Clinical discussion about pih
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertensive disorders pregnancy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive material from 5 major textbooks. Let me compile the full clinical discussion.
Pregnancy-Induced Hypertension (PIH) - Clinical Discussion
Definition & Classification
Hypertension complicates up to 8-10% of all pregnancies and is one of the leading causes of maternal and perinatal morbidity and mortality worldwide. The umbrella term "Pregnancy-Induced Hypertension (PIH)" encompasses several distinct entities:
| Category | Definition |
|---|---|
| Gestational Hypertension | New BP ≥140/90 mmHg after 20 weeks, no proteinuria, resolves postpartum |
| Preeclampsia | Gestational HTN + proteinuria (>300 mg/24 hr) or end-organ damage |
| Eclampsia | Seizures/coma in a patient with signs of preeclampsia |
| HELLP Syndrome | Hemolysis + Elevated Liver enzymes + Low Platelets |
| Superimposed Preeclampsia | Chronic HTN with new-onset preeclampsia features |
| Chronic/Coincidental HTN | Present before pregnancy or persists >6 weeks postpartum |
(Rosen's Emergency Medicine)
Epidemiology & Risk Factors
- Incidence of PIH: 2-7% of pregnancies; ~85 per 1000 deliveries in the US have hypertensive disorders of pregnancy
- Eclampsia remains a major cause of maternal mortality, though its incidence is declining with better management
Key risk factors:
- Nulliparity - highest population attributable fraction (~32%)
- Age extremes (very young, older women)
- Prior preeclampsia
- Twin/molar pregnancies
- Chronic hypertension (25% go on to develop preeclampsia)
- Diabetes mellitus (20% overall risk; up to 70% with class F/R diabetes)
- Chronic renal failure
- Antiphospholipid syndrome, SLE
- Family history of PIH
- Obesity, hypercholesterolemia
- African-American race (associated with more severe disease)
- In vitro fertilization
(Creasy & Resnik's Maternal-Fetal Medicine)
Pathophysiology
The central mechanism is insufficient uteroplacental blood flow, but the cascade that follows involves multiple systems.
Normal vs. Preeclamptic Spiral Artery Remodeling
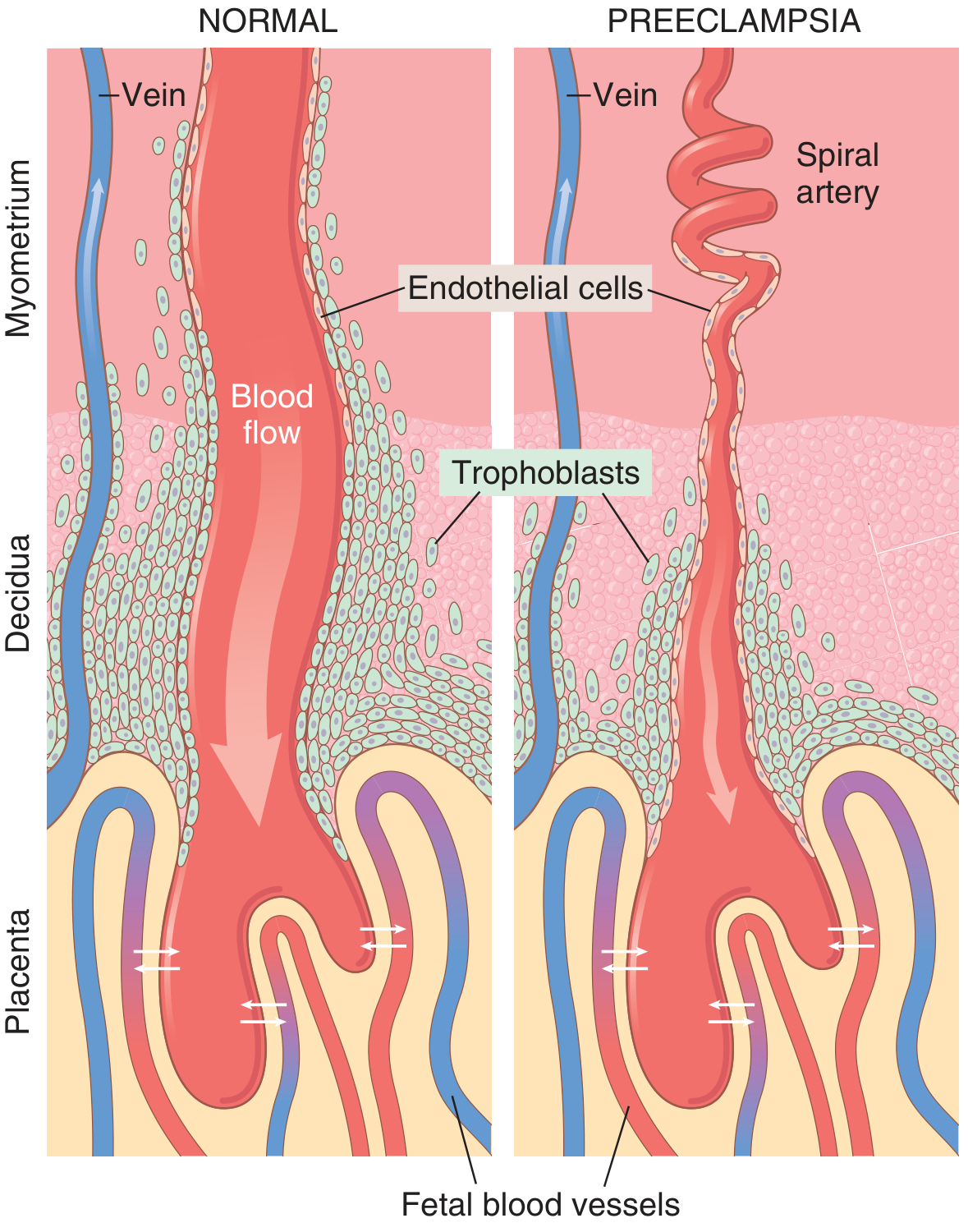
In normal pregnancy, trophoblasts invade the spiral arteries of the uterine endometrium, converting them into wide, low-resistance vascular sinusoids. In preeclampsia, this invasion fails - the vessels remain narrow and tortuous, resulting in relative placental ischemia.
Step-by-Step Cascade
- Failed trophoblast invasion of spiral arteries → narrow, high-resistance vessels retained
- Placental hypoxia/ischemia → placenta releases circulating factors
- Anti-angiogenic proteins released into maternal circulation:
- Soluble sFlt-1 (soluble fms-like tyrosine kinase-1) - antagonizes VEGF
- Soluble endoglin - antagonizes TGF-β
- These factors cause widespread maternal vascular endothelial dysfunction
- Inflammatory cytokines (TNF-α, IL-6) amplify the injury
- Downstream consequences:
| Mechanism | Clinical Consequence |
|---|---|
| Reduced prostacyclin (PGI₂) + increased thromboxane A₂ | Hypertension (vasoconstriction) |
| Endothelial dysfunction, decreased antithrombotic factors | Hypercoagulability, DIC |
| Decreased renal blood flow & GFR; glomerular basement membrane deposits | Proteinuria, oliguria |
| Hepatic microangiopathy | Elevated LFTs, epigastric pain |
| Thrombocytopenia from platelet consumption | Low platelets |
| Placental infarction from chronic hypoperfusion | Fetal growth restriction, abruption |
| Cerebral vasospasm | Headache, visual disturbances, seizures |
(Guyton & Hall; Robbins & Kumar Basic Pathology)
- Normal pregnancy is a high-output, low-resistance state
- In early PIH: cardiac output rises even further, then peripheral resistance rises abnormally
- In established preeclampsia: cardiac output drops as TPR rises markedly
Clinical Features
Diagnostic Criteria for Preeclampsia
Minimum criteria:
- BP ≥ 140/90 mmHg on 2 occasions ≥4 hours apart, after 20 weeks
- PLUS one of:
- Proteinuria >300 mg/24-hr urine, OR
- Protein:creatinine ratio ≥0.3, OR
- Signs of end-organ damage (see below)
Severe Features (any one warrants severe designation):
- BP ≥ 160/110 mmHg
- Thrombocytopenia (<100,000/µL)
- Impaired hepatic function (AST/ALT >2x normal, severe RUQ/epigastric pain)
- Renal insufficiency (creatinine >1.1 mg/dL or doubling of creatinine)
- Pulmonary edema
- New-onset headache unresponsive to medication
- Visual disturbances
Clinical Presentation Timeline
- Most commonly appears after 34 weeks, but earlier in women with molar pregnancy, preexisting renal disease, or coagulopathies
- Edema - particularly facial/periorbital; weight gain
- Headache - frontal or occipital, severe
- Visual symptoms - scotomata, blurring, photophobia
- Epigastric/RUQ pain - hepatic capsule stretching or HELLP
- Oliguria - renal involvement
- Seizures - eclampsia
HELLP Syndrome
A particularly dangerous complication occurring in ~10% of severe preeclampsia cases:
| Component | Criteria |
|---|---|
| H - Hemolysis | Microangiopathic hemolytic anemia on smear |
| EL - Elevated Liver enzymes | ALT/AST >70 U/L |
| LP - Low Platelets | Platelet count <100,000/mL |
- May be complicated by DIC
- Can occur without hypertension or proteinuria initially
- High maternal and fetal mortality if unrecognized
(Rosen's Emergency Medicine)
Investigations (Baseline Workup)
| System | Tests |
|---|---|
| Renal | Urinalysis, spot protein:creatinine, 24-hr urine protein, serum creatinine, uric acid |
| Hematologic | CBC with platelets, peripheral smear, coagulation profile (PT/aPTT, fibrinogen) |
| Hepatic | AST, ALT, LDH, bilirubin |
| Fetal wellbeing | Fetal biometry, NST/BPP, umbilical artery Doppler |
| Neurological | CT/MRI brain if focal deficits or seizures of unclear etiology |
Management
Guiding Principles
"Delivery is the only cure for preeclampsia." - The definitive treatment is delivery once the fetus is mature or the mother's condition deteriorates.
1. Blood Pressure Targets
- Threshold to treat: Diastolic >105 mmHg OR systolic >160 mmHg
- Goal: Lower BP by 15-20%, targeting systolic 140-150 mmHg and diastolic 90-100 mmHg
- Avoid over-rapid lowering - can cause uterine hypoperfusion
2. Antihypertensive Drugs in Pregnancy
| Drug | Route | Dose | Notes |
|---|---|---|---|
| Methyldopa | PO | 250 mg BD | First-line oral agent; centrally acting α-agonist; long safety record |
| Labetalol | PO/IV | 100 mg BD PO; 20-40 mg IV | Combined α₁/β blocker; good safety profile |
| Nifedipine | PO | 30 mg once daily (extended release) | Ca²⁺ channel blocker; effective and safe |
| Hydralazine | IV/IM | 5-10 mg IV/IM q20 min | For acute severe HTN; vasodilator |
Drugs CONTRAINDICATED in pregnancy:
- ACE inhibitors (captopril, enalapril) - cause fetal renal agenesis, oligohydramnios
- Angiotensin receptor blockers (ARBs) - same fetal toxicity
- Beta-blockers used cautiously (associated with fetal growth restriction)
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
3. Seizure Prophylaxis & Treatment - Magnesium Sulfate
Magnesium sulfate is the cornerstone for seizure prevention and treatment in preeclampsia/eclampsia:
Why MgSO₄?
- Most effective anticonvulsant in this setting
- Maintains uterine and fetal blood flow
- Does NOT significantly lower BP
- Wide margin of safety with monitoring
Parkland Protocol:
- Loading dose: 4-6 g IV over 15-20 minutes
- Maintenance: 2 g/hr IV infusion
Monitoring for toxicity:
| Serum Mg Level | Effect |
|---|---|
| 4-7 mEq/L | Therapeutic (anticonvulsant) |
| ~10 mg/dL | Loss of deep tendon reflexes (first sign of toxicity) |
| ~12 mg/dL | Respiratory depression |
| >15 mg/dL | Cardiac arrest |
Clinical monitoring (when levels unavailable):
- Check patellar reflexes before each dose
- Monitor respiratory rate and urine output (≥25 mL/hr)
Antidote for hypermagnesemia: Calcium gluconate 1 g IV (given slowly)
4. If Seizures Persist Despite MgSO₄
Second-line anticonvulsants (with obstetric consultation):
- Lorazepam 2-4 mg IV (may repeat ×1 after 10-15 min)
- Phenytoin/Fosphenytoin 15-20 mg/kg IV
- Levetiracetam 20-60 mg/kg IV
Always exclude other causes: hypoglycemia, intracranial hemorrhage, drug toxicity
(Rosen's Emergency Medicine)
5. Delivery - Definitive Management
| Gestational Age | Management |
|---|---|
| ≥37 weeks | Deliver promptly |
| 34-37 weeks with severe features | Deliver after stabilization |
| <34 weeks without severe features | Expectant management, steroids for fetal lung maturity, hospitalize |
| <34 weeks with severe features | Delivery is usually indicated after initial stabilization |
- Betamethasone or dexamethasone given for fetal lung maturation if <34 weeks
- Consider antibiotics if infection risk present
6. Postpartum Considerations
- ~20% of eclamptic seizures occur >48 hours postpartum
- Continue MgSO₄ for 24-48 hours postpartum in severe cases
- Proteinuria and hypertension typically resolve within 1-2 weeks after delivery
- Long-term: women with PIH have elevated lifetime risk of cardiovascular disease, chronic hypertension, and stroke
Morphological/Pathological Changes
(Robbins & Kumar Basic Pathology)
Placental changes:
- Multiple placental infarcts (far more extensive than in normal pregnancy)
- Retroplacental hemorrhage
- Ischemic villi changes: increased syncytial epithelial knots
- Acute atherosis of decidual vessels - fibrinoid necrosis with lipid-laden macrophage accumulation
Renal changes:
- Glomerular endotheliosis - swollen endothelial cells, protein deposits in basement membranes
- Reduced GFR (opposite to the increased GFR of normal pregnancy)
Summary
| Aspect | Key Point |
|---|---|
| Core mechanism | Failed spiral artery remodeling → placental ischemia → endothelial dysfunction |
| Diagnosis triggers | BP ≥140/90 after 20 wks + proteinuria or end-organ damage |
| Severe BP threshold | ≥160/110 mmHg |
| Anticonvulsant of choice | Magnesium sulfate (not antihypertensive effect, but best seizure prevention) |
| First-line antihypertensives | Methyldopa, Labetalol, Nifedipine |
| Contraindicated drugs | ACEi, ARBs |
| Definitive treatment | Delivery |
| HELLP components | Hemolysis + Elevated LFTs + Low Platelets |
| Post-delivery prognosis | Usually resolves in 1-2 weeks; long-term CV risk elevated |
Sources:
- Rosen's Emergency Medicine, 9th Ed. - Ch. 173
- Robbins & Kumar Basic Pathology - Ch. 7
- Guyton and Hall Textbook of Medical Physiology
- Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed.
- Creasy & Resnik's Maternal-Fetal Medicine, 8th Ed. - Ch. 45
This is a shared conversation. Sign in to Orris to start your own chat.