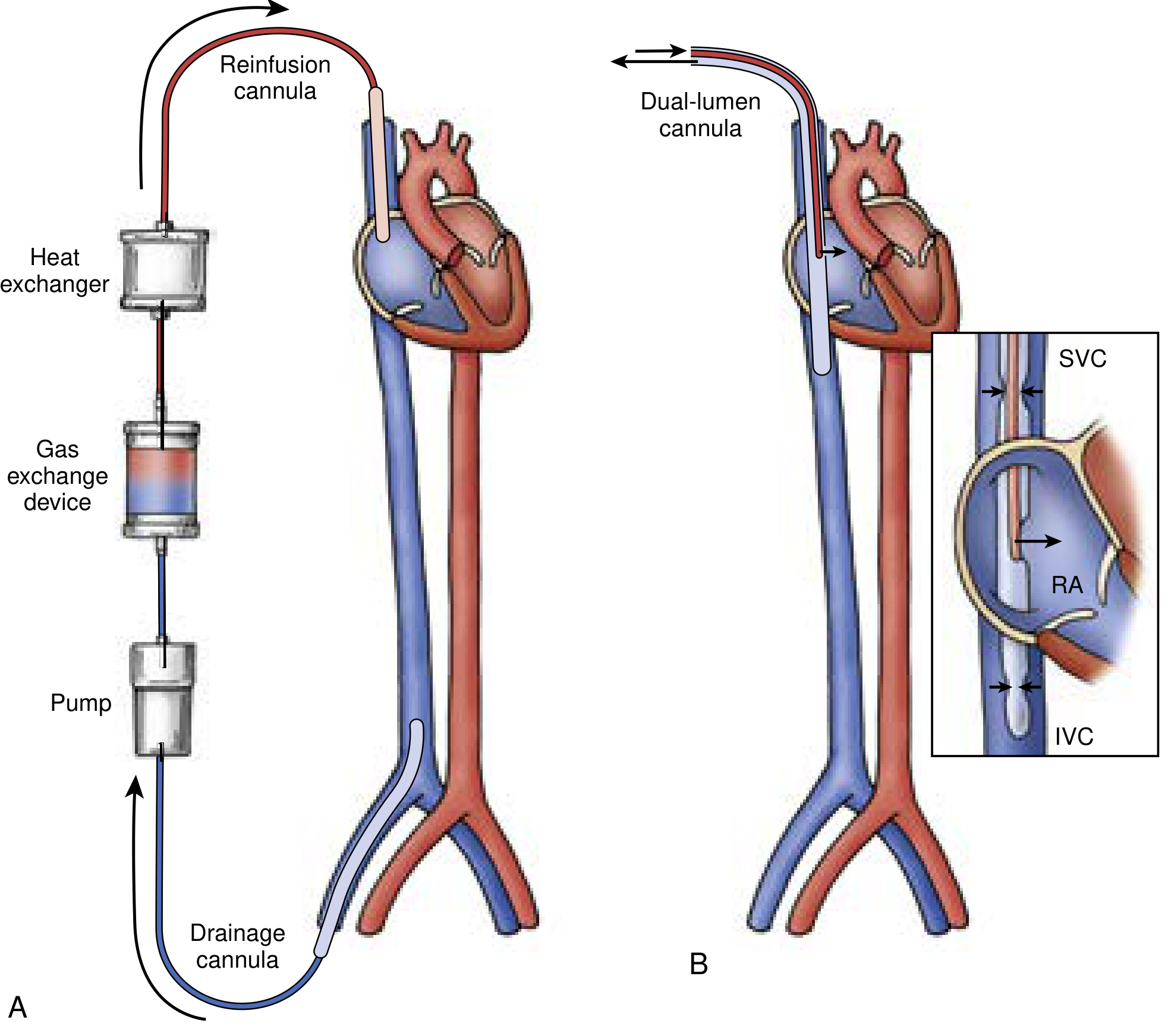
Fig. 2: Venovenous ECMO - (A) Dual-site: femoral vein drainage → IJV return; (B) Single dual-lumen cannula via right IJV draining SVC/IVC and reinfusing into RA (Current Surgical Therapy 14e)
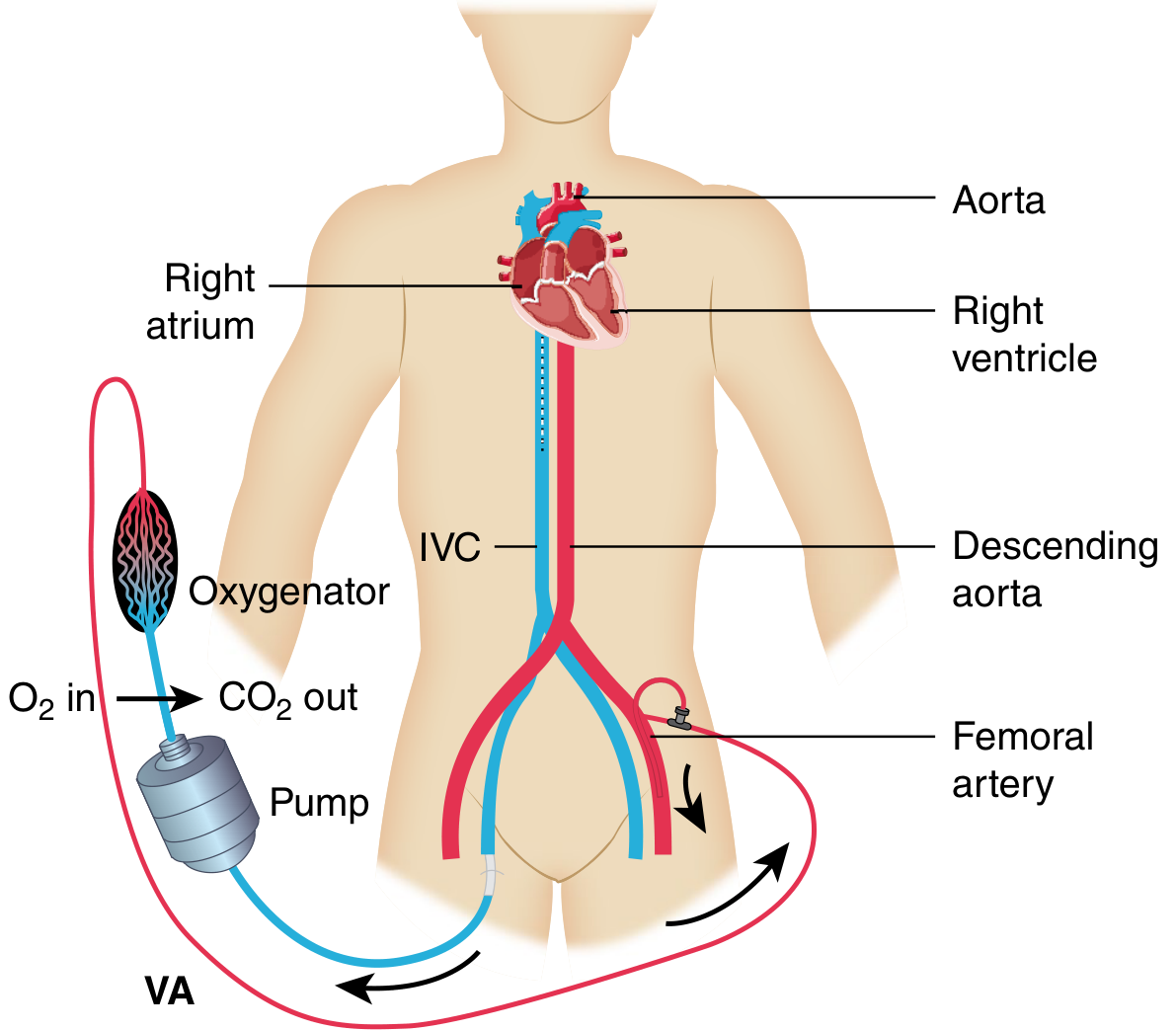
Fig. 3: Venoarterial (VA) ECMO - femoral vein drainage, femoral artery return bypassing heart and lungs (Sabiston Textbook of Surgery)
1. Venovenous ECMO (VV ECMO)
- Drainage: Femoral vein or IJV (or dual-lumen single cannula in IJV - "Avalon" cannula)
- Return: Internal jugular vein → right atrium
- Function: Respiratory support ONLY - oxygenates blood and removes CO2; requires intact cardiac function
- Hemodynamic effect: Does NOT increase cardiac output; may slightly reduce afterload via vasodilation on initiation
2. Venoarterial ECMO (VA ECMO)
- Drainage: Femoral vein / right atrium
- Return: Femoral artery / aorta (peripheral) or aorta/axillary artery (central)
- Function: Biventricular cardiac support AND respiratory support
- Hemodynamic effect: Increases MAP, reduces preload, increases systemic afterload; provides circulatory support independent of cardiac function
3. Veno-Arterio-Venous ECMO (V-AV ECMO) - Hybrid
- Returns blood to BOTH arterial and venous circulations
- Used when patient needs both respiratory and cardiac support simultaneously, or transitioning between modalities
4. Parallel / Dual-circuit ECMO
- Two separate ECMO circuits used when one circuit is insufficient
- Used in high cardiac output states (sepsis) or severe refractory hypoxia
- Risk of recirculation between circuits
INDICATIONS
VV ECMO - Respiratory Failure
Berlin criteria for severe ARDS (PaO2/FiO2 < 100 mmHg with PEEP >5 cmH2O) is the primary indication. Murray Lung Injury Score ≥3 (based on P/F ratio, PEEP, chest radiograph quadrants, lung compliance) is also used.
| Indication | Notes |
|---|---|
| Severe ARDS (P/F <100 with PEEP >5) | Most common; viral/bacterial pneumonia, H1N1, COVID-19 |
| Status asthmaticus refractory to all therapies | |
| Bridge to lung transplantation | In end-stage chronic lung disease |
| Perioperative support during lung transplantation | Preferred over CPB; less PGD |
| Post-lung transplant primary graft dysfunction |
CESAR trial (2009): VV ECMO at specialist centre - 63% vs 47% survival (RR 0.69, p=0.03)
EOLIA trial (2015): No mortality difference at 60 days (35% vs 46%, p=0.09) but 28% crossover to ECMO and 57% mortality in that crossover group - interpreted by many as supporting early ECMO.
ELSO registry: ~60% survival to discharge for adult respiratory ECMO.
VA ECMO - Cardiac Failure
| Indication | Details |
|---|---|
| Postcardiotomy failure | Failure to wean from CPB; most common indication |
| Refractory cardiogenic shock | After myocardial infarction; failed IABP/Impella/inotropes |
| Acute myocarditis | Bridge to recovery or transplant |
| Massive pulmonary embolism | Obstructive shock; buys time for thrombolysis/embolectomy |
| High-risk PCI support | Elective hemodynamic support |
| Bridge to LVAD/transplant | End-stage heart failure |
| ECPR (extracorporeal CPR) | In-hospital cardiac arrest refractory to ACLS |
| Post-cardiac transplant primary graft failure | |
| Septic cardiomyopathy | |
| Drug toxicity / toxic myocarditis |
ELSO registry: ~40% survival to discharge for adult cardiac ECMO.
- Miller's Anesthesia, 10e, p. 12118; Sabiston Textbook of Surgery, p. 2654
CONTRAINDICATIONS
Absolute:
- Irreversible condition with no possibility of recovery, transplant, or destination therapy
- Severe aortic regurgitation (VA ECMO increases afterload, worsens AR and prevents LV ejection)
- Advanced age with multiple comorbidities and no bridge therapy planned
Relative:
- Chronic terminal illness / poor baseline quality of life
- Severe neurological injury / prolonged low-flow cardiac arrest
- Prolonged mechanical ventilation (>7 days) before ECMO consideration
- Active non-compressible bleeding (especially intracranial haemorrhage)
- Severe peripheral vascular disease (for peripheral cannulation)
- Morbid obesity
CANNULATION
Peripheral (bedside, percutaneous - most common)
- Performed at bedside without surgical exposure
- Seldinger technique under fluoroscopic/echocardiographic guidance
- VV ECMO sites: Femoral vein (drainage) + right IJV (return); OR dual-lumen Avalon cannula in right IJV
- VA ECMO sites: Femoral vein (drainage) + femoral artery (return) + separate distal perfusion cannula in superficial femoral artery to prevent limb ischaemia
Central (surgical, intraoperative)
- Requires sternotomy or thoracotomy
- Direct aortic/right atrial cannulation (as in CPB)
- Reserved for postcardiotomy cases, intraoperative use, or when peripheral access is impractical
- Advantages: larger cannulas, better flows, avoids Harlequin syndrome
Role of echocardiography in cannulation:
- Subcostal view confirms guidewire position in IVC/RA junction
- Guides cannula tip placement and confirms position
- Detects pericardial effusion, cardiac thrombus, AR (contraindication to VA), LV distension on VA ECMO
MANAGEMENT ON ECMO
VV ECMO Management
Primary goal: Allow lung rest while ECMO performs gas exchange
Mechanical ventilation settings (lung-protective/ultra-protective):
- Tidal volume: 4-6 mL/kg predicted body weight
- Plateau pressure: <25 cmH2O
- Driving pressure: <15 cmH2O
- PEEP: 10 cmH2O
- RR: 10 breaths/min
- FiO2: 40%
ECMO flow and oxygenation:
- Target SaO2 >88-92%
- ECMO blood flow typically 3-5 L/min
- Oxygenation determined by: ECMO flow rate, FiO2 on sweep gas, haemoglobin level, cardiac output (ECMOBF/CO ratio)
- CO2 removal: controlled primarily by sweep gas flow rate (increase sweep = more CO2 removed)
Anticoagulation:
- Unfractionated heparin continuous infusion - target aPTT 60-80 seconds OR anti-Xa 0.3-0.7 IU/mL
- Antithrombin III (AT-III) supplementation if heparin resistance occurs
- Monitor ACT, aPTT, TEG/ROTEM
Haemoglobin target: >7 g/dL (liberal targets >10 may be used for high cardiac output states)
Problem: Recirculation in VV ECMO
- Reinfused oxygenated blood re-enters drainage cannula without entering patient's circulation
- Recognised by: high SaO2 at pump inlet, no improvement in patient oxygenation
- Management: reposition cannulas (increase distance between drainage and return), reduce pump speed, add second drainage cannula, change to dual-lumen cannula
Problem: Persistent hypoxia on VV ECMO
- Check oxygenator function (replace if P50 or pre/post oxygenator PaO2 difference reduced)
- Increase pump flow rates
- Treat recirculation
- If cardiac output very high (sepsis) - flow may be insufficient fraction of total CO
VA ECMO Management
Haemodynamic targets: MAP 65-80 mmHg; adequate cardiac pulsatility to maintain aortic valve opening
Inotropes on VA ECMO:
| Drug | Mechanism | ECMO Indication | Caution |
|---|---|---|---|
| Dobutamine | β1 agonist | Enhance LV contractility, maintain pulsatility, vasodilation | Tachyarrhythmia, ↑myocardial O2 demand |
| Milrinone | PDE-3 inhibitor | RV failure, pulmonary hypertension; improves diastolic relaxation | Hypotension; useful for weaning |
| Epinephrine | α + β agonist | Severe cardiogenic shock; maintain pulsatility | ↑myocardial O2 demand, arrhythmogenicity |
| Vasopressin | V1 agonist | Vasodilatory shock | Splanchnic vasoconstriction |
Vasopressors: Norepinephrine to maintain MAP; Phenylephrine (pure α1) when tachycardia must be avoided.
Antihypertensives: Nicardipine (first-line - titratable calcium channel blocker), Clevidipine (very short acting); avoid esmolol/labetalol on VA ECMO as they reduce pulsatility.
Goal: Minimise inotropes - allow cardiac rest. Inotropes only to maintain pulsatility and aortic valve opening. If no pulsatility: risk of LV distension, aortic root thrombus, pulmonary oedema, reduced coronary perfusion.
LV Venting / Unloading:
When VA ECMO increases afterload excessively, the LV may distend (unable to eject against increased afterload + ECMO return). Strategies:
- Intra-aortic balloon pump (IABP) - reduces afterload, improves coronary perfusion
- Impella device - directly drains LV into aorta
- Atrial septostomy (blade or balloon) - creates interatrial communication
- Surgical vent in LA/LV during open surgery
- Sabiston Textbook of Surgery, p. 2661
SPECIAL SITUATION: HARLEQUIN SYNDROME (North-South Syndrome)
Definition: A complication of peripheral VA ECMO where differential oxygenation occurs - the lower body receives well-oxygenated blood from the ECMO circuit while the upper body (including brain and coronary arteries) receives poorly oxygenated blood from the native left heart ejecting hypoxic blood from damaged lungs.
Mechanism: The ECMO return cannula in the femoral artery delivers oxygenated blood retrograde up the descending aorta. If the native heart recovers and ejects significant cardiac output, the "mixing zone" of ECMO and native blood moves down the aorta - leaving the cerebral and coronary circulations supplied by deoxygenated native cardiac output.
Monitoring: Right radial artery ABG (best estimates upper body/cerebral oxygenation); right finger SpO2.
Management:
- Increase ECMO flow to push mixing zone towards aortic arch
- Reduce inotropes to decrease native cardiac output
- Aggressive volume removal
- Convert to central cannulation
- Add second return cannula in IJV (VAV-ECMO configuration)
- Optimise mechanical ventilation to improve native lung function
PHARMACOKINETICS ON ECMO
Drug pharmacokinetics are significantly altered on ECMO:
- Sequestration: Lipophilic drugs (e.g., fentanyl, midazolam, propofol) are adsorbed onto the circuit tubing and oxygenator - substantially reduced plasma levels; dose requirements increase
- Volume of distribution: Increased due to circuit prime volume and haemodilution
- Protein binding: Altered; affects drug distribution
- Practical: Increase initial doses of sedatives and opioids; monitor drug levels where possible
WEANING FROM ECMO
Weaning VV ECMO
Signs of readiness: Improving lung compliance (increasing tidal volumes on pressure-control), improving P/F ratio, improving chest X-ray.
Process:
- Wean sweep gas FiO2 first (to 21%), then reduce sweep gas flow rate
- Wean ventilator FiO2 simultaneously
- Decannulation thresholds: FiO2 <50%, PEEP <10 cmH2O, compliance >50 mL/cmH2O, RR <20 breaths/min - sustained for ≥48 hours
- Trial of "clamping" sweep gas with the circuit still running to test native lung function
- Consider ECCO2R (extracorporeal CO2 removal at low flows) as transition if CO2 removal but not oxygenation needed
Weaning VA ECMO
Signs of readiness: Return of arterial pulsatility, improving echocardiographic LV function (LVEF >20-25%), decreasing inotrope requirements, MAP maintained without high vasopressor support.
Process:
- Gradually reduce ECMO flow (by 0.5 L/min increments)
- Monitor haemodynamics at each step
- At flows of 1-1.5 L/min, assess feasibility of decannulation
- Maintain anticoagulation until cannula removal
Decannulation
- Peripheral: cannulas removed, manual compression or surgical closure
- Post-decannulation: limb Doppler, venous duplex for DVT at 24h
- If decannulation fails: bridge to LVAD/transplant, or palliation discussion
COMPLICATIONS
Patient-related Complications
| Complication | Details |
|---|---|
| Bleeding | Most common - systemic anticoagulation required; cannula sites, surgical sites, intracranial haemorrhage, GI bleed |
| Thrombosis / Thromboembolism | Clot in circuit, oxygenator, or patient; stroke (CVA), limb DVT, PE |
| Infection | Cannula site infection, circuit colonisation, nosocomial pneumonia |
| Limb ischaemia | Femoral arterial cannula (VA ECMO) - distal perfusion cannula in SFA is mandatory |
| Harlequin syndrome | Peripheral VA ECMO; cerebral/coronary hypoxia (see above) |
| Neurological | CVA (haemorrhagic or ischaemic), seizures, rarely spinal cord ischaemia |
| Haemolysis | Mechanical red cell destruction; monitor LDH, plasma free haemoglobin, trans-membrane pressure |
| Acute kidney injury | From low flow, haemolysis, inflammatory response |
| SIRS on decannulation | Removal of indwelling cannulas triggers inflammatory response |
Circuit/Mechanical Complications
| Complication | Cause | Management |
|---|---|---|
| Low flow / "chattering" | Hypovolaemia, cannula malposition, circuit thrombosis, abdominal compartment syndrome | Fluid bolus, reposition cannula, circuit change |
| Oxygenator failure | Clot in oxygenator, plasma leakage | Oxygenator exchange (circuit change) |
| Air embolism | Circuit disconnection, de-airing failure | Clamp, aspirate, remove air |
| Pump malfunction | Power failure, pump head failure | Back-up pump on standby; hand crank available |
| Cannula dislodgement | Patient movement | Secure cannulas; sedation |
- Sabiston Textbook of Surgery, p. 2665-2666
ANTICOAGULATION IN ECMO
- Heparin infusion is the standard; titrated to aPTT 60-80 sec or anti-Xa 0.3-0.7 IU/mL
- AT-III deficiency causes heparin resistance - supplement AT-III or use bivalirudin
- Bivalirudin - alternative in heparin-induced thrombocytopenia (HIT)
- No anticoagulation ECMO - short runs or high bleeding risk; evidence emerging but not standard
- Monitor: ACT, aPTT, anti-Xa, platelet count, fibrinogen, TEG/ROTEM
- Target platelet count >80,000/µL; fibrinogen >200 mg/dL
ECMO IN SPECIFIC SCENARIOS (Anaesthesia Context)
ECPR (Extracorporeal CPR)
- ECMO initiated during CPR for refractory in-hospital cardiac arrest
- Requires rapid cannulation team (ideally within 60 minutes of arrest)
- Best outcomes: witnessed arrest, CPR duration <60 min, reversible cause, age <65 years
- ELSO guidelines recommend consideration when conventional CPR fails within 10-15 minutes
ECMO During Lung Transplantation
- VA ECMO preferred intraoperatively (surgical manipulation causes haemodynamic instability + one-lung ventilation in end-stage lung disease)
- Advantages over CPB: less inflammatory response, less primary graft dysfunction (PGD), better short and long-term outcomes
- Post-transplant: VV or VA ECMO for PGD, RV failure, LV failure
ECMO During High-Risk Cardiac Procedures
- Pre-procedural prophylactic ECMO support for high-risk PCI
- Anaesthetic consideration: arterial line in right radial artery (for upper body ABG in VA ECMO), central venous access, invasive haemodynamic monitoring
ELSO (EXTRACORPOREAL LIFE SUPPORT ORGANISATION) GUIDELINES - KEY POINTS
| Category | Survival to Discharge |
|---|---|
| Neonatal respiratory | ~75% |
| Paediatric respiratory | ~57% |
| Adult respiratory (ARDS) | ~60% |
| Adult cardiac | ~40% |
| ECPR (adult) | ~29% |
ANAESTHESIA CONSIDERATIONS - KEY POINTS FOR EXAM
- Monitoring: Invasive arterial line in right radial artery for VA ECMO (best proxy for upper body oxygenation, especially in Harlequin syndrome); additional CVP, PA catheter or TOE/TTE
- Drug dosing: Significantly increased doses of lipophilic drugs (fentanyl, propofol, midazolam) due to circuit sequestration; monitor drug levels
- Lung rest ventilation: Ultra-protective on VV ECMO (Vt 4-6 mL/kg, plateau <25 cmH2O, driving pressure <15 cmH2O)
- LV distension on VA ECMO: Recognised by loss of arterial pulse pressure; treat with IABP/Impella/septostomy
- Anticoagulation: Continuous heparin; frequent monitoring; reverse with protamine at decannulation
- Temperature: Heat exchanger in circuit; avoid hyperthermia (increases O2 demand) and hypothermia (coagulopathy, arrhythmia)
- Recirculation in VV ECMO: Suspected when circuit looks "too red" or patient not improving; managed by repositioning cannulas
SUMMARY TABLE: VV vs VA ECMO
| Feature | VV ECMO | VA ECMO |
|---|---|---|
| Drainage | Femoral vein / IJV | Femoral vein / RA |
| Return | IJV / RA | Femoral artery / Aorta |
| Cardiac function required | Yes | No |
| Support provided | Respiratory only | Respiratory + Cardiac |
| Pulsatility maintained | Yes (native) | May be lost |
| Main indication | ARDS, respiratory failure | Cardiogenic shock, ECPR |
| Specific complication | Recirculation | Harlequin syndrome, LV distension |
| Survival (adult) | ~60% | ~40% |
REFERENCES (Textbook Sources)
- Miller's Anesthesia, 10e - Chapters 49, 81, 33
- Sabiston Textbook of Surgery - Chapter 116
- Fishman's Pulmonary Diseases and Disorders - Chapter 31
- Current Surgical Therapy, 14e
- Murray & Nadel's Textbook of Respiratory Medicine
Word count note for examiner: This answer covers definition, history, circuit components, types/configurations (VV/VA/hybrid), indications (with evidence - CESAR/EOLIA trials), contraindications, cannulation techniques, management (ventilation, haemodynamics, anticoagulation, inotropes), special complications (Harlequin syndrome, LV distension, recirculation), weaning criteria and process, pharmacokinetics, ECPR, and anaesthesia-specific considerations - providing comprehensive coverage for a 30-mark essay expected at the MD Anaesthesia level.
This is a shared conversation. Sign in to Orris to start your own chat.