Midget rotation embryology 5M answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive information from both The Developing Human and Langman's Medical Embryology. Here is a complete 5-mark answer:
Midgut Rotation - Embryology (5 Marks)
Overview
The midgut is the segment of the primitive gut supplied by the superior mesenteric artery (SMA). It extends from the duodenojejunal junction to the mid-transverse colon. Rapid elongation of the midgut outstrips the growth of the abdominal cavity, forcing it to herniate and rotate.
The Primary Intestinal Loop
The midgut forms a U-shaped primary intestinal loop with two limbs:
| Limb | Derivative |
|---|---|
| Cranial limb | Jejunum and ileum (elongates rapidly into coils) |
| Caudal limb | Cecum, appendix, ascending colon, proximal 2/3 of transverse colon |
The apex of the loop is attached to the omphaloenteric (vitelline) duct, which connects to the yolk sac.
Stages of Midgut Rotation
Stage 1 - Physiological Herniation and 90° Rotation (Week 6)
- The midgut loop herniates into the umbilical cord (extraembryonic coelom) at Week 6, due to rapid gut elongation and relatively small abdominal cavity.
- During herniation, the loop rotates 90° counterclockwise around the axis of the SMA (when viewed from the front).
- This brings:
- Cranial limb (small intestine) → to the right
- Caudal limb (large intestine) → to the left
Stage 2 - Retraction and further 180° Rotation (Week 10)
- During Week 10, the herniated loops return to the abdominal cavity (reduction of midgut hernia). Factors facilitating this:
- Expansion of the abdominal cavity
- Regression of the mesonephric kidney
- Relative decrease in size of the liver
- As the large intestine re-enters, it undergoes a further 180° counterclockwise rotation
- Total rotation = 90° + 180° = 270° counterclockwise around the SMA axis
Order of Return:
- Small intestine (cranial limb) returns first - passes posterior to the SMA - occupies the central and left abdomen
- Cecum is the last to return - temporarily sits in the right upper quadrant under the right lobe of liver
- Cecum then descends to the right iliac fossa, placing the ascending colon and hepatic flexure on the right side
- The appendix forms as a narrow diverticulum from the distal cecal bud during this descent
Diagram
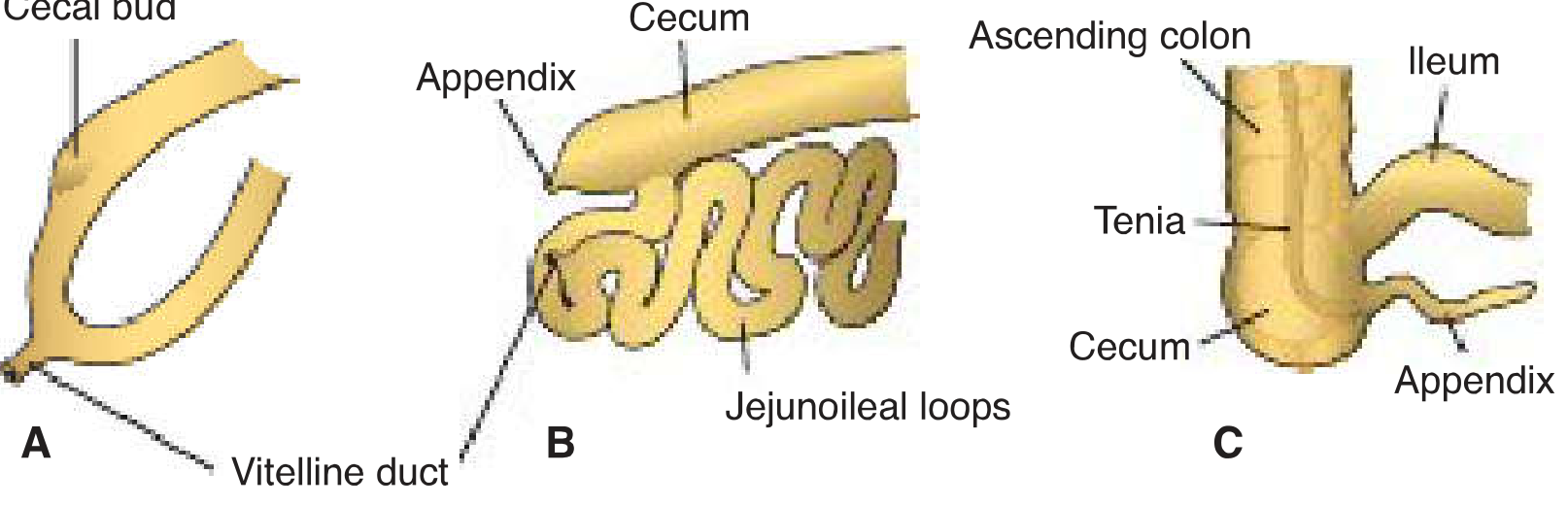
Successive stages in development of the cecum and appendix - Langman's Medical Embryology
Fixation of the Intestines
- Rotation of the stomach and duodenum causes the duodenum and pancreas to fall retroperitoneally (their mesentery is absorbed)
- The ascending colon and descending colon become retroperitoneal as their mesenteries fuse with the posterior abdominal wall
- Segments retaining free mesentery: jejunum/ileum (mesentery proper), transverse colon, sigmoid colon, rectum
Anomalies of Midgut Rotation (Clinical Correlates)
| Anomaly | Mechanism | Consequence |
|---|---|---|
| Malrotation | Failure to complete 270° rotation | Cecum stays in upper abdomen; duodenum at risk |
| Ladd's bands | Abnormal peritoneal bands from cecum to posterior wall crossing the duodenum | Duodenal obstruction |
| Midgut volvulus | Narrow mesenteric base (due to malrotation) allows gut to twist around SMA | Intestinal ischemia/necrosis - surgical emergency |
| Reversed rotation | Clockwise instead of counterclockwise rotation | Transverse colon behind duodenum |
| Non-rotation | Gut returns without rotating | Small bowel on right, large bowel on left |
Key Points Summary (Exam-Ready)
- Axis of rotation = Superior Mesenteric Artery
- Direction = Counterclockwise (when viewed from front/anterior)
- Total rotation = 270° (90° during herniation + 180° during return)
- Timing: Herniation at Week 6; return at Week 10
- Cecum descends last - from right upper quadrant to right iliac fossa
- Appendix forms from distal cecal bud during cecal descent
- Clinical: Malrotation → Ladd's bands → duodenal obstruction; narrow mesenteric base → midgut volvulus
Sources: The Developing Human: Clinically Oriented Embryology, p. 634-636; Langman's Medical Embryology, p. 266-267
Neural tube development 5m answer
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have everything needed for a comprehensive answer. Here it is:
Neural Tube Development (Neurulation) - 5 Marks
Definition
Neurulation is the process by which the neural plate forms, folds, and closes to produce the neural tube - the primordium of the entire central nervous system (brain and spinal cord). It is completed by the end of Week 4.
Step-by-Step Process
Step 1 - Induction of the Neural Plate (Day 18)
- The notochord (derived from mesoderm) induces the overlying embryonic ectoderm to thicken
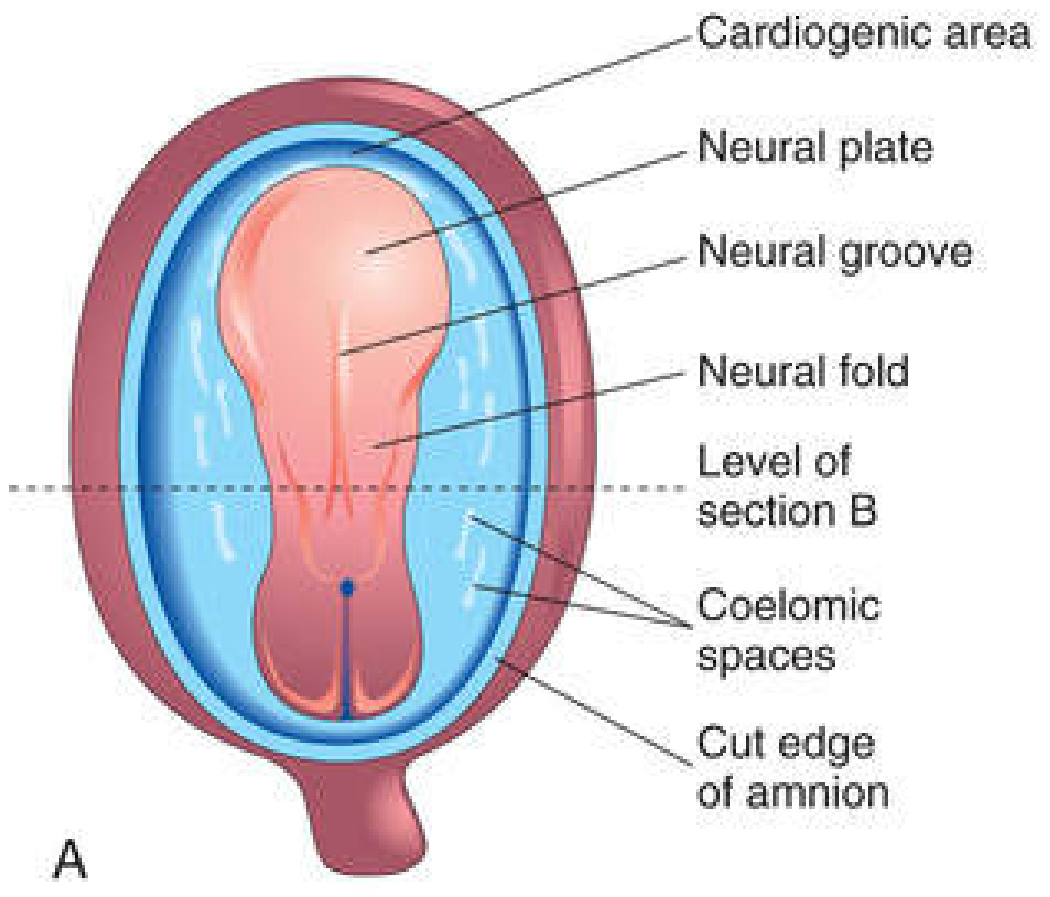
- This thickened region of ectoderm forms the neural plate - an elongated slipper-shaped structure of pseudostratified columnar neuroepithelium
- The neural plate is located rostral to the primitive node, dorsal to the notochord
- As the notochord elongates, the neural plate broadens cranially as far as the oropharyngeal membrane
- Molecular inducers: FGF, Wnt, BMP inhibitors (Noggin, Chordin, Follistatin)
Step 2 - Neural Groove and Neural Folds (Day 18-20)
- On approximately Day 18, the neural plate invaginates along its central axis to form a longitudinal midline neural groove
- The elevated lateral edges form the neural folds
- The neural folds are especially prominent cranially - these are the first signs of brain development
Step 3 - Fusion of Neural Folds (Day 22 onward)
- By the end of Week 3, neural folds begin to approach each other in the midline and fuse
- Fusion begins in the cervical region (at the level of the 5th somite) and proceeds both cranially and caudally (like a zipper)
- The neural tube soon separates from the surface ectoderm as the folds fuse - the surface ectoderm later forms the overlying skin
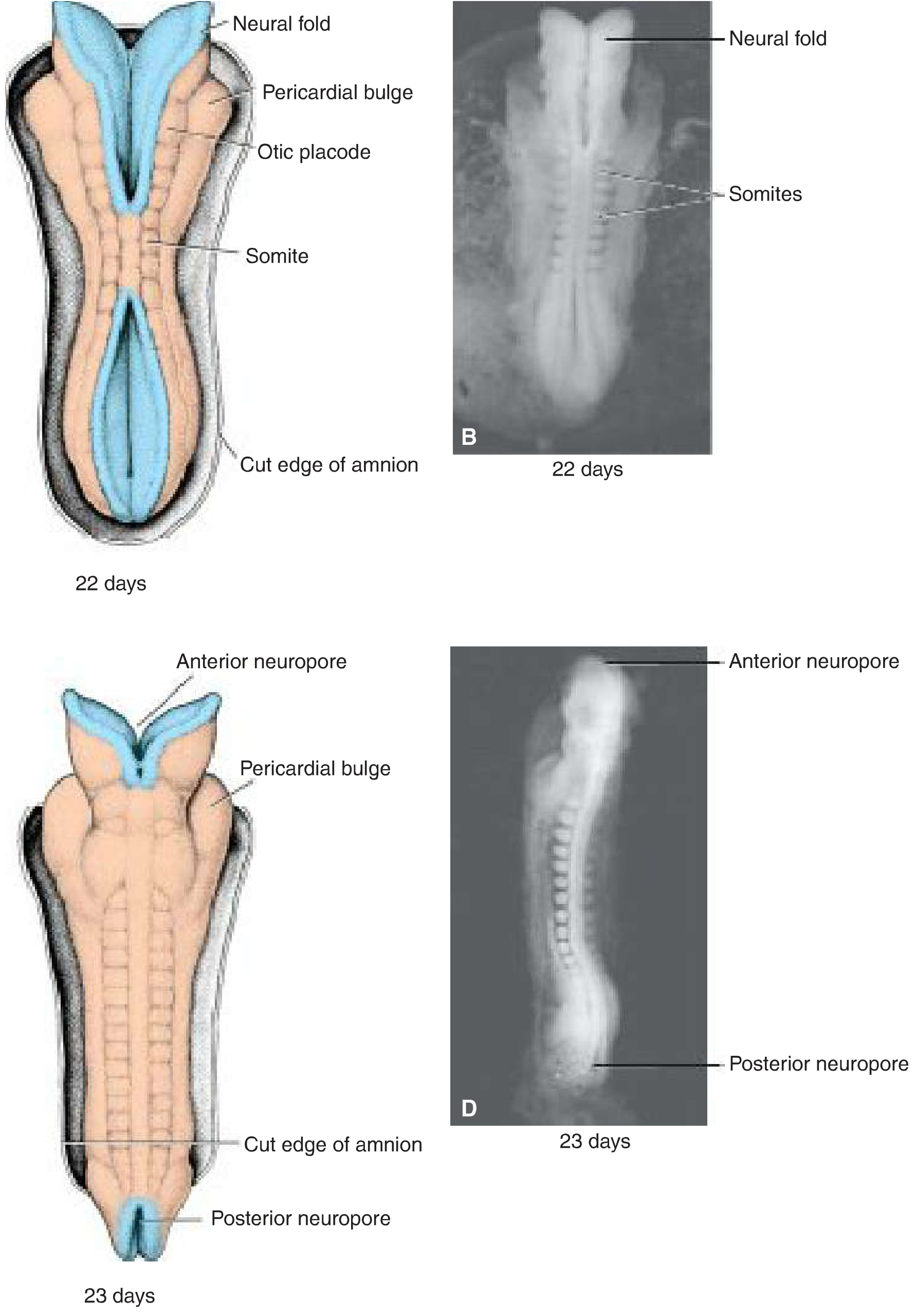
Step 4 - Closure of Neuropores (Days 25-28)
Until fusion is complete, the open cranial and caudal ends of the neural tube communicate with the amniotic cavity:
| Neuropore | Closure Day | Somite Stage |
|---|---|---|
| Anterior (cranial) neuropore | Day 25 | 18-20 somite stage |
| Posterior (caudal) neuropore | Day 28 | 25 somite stage |
- After both neuropores close, neurulation is complete
- The CNS is now represented by a closed tubular structure
Primary vs. Secondary Neurulation
| Feature | Primary Neurulation | Secondary Neurulation |
|---|---|---|
| Region | Entire neural tube cranial to S2 | Caudal to posterior neuropore (S2 downward) |
| Mechanism | Folding and fusion of neural plate | Canalization of solid cord of cells |
| Timing | Weeks 3-4 | Later in development |
Neural Crest Cells
- As the neural folds fuse, neural crest cells separate bilaterally from the fusing lips of the closing neural tube
- They migrate along predetermined pathways and differentiate into:
- Peripheral nervous system (dorsal root ganglia, autonomic ganglia)
- Schwann cells
- Chromaffin tissue (adrenal medulla)
- Melanocytes
- Craniofacial structures (cartilage, bone)
- Some scholars regard neural crest as a 4th germ layer
Derivatives of the Neural Tube
After closure, the cranial end expands into 3 primary brain vesicles:
| Primary Vesicle | Secondary Division | Adult Derivative |
|---|---|---|
| Prosencephalon (forebrain) | Telencephalon + Diencephalon | Cerebral hemispheres, thalamus, hypothalamus |
| Mesencephalon (midbrain) | Mesencephalon | Midbrain |
| Rhombencephalon (hindbrain) | Metencephalon + Myelencephalon | Pons/cerebellum, medulla |
The caudal part of the neural tube becomes the spinal cord (caudal to the 4th somite).
Wall Layers of the Neural Tube
The wall of the neural tube forms 3 zones:
- Ventricular zone (ependymal layer) - gives rise to all neurons and macroglial cells
- Intermediate (mantle) zone - becomes grey matter
- Marginal zone - becomes white matter (axons grow in)
Neural Tube Defects (NTDs) - Clinical Correlates
Failure of neural tube closure leads to NTDs. There are 5 proposed closure sites:
| Defect | Site of Failure | Result |
|---|---|---|
| Spina bifida cystica | Site 1 failure | Posterior vertebral arch defect with spinal cord exposure |
| Anencephaly | Site 2 failure | Absence of forebrain/cranial vault |
| Craniorachischisis | Sites 2, 4, and 1 | Combined open defect |
| Meroencephaly | Site 2 failure | Partial brain absence |
Risk reduction: Periconceptional folic acid supplementation (400 mcg/day) significantly reduces NTD risk by supporting proper neural tube closure.
Key Points Summary
- Neurulation = neural plate → neural groove → neural folds → neural tube closure
- Induced by the notochord
- Fusion starts at cervical (5th somite) level, proceeds bidirectionally
- Cranial neuropore closes Day 25; Caudal neuropore closes Day 28
- Neural crest cells emigrate at the time of tube closure
- 3 primary brain vesicles form at the cranial end
- NTDs = failure of closure; prevented by folic acid
Sources: The Developing Human: Clinically Oriented Embryology, p. 205-206; Langman's Medical Embryology, p. 94-95; Bradley and Daroff's Neurology in Clinical Practice, p. 1863
This is a shared conversation. Sign in to Orris to start your own chat.