Recent advances in management of rotator cuff tear ms ortho 20 marks answer
Reading File
Finding Sources
Searching PubMed
"rotator cuff tear"[MeSH Terms] AND management
Searching the Web
recent advances management rotator cuff tear 2024 2025 surgical repair biologic augmentation
Reading File
Reading File
Searching PubMed
"rotator cuff" AND repair AND outcomes
Reading File
Reading File
Reading Web Page
https://orthospinenews.com/2025/08/28/aaos-updates-clinical-…
Reading File
Reading File
Loading Image
I now have all the material needed to write a comprehensive MS Ortho 20-mark exam answer. Here it is:
Recent Advances in Management of Rotator Cuff Tear
(MS Orthopaedics - 20 Marks Answer)
Introduction
The rotator cuff is formed by four muscles - supraspinatus, infraspinatus, teres minor, and subscapularis. Rotator cuff tears (RCT) represent a continuum from mild impingement through partial tear, full-thickness tear, massive tear, to rotator cuff tear arthropathy. Management has undergone a remarkable evolution over the past two decades, with advances spanning diagnostics, surgical technique, biologic augmentation, rehabilitation protocols, and implant technology.
Classification (DeOrio & Cofield)
| Category | Size |
|---|---|
| Small | < 1 cm |
| Medium | 1 - 3 cm |
| Large | 3 - 5 cm |
| Massive | > 5 cm (two or more tendons) |
Bursal-side tears carry a worse prognosis than articular-side tears (mnemonic: "Bursa is Bad"). Tears typically begin at the anterolateral supraspinatus and progress posteriorly to involve the infraspinatus and teres minor.
I. ADVANCES IN DIAGNOSIS
1. MRI
MRI remains the gold standard, providing information on:
- Extent and pattern of tear (crescent, U-shape, L-shape, massive contracted)
- Degree of retraction
- Muscular atrophy and fatty infiltration (Goutallier classification)
- Tangent sign - failure of the supraspinatus muscle belly to cross a line from the superior coracoid to the superior scapular spine; predicts irreparability
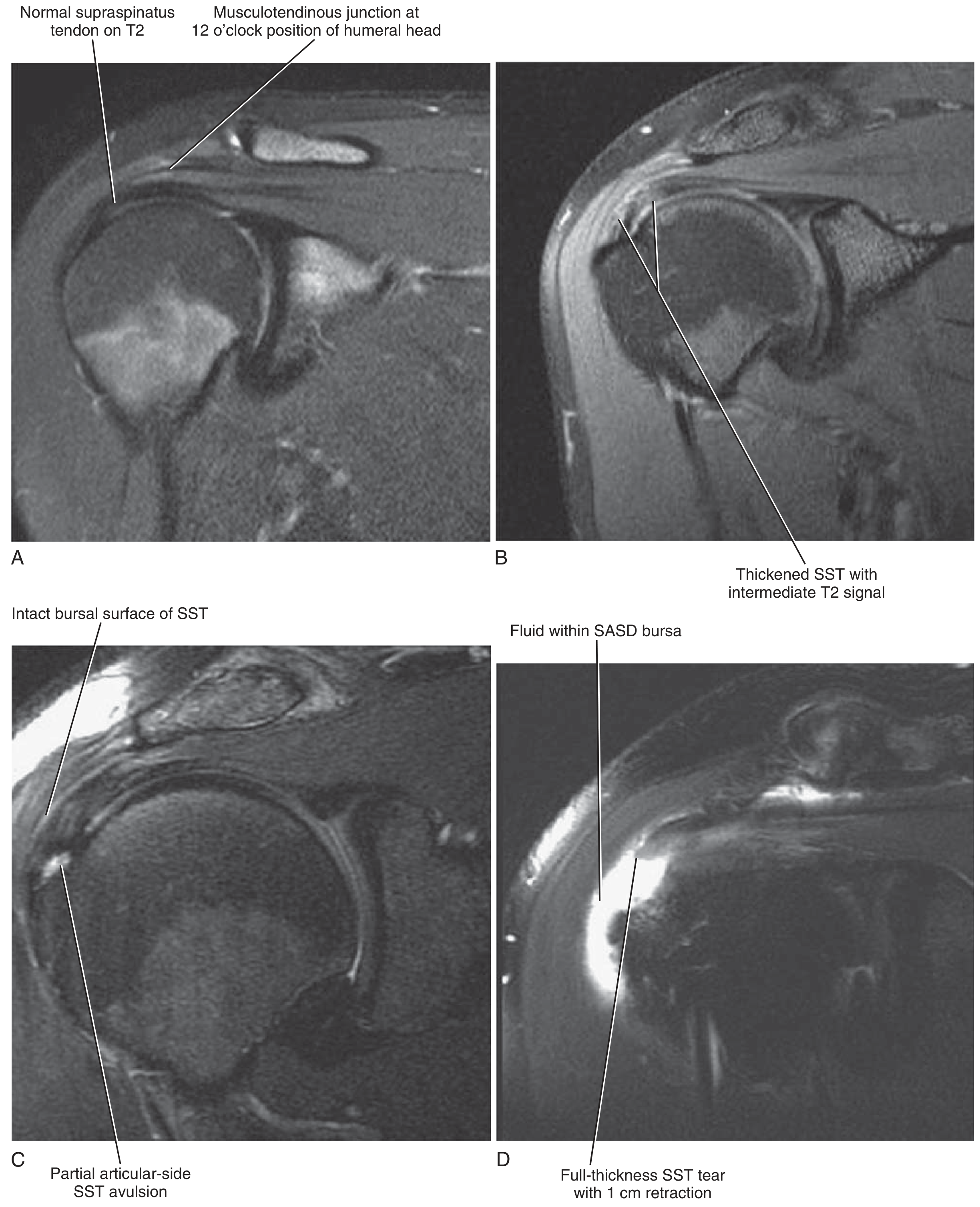
MRI appearances of rotator cuff tears - Miller's Review of Orthopaedics, 9th Ed., p. 392
2. Ultrasound
- Increasingly popular for diagnosis and real-time guided injections
- Dynamic assessment of tendon during movement is a unique advantage over MRI
- Cost-effective; no radiation; sensitivity for full-thickness tears approaches MRI
3. AI-Assisted Imaging (Emerging)
- Machine learning algorithms applied to CT and MRI now allow automated, accurate classification of tear size, fatty infiltration grade, and prediction of repair failure risk - an area of active research (Familiari et al., 2022)
II. NON-OPERATIVE MANAGEMENT
Indications
- Asymptomatic full-thickness tears
- Elderly patients (> 65 years) with low functional demands
- Medical contraindications to surgery
- Rotator cuff tear arthropathy
Protocol (3-Phase Rehabilitation)
Phase I - Pain relief, restore motion
- Pendulum exercises, passive wand-assisted flexion, overhead pulley, posterior capsular stretching
- NSAIDs, ice/heat modalities
Phase II - Strengthening
- Elastic resistance band exercises out of the impingement arc (70-120° flexion)
- Scapular stabilizers: trapezius, serratus anterior
- Deltoid and remaining cuff strengthening
Phase III - Return to activity / sports-specific rehabilitation
Steroid Injections - Updated Evidence (AAOS 2025)
- Previously, multiple cortisone injections were common practice
- The 2025 AAOS CPG now recommends a maximum of one corticosteroid injection, especially in patients considering surgery - to optimize healing potential and minimize surgical site infection risk
- Injection into the cuff tendon itself must be avoided
III. ADVANCES IN SURGICAL TECHNIQUE
A. Evolution of Approach
| Era | Technique |
|---|---|
| 1970s-1990s | Open repair (large deltoid-splitting incision) |
| 1990s-2000s | Mini-open / deltoid-sparing approach |
| 2000s-present | All-arthroscopic repair (gold standard) |
The all-arthroscopic technique offers less blood loss, faster recovery, reduced deltoid morbidity, and equivalent or superior clinical outcomes compared to open repair.
B. Repair Configurations
Single-Row Repair
- Single line of anchors at the medial aspect of the footprint
- Simpler, faster
Double-Row Repair
- Medial row anchors + lateral row anchors
- Restores the original footprint anatomy more faithfully
- Greater contact area and compression at the tendon-bone interface
Suture-Bridge / Transosseous-Equivalent (TOE) Technique
- Current state-of-the-art configuration
- Medial row anchors + lateral row knotless anchors with sutures crossing over the tendon like a bridge
- Creates a watertight seal over the footprint
- Biomechanically superior in vitro; meta-analyses show improved structural healing rates over single-row, though functional outcome differences remain debated
- (Miller's Review of Orthopaedics, 9th Ed., p. 393)
C. Acromioplasty - No Longer Routine
- Routine acromioplasty is no longer recommended during rotator cuff repair, based on current evidence showing no additional benefit
D. Anchor Technology
- Evolution from metallic to bioabsorbable to all-suture anchors
- All-suture anchors (e.g., ICONIX, JuggerKnot) offer smaller profiles, preserve bone stock, and are particularly useful in osteoporotic bone
IV. MANAGEMENT OF SPECIAL SITUATIONS
A. Partial-Thickness Tears (PASTA lesion)
- Articular-side partial tears with >50% thickness involvement (>7 mm lateral bone exposed): proceed to repair
- < 50% thickness: debridement + subacromial decompression
- Factors considered: tear depth, pattern, footprint uncoverage, patient activity level
B. Large and Massive Tears
- Higher failure rates; tissue quality is the rate-limiting factor
- Interval slides (coracohumeral ligament release, interval slide medially and posteriorly) allow tendon mobilization
- Margin convergence technique (side-to-side suturing the free edges of U- or L-shaped tears) reduces tension on the repair
C. Irreparable Massive Tears - Major Advances
This is the area with the greatest recent innovation:
1. Debridement + Biceps Tenotomy/Tenodesis
- Useful when pain is the primary complaint with preserved motion
- Biceps tenotomy reliably reduces subacromial pain
2. Latissimus Dorsi Tendon Transfer
- Indicated for combined supraspinatus + infraspinatus irreparable tears in patients younger than 65 years without glenohumeral arthritis
- Restores external rotation and abduction
3. Superior Capsular Reconstruction (SCR) - Recent Advance
- Pioneered by Mihata (Japan, 2013)
- Uses fascia lata autograft (preferred) or dermal allograft
- Reconstructs the superior capsule, restoring the superior restraint mechanism and preventing proximal humeral migration
- Indications: massive irreparable tears with pseudoparalysis, acromiohumeral distance < 7 mm
- Clinical enthusiasm has grown significantly; rigorous long-term outcome studies continue
- (Miller's Review of Orthopaedics, 9th Ed., p. 393)
4. Balloon Spacer (InSpace Balloon)
- Biodegradable subacromial balloon implant
- Creates a mechanical spacer preventing superior humeral head migration
- Indicated in elderly, low-demand patients with massive irreparable tears
- Provides pain relief without the complexity of tendon transfer surgery
5. Reverse Total Shoulder Arthroplasty (RTSA)
- Traditional indication: massive irreparable RCT + glenohumeral arthritis + pseudoparalysis
- Expanding indication (controversial): RTSA now increasingly used for massive irreparable tears even WITHOUT arthritis
- Produces reliable pain relief and functional improvement in elderly patients
- (Miller's Review of Orthopaedics, 9th Ed., p. 393)
V. BIOLOGIC AUGMENTATION - THE FRONTIER
The 2025 AAOS Clinical Practice Guideline explicitly identifies biologics as the newest frontier in rotator cuff management, noting that despite advances in technique, achieving consistent healing in certain tears remains a challenge.
A. Platelet-Rich Plasma (PRP)
- Concentrated autologous growth factors: PDGF, TGF-β, VEGF, EGF
- Meta-analyses of RCTs (Shen et al., 2024) show PRP augmentation at the tendon-bone interface reduces retear rates and improves clinical outcomes after arthroscopic repair
- Leukocyte-poor PRP (LP-PRP) may be superior to leukocyte-rich PRP (LR-PRP) for tendon healing (Tang et al., 2024)
- Application methods: subacromial injection, gel application at repair site, fibrin matrix
B. Bioinductive Collagen Implants (REGENETEN - Smith+Nephew)
- Strong recommendation in the 2025 AAOS CPG
- A bovine-derived type I collagen scaffold placed on the bursal surface of the repaired tendon
- Induces new host tendon tissue formation ("bioinduction")
- Systematic review (Warren et al., J Shoulder Elbow Surg, 2024 - PMID 38942225) confirms reduced retear rates and improved patient-reported outcomes
- Systematic review by Benthami Kbibi et al. (Acta Orthop Belg, 2024 - PMID 39869884) further validates clinical efficacy
- Particularly effective for partial-thickness and large full-thickness tears
C. Mesenchymal Stem Cells (MSCs)
- Applied at the tendon-bone junction to promote regeneration
- Early clinical evidence is promising; standardized protocols not yet established
- Subacromial bursal cells identified as a rich autologous MSC source (Morikawa et al., 2019)
D. Scaffolds and Patches
- Dermal allografts (GraftJacket): augment repair in massive tears
- Decellularized amniotic membrane: shown to improve tendon-bone integration in animal models (Wang et al., 2025)
- Xenograft patches: NOT recommended - not found to be helpful
- EnFix (Tetrous) DBF implant: novel decellularized bone-fibrocartilage implant showing superior Sugaya scale outcomes in augmented vs. non-augmented massive tear repair (2024 SESA meeting data)
VI. POSTOPERATIVE REHABILITATION - UPDATED EVIDENCE
Immobilization vs. Early Mobilization
The 2025 AAOS CPG provides high-level evidence that for small-to-medium full-thickness tears repaired arthroscopically:
- Early mobilization and delayed mobilization (up to 8 weeks) yield similar clinical and patient-reported outcomes
- Sling use guidance: early sling mobilization is safe and does not increase retear risk
Meta-analyses (Hu et al., BMC Musculoskelet Disord, 2023 - PMID 38049792; Hao et al., BMC Musculoskelet Disord, 2025 - PMID 40082920) confirm no significant difference in functional recovery between early exercise and immobilization protocols for small-medium tears.
Clinical implication: Surgeons now trend toward earlier mobilization to prevent stiffness, particularly in smaller tears, without compromising structural outcomes.
VII. PREDICTORS OF OUTCOME & FAILURE
- Age: younger patients have better structural healing; correlation between age and repair success is strong
- Tear size: larger, more retracted tears (> 40 mm) have higher failure rates
- Fatty infiltration: Goutallier grade ≥ 3 predicts poor healing
- Tangent sign positive: correlates with irreparability
- Acromiohumeral distance < 7 mm: suggests irreparable tear
- Obesity: worsens postoperative outcomes (Ma et al., PLoS One, 2024 - PMID 38478532)
- Steroid injection within 6 months of surgery: increases failure rate
- Failure is most common in the first 3 to 6 months; tissue pull-through of sutures is the typical mechanism
- Despite structural failure, most patients report subjective improvement following repair
VIII. OPERATIVE vs. NON-OPERATIVE (AAOS 2025)
The 2025 AAOS CPG states: moderate evidence suggests that surgery to repair a torn rotator cuff yields improved patient-reported and functional outcomes compared to non-operative management, specifically in patients whose repairs heal. Healed repairs lead to significantly better outcomes than unhealed repairs or physical therapy alone.
IX. EMERGING TECHNOLOGIES
| Technology | Status |
|---|---|
| AI-driven diagnosis & outcome prediction | Early clinical use |
| Extracellular vesicle therapy (exosomes) | Preclinical / early trials |
| Gene therapy for tendon healing | Experimental |
| 3D-printed bioscaffolds | Experimental |
| Robotic-assisted arthroscopy | Emerging |
Summary Table - Recent Advances at a Glance
| Domain | Advance |
|---|---|
| Diagnosis | Tangent sign for irreparability; AI-assisted MRI analysis |
| Surgical approach | All-arthroscopic TOE/suture-bridge repair as standard |
| Partial tear | PASTA repair for > 50% thickness |
| Massive/irreparable tear | SCR, balloon spacer, RTSA expansion |
| Biological healing | PRP, bioinductive collagen implants (strong AAOS 2025 rec.) |
| Scaffolds | Dermal allograft, decellularized amniotic membrane, EnFix |
| Rehab | Early mobilization safe for small-medium tears (AAOS 2025) |
| Steroids | Only one pre-op injection recommended (AAOS 2025) |
| Arthroplasty | RTSA expanding to non-arthritic massive irreparable tears |
Conclusion
Management of rotator cuff tears has moved from simple open debridement to a highly individualized, biology-driven, arthroscopic paradigm. The greatest recent shift is the recognition that anatomical repair alone is insufficient in certain tears - the future lies in biologic augmentation (PRP, bioinductive implants, stem cells, smart scaffolds) combined with precise patient selection and optimized rehabilitation. The 2025 AAOS guidelines formalize many of these advances into evidence-based recommendations, marking a new era in rotator cuff surgery.
Key References:
- Miller's Review of Orthopaedics, 9th Edition
- Firestein & Kelley's Textbook of Rheumatology
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- AAOS Clinical Practice Guideline: Management of Rotator Cuff Injuries, 2025
- Warren JR et al. Bioinductive patch meta-analysis. J Shoulder Elbow Surg 2024 [PMID 38942225]
- Hu CW et al. Early vs. delayed mobilization meta-analysis. BMC Musculoskelet Disord 2023 [PMID 38049792]
- Ma X et al. Obesity and RCR outcomes. PLoS One 2024 [PMID 38478532]
- Hao B et al. Early exercise after arthroscopic RCR. BMC Musculoskelet Disord 2025 [PMID 40082920]
- Lee KS et al. Current concepts in arthroscopic RCR. Clin Shoulder Elbow 2025
Recent advances in management of rotator cuff tear ms ortho 20 marks answer
Reading File
Finding Sources
Searching PubMed
"rotator cuff" AND repair AND biologics
Searching the Web
AAOS 2025 rotator cuff guidelines bioinductive implant PRP superior capsular reconstruction advances
Reading File
Reading File
Reading Web Page
https://www.aaos.org/rccpg2025
Loading Image
Reading File
Searching PubMed
"rotator cuff" AND "superior capsular reconstruction" OR "reverse shoulder arthroplasty"
I now have comprehensive, up-to-date material from Miller's Orthopaedics, Firestein Rheumatology, the AAOS 2025 CPG, and recent PubMed evidence. Here is the full MS Ortho 20-marks answer:
Recent Advances in Management of Rotator Cuff Tear
MS Orthopaedics - 20 Marks
Introduction
The rotator cuff comprises four muscles - supraspinatus, infraspinatus, teres minor, and subscapularis - that together provide dynamic stability and power to the glenohumeral joint. Rotator cuff tears (RCT) represent a disease continuum from mild impingement through partial tear, full-thickness tear, and massive tear, to rotator cuff tear arthropathy. Management has undergone a remarkable transformation, driven by advances in surgical technique, implant design, biologic science, diagnostic imaging, and evidence-based rehabilitation. The landmark AAOS 2025 Clinical Practice Guideline (published August 2025) now formally incorporates many of these advances.
Classification
DeOrio & Cofield Classification (by size):
| Grade | Size |
|---|---|
| Small | < 1 cm |
| Medium | 1 - 3 cm |
| Large | 3 - 5 cm |
| Massive | > 5 cm or two or more tendons |
Classification does not directly predict prognosis. Tears typically begin at the anterolateral supraspinatus and progress posteriorly. Bursal-side tears carry a worse prognosis than articular-side tears (mnemonic: "Bursa is Bad").
I. ADVANCES IN DIAGNOSIS
1. MRI - Gold Standard
MRI defines the extent of tear, retraction, muscular atrophy, and fatty infiltration (Goutallier classification, Grade 0-4). Key recent MRI parameters:
- Tangent sign: Failure of the supraspinatus muscle belly to cross a line from the superior coracoid to the superior scapular spine - correlates with muscular atrophy and fatty infiltration, and predicts irreparability
- Acromiohumeral distance < 7 mm on AP radiograph: further predictor of irreparable tear
- Larger, more retracted tears (> 40 mm) with supraspinatus width < 5 mm at glenoid margin and high infraspinatus signal indicate poor repairability
2. Ultrasound
- Increasing popularity for diagnosis AND for guiding injections
- Dynamic imaging during movement is a unique advantage over MRI
- Cost-effective, no radiation; sensitivity for full-thickness tears approaches MRI
- Allows real-time guided PRP injection - directly applicable to newer biologic therapies
3. AI-Assisted Imaging (Emerging)
Machine learning algorithms applied to CT and MRI allow automated classification of tear size, fatty infiltration grading, and prediction of surgical failure risk - an area of rapidly expanding research (Familiari et al., IJERPH 2022). AI tools are being developed to optimize patient selection for repair vs. conservative management.
II. NON-OPERATIVE MANAGEMENT
Indications
- Asymptomatic full-thickness tears
- Elderly (> 65 years), low-demand patients
- Medical contraindications to surgery
- Rotator cuff tear arthropathy
- Athletes with articular-side partial tears and instability component
Three-Phase Rehabilitation (Mainstay)
Phase I - Pain relief and motion restoration:
- Pendulum exercises, passive wand-assisted flexion, overhead pulley, posterior capsular stretching
- NSAIDs, ice post-activity, heat before stretching
- Deep massage to periscapular trigger points
Phase II - Strengthening:
- Elastic resistance band exercises outside the impingement arc (70-120° flexion)
- Strengthen deltoid, remaining cuff muscles, scapular stabilizers (trapezius, serratus anterior)
- Goal: prevent dynamic proximal humeral migration
Phase III - Return to activity / work / sport-specific training
Non-operative response rates range from 33% to 90% in the literature (Firestein & Kelley, p. 892). Full-thickness tears can remain functional - 90% of patients in some series responded to conservative measures.
Updated Steroid Injection Policy (AAOS 2025)
Previously, multiple sequential cortisone injections were routine. The 2025 AAOS CPG now recommends a maximum of one corticosteroid injection, particularly in patients considering surgery, to optimize healing potential and minimize surgical site infection risk. Injection frequency should not exceed once every 3 months, and injection directly into the cuff tendon must be avoided.
III. ADVANCES IN SURGICAL TECHNIQUE
A. Evolution of Surgical Approach
| Era | Technique |
|---|---|
| 1970s-1990s | Classic open repair (deltoid-splitting) |
| 1990s-2000s | Mini-open / deltoid-sparing approach |
| 2000s-present | All-arthroscopic repair - current gold standard |
Arthroscopic repair offers reduced blood loss, less deltoid morbidity, faster recovery, and equivalent or superior outcomes. The rate-limiting step remains biologic healing of tendon to bone, requiring a minimum of 8-12 weeks regardless of technique (Miller's Review of Orthopaedics, p. 393).
B. Repair Configurations - The Suture-Bridge Evolution
Single-Row Repair:
- One line of anchors medially at the footprint
- Simpler and faster; adequate for small tears
Double-Row Repair:
- Medial row + lateral row anchors
- Restores original footprint anatomy more faithfully
- Greater contact area and compression at tendon-bone interface
- Meta-analyses: lower retear rates vs. single-row in large tears
Suture-Bridge / Transosseous-Equivalent (TOE) Technique - Current Standard:
- Medial row anchors with limbs crossed over the tendon and fixed laterally with knotless anchors
- Creates a watertight seal over the entire footprint
- Maximizes footprint contact, compresses vascularity into tendon
- Biomechanically superior in vitro; clinical outcome differences vs. double-row continue to be studied
- This is the current technique of choice for medium to large tears
C. Acromioplasty - No Longer Routine
Routine subacromial acromioplasty is no longer recommended as part of rotator cuff repair, based on current evidence showing no added clinical benefit (Miller's Review of Orthopaedics, p. 393; AAOS 2025 CPG).
D. Anchor Technology Advances
| Generation | Material | Feature |
|---|---|---|
| 1st | Metal (titanium/stainless) | Strong, artifact on MRI |
| 2nd | Bioabsorbable polymer | Dissolves over time |
| 3rd | All-suture anchors | Smallest profile, preserves bone stock |
All-suture anchors (e.g., ICONIX, JuggerKnot, Y-Knot) are now preferred - ideal in osteoporotic bone and revision cases as they leave no debris if they fail.
E. Open vs. Arthroscopic - AAOS 2025 Guidance
The 2025 AAOS CPG addresses this explicitly. Evidence supports arthroscopic approach for equivalent outcomes with less morbidity. Open repair remains an option for complex reconstructions (tendon transfers).
IV. MANAGEMENT OF SPECIAL SITUATIONS
A. Partial-Thickness Tears (PASTA Lesion)
- Articular-side partial tears involving > 50% tendon thickness (> 7 mm lateral bone exposed): recommend surgical repair
- < 50% thickness: debridement + subacromial decompression
- AAOS 2025 CPG addresses high-grade partial tears specifically; surgical repair is supported for high-grade (> 50%) lesions
- Factors to consider: tear depth, avulsion vs. degeneration pattern, footprint uncoverage, patient activity level
B. Large and Massive Tears
- Interval slides: coracohumeral ligament release ± interval slide posteriorly allows tendon mobilization to reduce repair tension
- Margin convergence (side-to-side suturing of U- or L-shaped tear free edges): reduces tension on the repair before anchoring to bone - key advance in managing complex tear patterns
- Despite higher failure rates, most patients report functional improvement following repair
V. MANAGEMENT OF IRREPARABLE MASSIVE TEARS - MAJOR ADVANCES
This is the domain of the greatest recent innovation. An irreparable tear is suggested when acromiohumeral distance is < 7 mm, tangent sign is positive, and fatty infiltration is Goutallier grade ≥ 3.
1. Debridement + Biceps Tenotomy/Tenodesis
- When pain is the primary complaint and motion is preserved
- Biceps tenotomy/tenodesis reliably reduces subacromial pain and reduces bicipital groove irritation
- AAOS 2025: consensus opinion supports this as an option for unrepairable tears without arthropathy
2. Latissimus Dorsi Tendon Transfer
- For combined supraspinatus + infraspinatus irreparable tears
- Best in patients < 65 years without glenohumeral arthritis
- Transfers latissimus to the greater tuberosity, restoring external rotation and abduction
- Established procedure with good medium-term outcomes
3. Superior Capsular Reconstruction (SCR) - Major Recent Advance
- Pioneered by Mihata (Japan) in 2013, now adopted worldwide
- Technique: A fascia lata autograft (preferred) or dermal allograft is fixed at the superior glenoid rim and the greater tuberosity, reconstructing the superior capsule
- Mechanism: Restores superior glenohumeral restraint, reduces superior humeral head migration, de-loads the remaining cuff
- Indications: Massive irreparable tears, pseudoparalysis, failure of prior repair, acromiohumeral distance < 7 mm
- Graft thickness matters: > 8 mm thick grafts have superior outcomes
- AAOS 2025 consensus: SCR is a valid option for unrepairable tears without arthropathy (along with partial repair, tendon transfer, balloon spacer, graft interposition)
- Systematic reviews and the SCR narrative review (Orthopedic Reviews, 2024) confirm good functional outcomes; ongoing research explores 3D bioprinted grafts as future direction
4. Subacromial Balloon Spacer (InSpace)
- A biodegradable balloon implant placed in the subacromial space
- Acts as a mechanical spacer, centering the humeral head, offloading the remaining cuff
- Gradually absorbed over 12 months
- Best for elderly, low-demand patients with massive irreparable tears who are not suitable for major reconstruction
- AAOS 2025 consensus: a valid option for unrepairable tears without arthropathy
- Avoids the morbidity of tendon transfer or arthroplasty
5. Reverse Total Shoulder Arthroplasty (RTSA) - Expanding Indication
- Traditional indication: massive irreparable RCT + glenohumeral arthritis + pseudoparalysis (rotator cuff tear arthropathy)
- Recent advance / controversy: RTSA is increasingly used for massive irreparable tears even without arthritis - the AAOS 2025 CPG addresses this
- RTSA works by medialization and distal shift of the center of rotation, enabling the deltoid to function as the primary abductor
- A 2025 systematic review and meta-analysis (Kelly JJ et al., Sports Med Arthrosc Rev, PMID 40424170) compares bridging reconstruction vs. RTSA for massive irreparable tears
- Reliable pain relief and functional improvement in elderly patients
- Concerns: High revision rate in younger patients; indication in non-arthritic tears remains controversial but expanding
VI. BIOLOGIC AUGMENTATION - THE FRONTLINE OF RECENT ADVANCES
Biologics represent the most rapidly evolving domain. The 2025 AAOS CPG explicitly identifies biologic augmentation as the key frontier, noting that despite refined surgical technique, consistent healing in certain tears remains challenging.
A. Platelet-Rich Plasma (PRP)
- Concentrated autologous growth factors: PDGF, TGF-β, VEGF, IGF-1, EGF
- Mechanisms: promotes cell proliferation, angiogenesis, collagen synthesis at tendon-bone interface
- Meta-analyses confirm PRP combined with arthroscopic repair reduces retear rates and improves patient-reported outcomes (Shen et al., Medicine, 2024)
- Leukocyte-poor PRP (LP-PRP) may be superior to leukocyte-rich (LR-PRP) for tendon healing - umbrella review of meta-analyses (Tang et al., J Orthop Traumatol, 2024)
- AAOS 2025 CPG: addresses PRP for both partial and full-thickness tears, emphasizes the need for standardized preparation protocols
- Application methods: subacromial injection, gel application at repair site, fibrin matrix incorporating the PRP
B. Bioinductive Collagen Implants - STRONG AAOS 2025 RECOMMENDATION
- REGENETEN (Smith+Nephew) and BioBrace (CONMED) are FDA-cleared bioinductive implants
- Bovine-derived Type I collagen scaffold placed on the bursal surface of the repaired cuff
- Mechanism: induces host tissue to grow new tendon-like tissue (bioinduction) - distinct from mechanical augmentation
- AAOS 2025 Strong Recommendation (4 out of 4 stars): "The use of bioinductive tendon implants to augment rotator cuff repair or as an alternative to non-augmented repair can lead to lower retear rates and better patient-reported outcomes"
- Evidence base:
- Ruiz Iban et al. (RCT, Arthroscopy 2024): 124 patients, medium-large tears - bioinductive group had significantly lower retear rate (8.3% vs. 25.8%, p=0.01) and better tendon integrity at 1 year
- Camacho Chacon et al. (RCT, J Shoulder Elbow Surg 2024): 60 patients, smaller tears with intact rotator cable - bioinductive repair alone vs. standard repair - better functional outcomes, lower retear rate, higher quality tendon on biopsy, faster return to work
- Systematic review (Warren JR et al., J Shoulder Elbow Surg, Nov 2024, PMID 38942225): meta-analysis confirms bioinductive patch reduces retear and improves outcomes
- Systematic review (Benthami Kbibi et al., Acta Orthop Belg, Dec 2024, PMID 39869884): further validates REGENETEN clinical efficacy
C. Mesenchymal Stem Cells (MSCs)
- Applied at the tendon-bone junction to promote regeneration
- Sources: bone marrow, adipose tissue, synovium, subacromial bursa (bursal cells identified as a rich autologous MSC source - Morikawa et al., 2019)
- Early clinical evidence promising; no internationally standardized protocol yet established
- Current reviews (Uyeki et al., Orthopedics, Nov-Dec 2024, PMID 39495158; Tagliero et al., JSES Rev Rep Tech, Feb 2026, PMID 41477010): confirm MSCs as a promising future augmentation strategy
D. Scaffolds
| Type | Example | Status |
|---|---|---|
| Dermal allograft | GraftJacket (Wright Medical) | Used clinically for massive tears |
| Decellularized amniotic membrane | Various | Animal models show improved tendon-bone integration |
| Synthetic scaffold | LARS, X-Repair | Clinical use |
| Xenograft patch | Porcine-derived | NOT recommended (AAOS 2025) |
| DBF implant | EnFix (Tetrous) | Promising early clinical data (2024 SESA) |
The AAOS 2025 consensus opinion for unrepairable tears permits "graft augmentation (non-porcine)" as a valid option. Porcine xenografts are explicitly excluded.
E. Bone Marrow Stimulation
The AAOS 2025 CPG specifically addresses marrow stimulation at the footprint during repair. Evidence suggests microfracture/needle fenestration of the greater tuberosity at the time of repair may enhance biologic healing by releasing local growth factors. Results are mixed; further studies needed.
VII. POSTOPERATIVE REHABILITATION - UPDATED EVIDENCE (AAOS 2025)
Immobilization vs. Early Mobilization
The 2025 AAOS CPG provides HIGH-level evidence (strongest recommendation level):
For small-to-medium full-thickness rotator cuff tears repaired arthroscopically, early mobilization (wearing a sling) and delayed mobilization (up to 8 weeks) yield similar clinical and patient-reported outcomes.
This is a paradigm shift from the traditional rigid 6-8 week sling immobilization protocols.
Supporting meta-analyses:
- Hu CW et al. (BMC Musculoskelet Disord, 2023, PMID 38049792): early vs. delayed mobilization meta-analysis of RCTs
- Hao B et al. (BMC Musculoskelet Disord, 2025, PMID 40082920): systematic review and meta-analysis of early exercise vs. immobilization post arthroscopic repair - similar functional recovery
Practical implication: Surgeons now trend toward earlier mobilization to prevent stiffness, especially for smaller tears, without compromising structural integrity.
Supervised vs. Unsupervised Rehabilitation
AAOS 2025 CPG also addresses supervised vs. unsupervised exercise post-repair. Evidence supports supervised rehabilitation for better outcomes, though the appropriate duration and intensity require further definition.
VIII. PREDICTORS OF OUTCOME AND FAILURE
| Factor | Effect |
|---|---|
| Younger age | Better structural healing |
| Tear size > 40 mm / massive | Higher failure rate |
| Fatty infiltration Goutallier ≥ 3 | Predicts poor healing |
| Tangent sign positive | Likely irreparable |
| Acromiohumeral distance < 7 mm | Suggests irreparable |
| Obesity | Worse postoperative outcomes (Ma et al., PLoS One 2024, PMID 38478532) |
| Steroid injection within 6 months of surgery | Increases failure rate |
| Healed repair | Significantly better outcomes than unhealed |
Most failures occur within the first 3 to 6 months - tissue pull-through of sutures is the typical mechanism. Despite structural failure, most patients still report subjective functional improvement.
IX. OPERATIVE vs. NON-OPERATIVE - AAOS 2025 GUIDANCE
The 2025 AAOS CPG states: moderate evidence supports that surgery for a torn rotator cuff yields improved patient-reported and functional outcomes compared to non-operative management, specifically when repairs heal. Healed repairs produce significantly better outcomes than physical therapy alone or failed repairs.
X. EMERGING TECHNOLOGIES
| Technology | Current Status |
|---|---|
| AI-driven imaging diagnosis and outcome prediction | Early clinical use |
| Extracellular vesicle/exosome therapy | Preclinical; SPRI $1M grant awarded 2025 |
| Gene therapy (TGF-β, BMP delivery) | Experimental |
| 3D bioprinted grafts (SCR) | Research phase |
| Robotic-assisted arthroscopy | Emerging |
Summary - Recent Advances at a Glance
| Domain | Advance |
|---|---|
| Diagnosis | Tangent sign, AI-assisted MRI interpretation |
| Surgical approach | All-arthroscopic TOE/suture-bridge repair |
| Partial tear | Repair if > 50% thickness (PASTA) |
| Massive/irreparable | SCR (fascia lata), balloon spacer, RTSA expansion |
| Biologic healing | Bioinductive implants (AAOS 2025 Strong rec.), PRP, MSCs |
| Scaffolds | Dermal allograft, decellularized amniotic membrane |
| Rehabilitation | Early mobilization safe for small-medium tears (AAOS 2025) |
| Injections | Max one pre-op steroid injection (AAOS 2025) |
| Acromioplasty | No longer routine |
Conclusion
The management of rotator cuff tears has evolved from simple open debridement to a precisely individualized, biology-driven, arthroscopic paradigm. The most important recent shift is the recognition that anatomical repair alone is insufficient in tears with poor tissue quality - the future lies in biologic augmentation (PRP, bioinductive collagen implants, stem cells, smart scaffolds), now formally endorsed by the 2025 AAOS guidelines. For irreparable massive tears, SCR and balloon spacers offer joint-preserving options while RTSA is expanding its role in non-arthritic cases. Rehabilitation protocols have been refined by high-quality RCT data supporting earlier mobilization without compromising healing. Together, these advances are rapidly improving outcomes and reducing retear rates for patients at all stages of rotator cuff disease.
Key References:
- Miller's Review of Orthopaedics, 9th Edition, pp. 391-394
- Firestein & Kelley's Textbook of Rheumatology, pp. 892-895
- AAOS Clinical Practice Guideline: Management of Rotator Cuff Injuries (Published August 2025) - aaos.org/rccpg2025
- Ruiz Iban MA et al. Bioinductive implant RCT. Arthroscopy 2024
- Camacho Chacon JA et al. Bioinductive vs repair alone. J Shoulder Elbow Surg 2024
- Warren JR et al. Bioinductive patch meta-analysis. J Shoulder Elbow Surg 2024 [PMID 38942225]
- Benthami Kbibi M et al. REGENETEN systematic review. Acta Orthop Belg 2024 [PMID 39869884]
- Hu CW et al. Early vs. delayed mobilization. BMC Musculoskelet Disord 2023 [PMID 38049792]
- Hao B et al. Early exercise after arthroscopic repair. BMC Musculoskelet Disord 2025 [PMID 40082920]
- Ma X et al. Obesity and rotator cuff repair outcomes. PLoS One 2024 [PMID 38478532]
- Kelly JJ et al. Bridging reconstruction vs RTSA. Sports Med Arthrosc Rev 2025 [PMID 40424170]
- Uyeki CL et al. Biologic augmentation current concepts. Orthopedics 2024 [PMID 39495158]
- Tagliero AJ et al. RCR and biologic augmentation. JSES Rev Rep Tech 2026 [PMID 41477010]
This is a shared conversation. Sign in to Orris to start your own chat.