
Answer
Reading File
Finding Sources
Searching the Web
acute epiglottitis AETCOM patient counseling intubation tracheostomy conservative management
Reading File
Reading File
Now I have comprehensive information. Here is the complete AETCOM answer for counseling a patient about Acute Epiglottitis:
AETCOM (5 marks) — Patient Counseling: Acute Epiglottitis
Context: You are explaining the diagnosis, management plan, and risks to a patient (or parent) with acute epiglottitis.
1. Necessary Conservative Management
Tell the patient/family:
- What the disease is: Acute epiglottitis is a serious infection causing swelling of the epiglottis (the flap covering the airway). It can rapidly block breathing and become life-threatening.
- Hospital admission is mandatory — this cannot be managed at home.
- Conservative treatment includes:
- Keeping the patient calm and in a comfortable sitting/upright position (leaning forward — "tripod position") to keep the airway open
- Supplemental oxygen by mask (non-threatening delivery)
- IV antibiotics (typically 3rd-generation cephalosporins to cover H. influenzae, streptococci, staphylococci)
- IV corticosteroids to reduce swelling
- IV fluids and close monitoring in an ICU or high-dependency setting
- Avoid agitating the patient — no unnecessary blood draws, IV insertions, or oral examination, as any distress can precipitate complete airway obstruction
2. Necessity of Intubation / Tracheostomy if Conservative Management Fails
- The airway can deteriorate rapidly and unpredictably — from sore throat to complete obstruction within hours.
- If breathing worsens despite antibiotics and steroids, securing the airway artificially becomes immediately necessary.
- Endotracheal intubation is the preferred method and is performed in the operating theatre under controlled general anaesthesia with surgeons on standby.
- Tracheostomy may be performed if intubation fails or is not technically possible due to severe swelling.
- In centers without expert airway personnel, tracheostomy may be the primary approach.
- The patient must consent to these procedures in advance, as there may be no time for discussion if deterioration is sudden.
3. Possibility of Worsening / Death Before, During, or After the Procedure
This is a critical part of honest, transparent informed consent:
- Acute epiglottitis carries a real risk of sudden complete airway obstruction at any point — even while appearing stable.
- Death can occur before a procedure if the airway closes before help is secured.
- During intubation/tracheostomy, there is risk of:
- Failed intubation due to massively swollen, distorted anatomy
- Laryngospasm triggered by airway manipulation in the non-anaesthetized patient
- Cardiac arrest from hypoxia
- After the procedure, risks include:
- Accidental extubation or tube displacement
- Secondary infection or subglottic stenosis
- Prolonged ICU stay
- Even with all appropriate treatment, mortality — though low in properly managed cases — exists and the family must be prepared.
Summary Points for Counseling (Mark-Scoring Format)
| Point | Detail |
|---|---|
| Nature of disease | Life-threatening swelling of airway structure |
| Conservative Rx | Antibiotics + steroids + O₂ + calm environment + monitoring |
| Indications for intubation | Worsening stridor, respiratory distress, failure of conservative Rx |
| Intubation vs tracheostomy | Intubation preferred; tracheostomy as fallback |
| Risk of death | Real risk before, during, and after any intervention — must disclose honestly |
Sources: Barash Clinical Anesthesia 9e; Tintinalli's Emergency Medicine; Acute epiglottitis: epidemiology, clinical presentation, management and outcome — Cummings Otolaryngology reference.
Symptoms
Finding Sources
Reading File
Symptoms of Acute Epiglottitis
Classic Presentation (the "4 D's + 1")
| Symptom | Detail |
|---|---|
| Dysphagia | Difficulty/pain on swallowing — often the first complaint |
| Drooling | Cannot swallow secretions; hallmark sign |
| Dysphonia | Muffled/"hot potato" voice (not hoarse like croup) |
| Dyspnoea | Difficulty breathing, especially on inspiration |
| +Distress/Toxicity | Patient looks acutely ill, anxious, pale |
Symptoms in Detail
General
- Abrupt onset — progresses within hours
- High fever (typically >38.5°C)
- Intense sore throat disproportionate to visible pharyngeal findings
Airway / Respiratory
- Inspiratory stridor (turbulent flow from supraglottic swelling)
- Laboured breathing with intercostal retractions
- Cyanosis — a late, pre-terminal sign
- Cough is usually absent (key differentiator from croup)
Posture
- Tripod / sniffing position — sitting upright, jaw jutting forward, neck extended to maximise airway opening; the child refuses to lie down
ENT / Oral
- Drooling due to inability to swallow
- Muffled, thick voice ("hot potato" speech)
- Tenderness on palpation of the anterior neck (especially in adults)
CNS
- Anxiety, agitation
- Altered mental status in severe cases (hypoxia)
Adults vs. Children
| Feature | Children | Adults |
|---|---|---|
| Onset | Sudden, dramatic | Slower, more insidious |
| Drooling | Prominent | Less obvious |
| Stridor | Common | Less prominent (larger airway) |
| Main complaint | Respiratory distress | Severe sore throat + odynophagia |
Key Differentiating Point from Croup
- No barking cough in epiglottitis
- Cough is a hallmark of croup; its absence should raise suspicion for epiglottitis
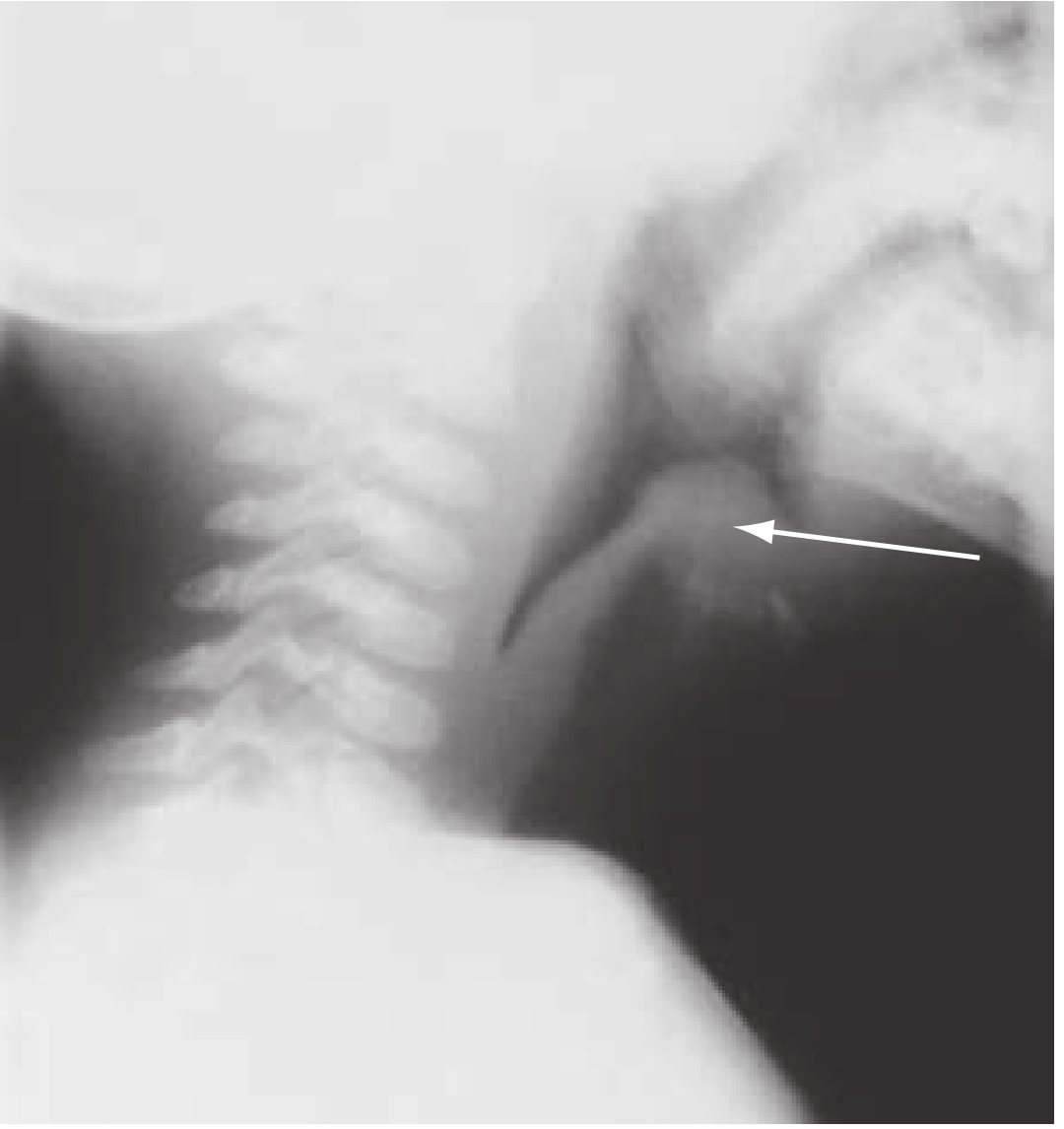
Radiological "Symptom" (Thumbprint Sign)
On lateral neck X-ray: swollen epiglottis appears as a thumb-shaped soft tissue shadow — thickened aryepiglottic folds and loss of air in the vallecula. Note that up to 70% of X-rays can be normal, so a negative film does not rule out the diagnosis.
Source: Rosen's Emergency Medicine; Barash Clinical Anesthesia; Tintinalli's Emergency Medicine
Diagnosed
Finding Sources
Reading File
Reading File
Diagnosis of Acute Epiglottitis
⚠️ Golden Rule Before Any Investigation
Do NOT examine the throat with a tongue depressor and do NOT attempt direct visualization of the epiglottis in an unanesthetized patient. This can trigger laryngospasm and cause immediate, complete airway obstruction. A qualified person with intubation equipment must be present at all times during any diagnostic procedure.
1. Clinical Diagnosis (Most Important)
Diagnosis is primarily clinical — based on history and observation:
| Feature | Finding |
|---|---|
| Posture | Tripod/sniffing position, refuses to lie flat |
| Voice | Muffled "hot potato" voice |
| Drooling | Unable to swallow secretions |
| Sore throat | Severe, out of proportion to exam findings |
| Fever | High grade |
| Cough | Absent (key differentiator from croup) |
| Age/onset | Abrupt onset, toxic-looking child |
A "sore throat + drooling + no cough + stridor" combination should immediately raise suspicion.
2. Lateral Neck X-Ray
The first-line imaging investigation.
Look for:
- Thumbprint sign — swollen epiglottis resembling a thumb on the lateral view (pathognomonic)
- Thickened aryepiglottic folds
- Loss of air in the vallecula
- Dilated hypopharynx
Limitation: Up to 70% of X-rays can be normal — a negative film does NOT rule out epiglottitis.
3. Direct Laryngoscopy (Gold Standard)
- Performed only in a controlled setting (operating theatre or ICU) with a skilled airway team ready to intubate immediately
- Visualises the cherry-red, swollen epiglottis directly
- Simultaneously allows securing the airway if obstruction occurs
4. Blood Investigations
- Full blood count (FBC): Leukocytosis (elevated WBC) with neutrophilia
- Blood cultures: Taken after airway is secured — identify causative organism
- C-reactive protein (CRP): Elevated, confirms infection
- Do NOT delay airway management for blood tests
5. Cultures
- Blood cultures and epiglottis swab (taken at time of intubation/laryngoscopy, not before)
- Guide antibiotic therapy
6. CT / MRI Neck
- Used selectively in stable adult patients or when diagnosis is uncertain
- CT can show thickened epiglottis, surrounding oedema, and rule out abscess
- Not suitable for unstable or distressed patients
Epiglottitis vs. Croup — Diagnostic Differentiator
| Feature | Epiglottitis | Croup |
|---|---|---|
| Cough | Absent | Barking cough |
| Drooling | Yes | No |
| Voice | Muffled | Hoarse |
| X-ray sign | Thumbprint sign | Steeple sign |
| Cause | Bacterial (H. influenzae, Strep) | Viral (parainfluenza) |
| Age | Older child/adult | Young infant/toddler |
| Onset | Rapid (hours) | Gradual (days) |
Sources: Rosen's Emergency Medicine; Swanson's Family Medicine Review; Tintinalli's Emergency Medicine
Examination
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.