Here is a comprehensive 10-mark answer on Whiplash Injury:
WHIPLASH INJURY (Whiplash-Associated Disorder - WAD)
DEFINITION
Whiplash injury is an indirect injury to the neck caused by an acceleration-deceleration incident resulting in a flexion-extension injury of the cervical spine, without direct trauma. The term "whiplash" implies amplification of relatively small forces into larger ones. The resulting functional impairment is termed Whiplash-Associated Disorder (WAD).
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2
MECHANISM OF INJURY
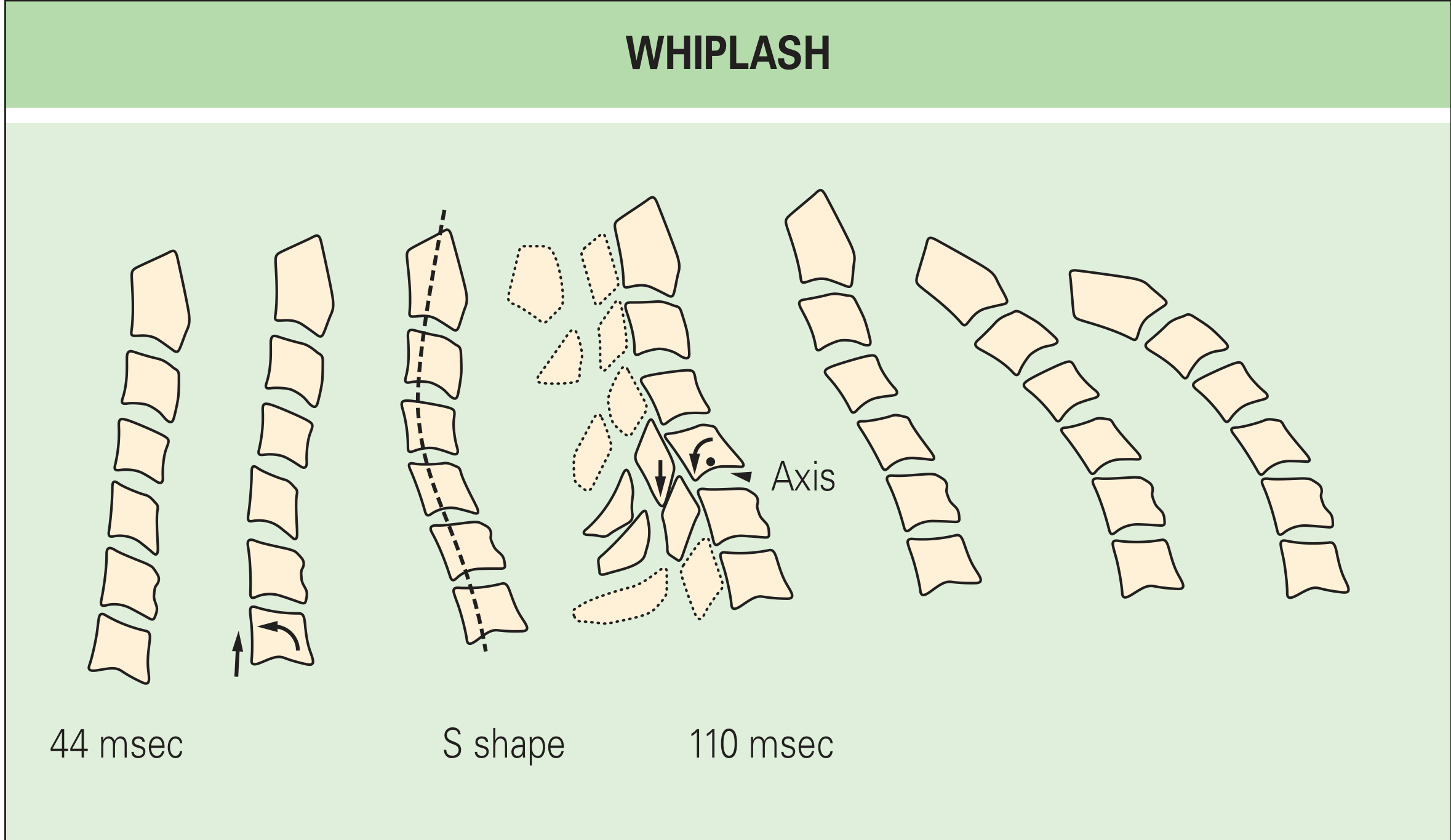
The traditional view of simple hyperextension is overly simplistic. Modern biomechanical studies have revealed a more complex sequence:
In a rear-end collision:
- The lower cervical spine is thrust upward and forward by inertial loading
- The lower segments undergo extension while upper segments remain in relative flexion
- This creates a characteristic "S-shape" deformity at ~100 msec
- Movement occurs around abnormal axes of rotation (pathologic axes higher than normal)
- The anterior end of the vertebra separates from the body below; posteriorly, the inferior articular process chisels into the superior articular process
- Thereafter, all segments undergo full extension and the head is thrown forward
The zygapophyseal (facet) joints are particularly susceptible due to rotation through these abnormal axes.
Sequential radiographs of the cervical spine during whiplash. At 110 msec, C5 rotates about an abnormally high axis, separating anteriorly from C6 while the inferior articular process chisels into the superior articular process of C6. - Rheumatology, 2-Volume Set (Elsevier 2022)
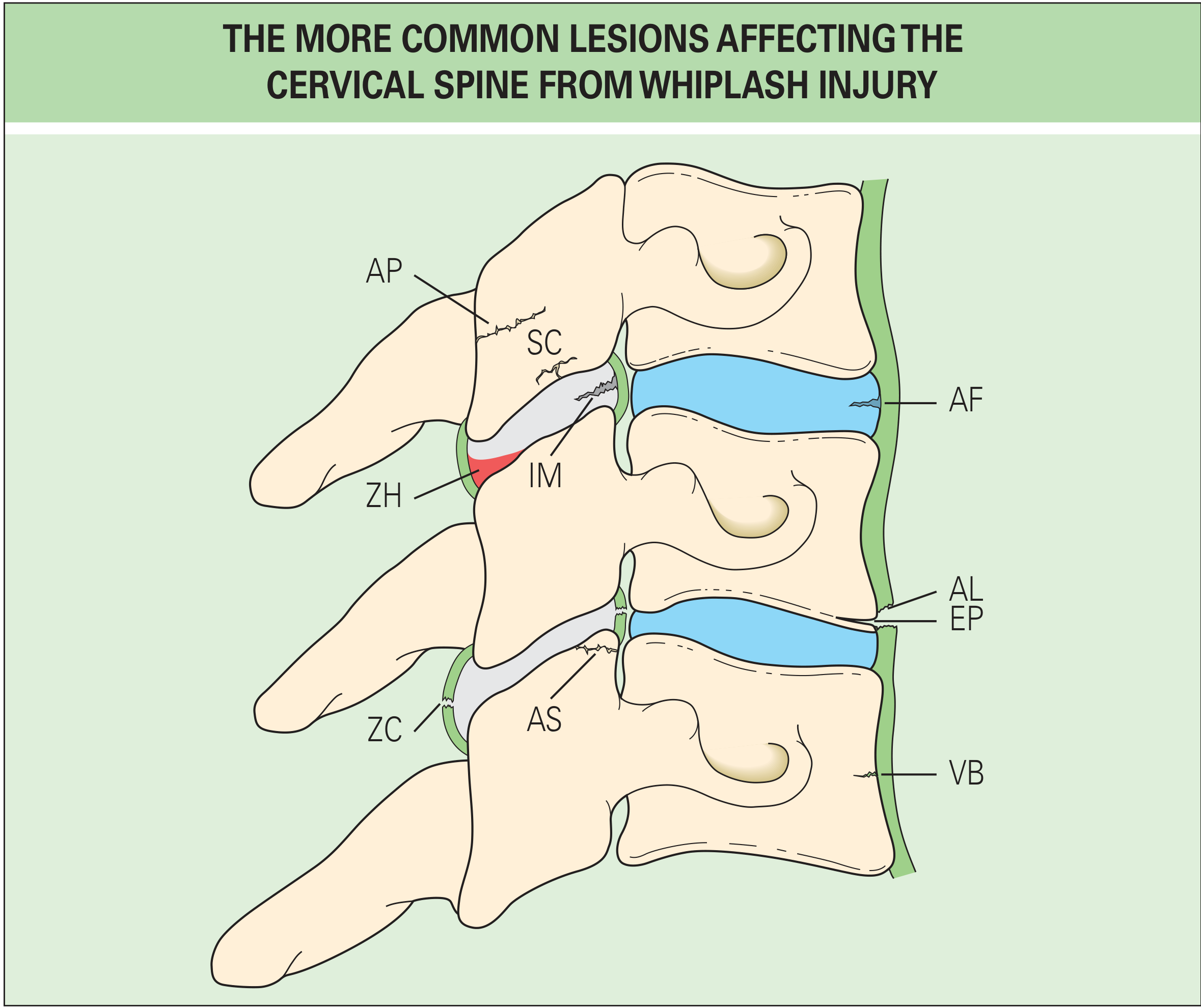
PATHOLOGY
The common structural lesions from whiplash injury are:
Common lesions of the cervical spine in whiplash. Key structures: AF = annulus fibrosus tear; ZC = zygapophyseal joint capsule rupture; ZH = hemarthrosis; IM = intraarticular meniscus contusion; EP = endplate avulsion; VB = vertebral body fracture - Rheumatology, 2-Volume Set (Elsevier 2022)
Plain radiographs detect only ~4 out of 245 injuries even under optimal conditions - they are profoundly insensitive to all but the most severe bony injuries.
EPIDEMIOLOGY
- Incidence: 70-300 per 100,000 population
- Over 1 million new cases per year in the US
- 85% of cases are from rear-end motor vehicle collisions
- UK: 250,000 patients per year at an estimated cost of £3 billion
- Risk increases with seat belt use (paradoxically - 268% increase after mandatory seat belt law)
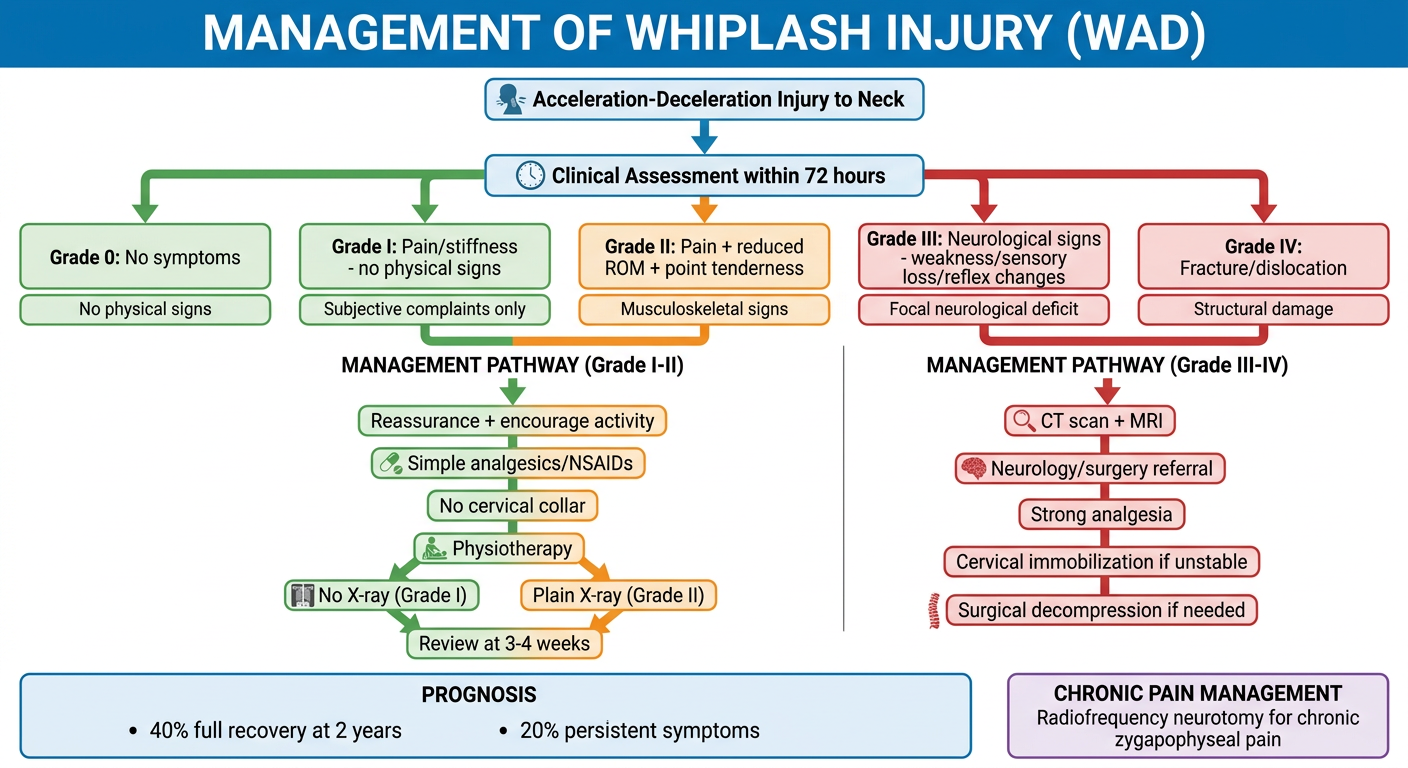
CLASSIFICATION - Quebec Task Force (QTF, 1995)
Symptoms/signs must occur within 72 hours to be attributable to the trauma.
| Grade | Symptoms and Signs |
|---|
| 0 | No symptoms, no physical signs |
| I | Pain/stiffness/tenderness on motion - NO physical signs on examination |
| II | Pain + musculoskeletal signs: reduced range of motion, point tenderness |
| III | Grade II + neurological signs: weakness, sensory loss, absent/reduced reflexes, long-tract signs |
| IV | Fracture and/or dislocation of the cervical spine |
- 90% of all whiplash claims fall under Grade I and II
- Grade III involves nerve root compression (e.g., disc herniation)
CLINICAL FEATURES
Acute symptoms (within 72 hours):
- Neck pain and stiffness (most common)
- Headache (occipital, often referred)
- Shoulder and arm pain
- Restricted cervical range of motion
- Dizziness/vertigo (particularly in Grade III)
- Visual disturbances
- Dysphagia
Signs by grade:
- Grade I: normal examination
- Grade II: reduced ROM, point tenderness, muscle spasm
- Grade III: reduced/absent deep tendon reflexes, weakness, dermatomal sensory loss
Less common features:
- Cognitive symptoms (~20% of patients)
- Tinnitus (not attributable to minor Grade I-II injury; tinnitus is not a persisting feature in Grade I-II)
- Subjective hearing loss (13% of cases)
- Benign Paroxysmal Positional Vertigo (most common vestibular complaint, usually Grade III)
INVESTIGATIONS / IMAGING
| Grade | Imaging Recommendation |
|---|
| I | No X-ray (exceptions: age >65, concurrent skeletal disease, prior neck surgery) |
| II | Plain X-ray or CT (CT mandatory if any nerve root or cord symptoms) |
| III | CT mandatory + MRI often indicated |
| IV | CT + MRI (urgent surgical assessment) |
Adapted from NICE guidelines and Jansen et al. - Scott-Brown's Otorhinolaryngology, Vol 2
MANAGEMENT FLOWCHART
TREATMENT
Acute WAD (Grade I-II):
- Encourage activity - activation is superior to rest; cervical collars and passive modalities are inferior and should be avoided
- Simple analgesics (paracetamol); NSAIDs for 3 weeks maximum
- Opioids not recommended for Grade I; only for VAS >8 in Grade II-III and for <2 weeks
- Muscle relaxants: no proven efficacy
- Systemic steroids: no benefit over placebo
- Reassurance and psychological support
- Physiotherapy with active exercise
Acute WAD (Grade III):
- NSAIDs + nonopioid analgesics
- Short-term opioids if severe pain
- Neurology/surgical referral
- CT + MRI imaging
WAD Grade IV:
- Urgent orthopedic/neurosurgical referral
- Cervical immobilization
- Surgical decompression if indicated
Chronic Whiplash:
- Percutaneous radiofrequency neurotomy - the single most promising treatment for constant, debilitating zygapophyseal joint pain (palliative but valuable)
- Exercise therapy
- Cognitive behavioral therapy for psychological components
- Acupuncture: a 2024 systematic review (Lee et al., BMJ Open, PMID 38233056) found benefit for whiplash-related pain
PROGNOSIS
| Outcome | Grade I | Grade II | Grade III |
|---|
| Neck pain >6 months | 44% | 81% | Up to 90% |
| Headache >6 months | 37% | 37% | 70% |
- ~40% of patients report complete recovery at 2 years
- ~45% continue to have major complaints at 2 years
- ~20% have persistent symptoms overall
- Grade I-II: 97-100% recover within 1 year
- Whiplash injury is extremely unlikely at speeds under 3 mph (4.8 km/h)
- Compensation/litigation significantly worsens prognosis
MEDICOLEGAL IMPORTANCE
- Whiplash is one of the most common causes of personal injury claims
- The QTF emphasizes it is essentially a benign condition but a refractory minority accounts for disproportionate costs
- Studies from Lithuania (where litigation is uncommon) showed far less symptomatology than comparable US accidents - highlighting the role of psychological and compensation factors
- Cognitive symptoms claimed by ~20% are likely functional or malingering in many cases
Bradley and Daroff's Neurology in Clinical Practice; Rheumatology, 2-Volume Set (Elsevier 2022); Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2
Key takeaway: Whiplash/WAD is classified Grade 0-IV by the Quebec Task Force (1995). The S-shape biomechanics explain zygapophyseal joint vulnerability. Treatment for Grade I-II centers on active mobilization, not rest or collar, and prognosis is generally good, though a significant minority develop chronic symptoms requiring radiofrequency neurotomy.