Physiology of lactation for 1st year mbbs 5 marks qn
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, exam-ready answer. Here is the complete 5-mark answer:
Physiology of Lactation
1. Development of the Breast (Mammogenesis)
Breast development for lactation occurs in stages under hormonal control:
- Estrogens (from puberty onward) stimulate growth of the ductal system and fat deposition. During pregnancy, placental estrogens cause the ductal system to grow and branch extensively.
- Progesterone (during pregnancy) drives full development of the lobule-alveolar system - it stimulates budding of alveoli and secretory differentiation of alveolar cells.
- Supporting hormones include: growth hormone, prolactin, adrenal glucocorticoids, and insulin - all involved in protein metabolism needed for breast tissue growth.
2. Initiation of Lactation (Lactogenesis) - Role of Prolactin
Prolactin is the key lactogenic hormone, secreted by the anterior pituitary.
- During pregnancy, prolactin levels rise steadily from the 5th week to 10-20 times the normal level by term.
- Why doesn't lactation occur during pregnancy? Despite high prolactin levels, high estrogen and progesterone from the placenta block prolactin's action on the breast - suppressing actual milk secretion.
- At parturition, the sudden fall in estrogen and progesterone (after placental delivery) removes this inhibition, and prolactin can now act freely - milk secretion begins within 1-7 days.
- The fluid secreted in the first few days before and after birth is colostrum - rich in proteins, immunoglobulins, and lactose, but low in fat.
3. Maintenance of Lactation - Suckling Reflex
Continued lactation depends on the neuroendocrine suckling reflex, involving two key hormones:
a) Prolactin (milk production):
- Suckling sends afferent nerve impulses from nipple mechanoreceptors → hypothalamus → causes a 10-20-fold surge in prolactin lasting ~1 hour.
- This surge keeps alveolar cells secreting milk for the next nursing period.
- Without regular suckling, milk production ceases within ~1 week.
b) Oxytocin (milk ejection/let-down reflex):
- Suckling (and also auditory, visual, olfactory stimuli associated with the baby) → hypothalamic nuclei → posterior pituitary releases oxytocin.
- Oxytocin causes contraction of myoepithelial cells surrounding the alveoli and ducts → milk is ejected through the nipple (let-down reflex).
- Emotional stress can inhibit oxytocin release and thus inhibit milk let-down.
4. Hypothalamic Control of Prolactin
The hypothalamus uniquely inhibits prolactin (unlike its stimulatory control of other pituitary hormones):
- Prolactin Inhibitory Hormone (PIH) = Dopamine, secreted by arcuate nucleus, travels via portal system to anterior pituitary, suppressing prolactin up to 10-fold.
- Suckling suppresses dopamine release → allows prolactin surge.
- Drugs blocking dopamine (e.g., antipsychotics) can cause galactorrhea; dopamine agonists (e.g., bromocriptine) suppress lactation.
- Prolactin Releasing Factor (PRF): TRH also has a minor prolactin-releasing effect.
5. Lactation Amenorrhea
As long as suckling continues:
- Elevated prolactin → inhibits GnRH secretion from hypothalamus → suppresses FSH and LH from anterior pituitary → ovulation is suppressed.
- This is the basis of lactational amenorrhea - breast-feeding acts as a natural (though not 100% effective) contraceptive method.
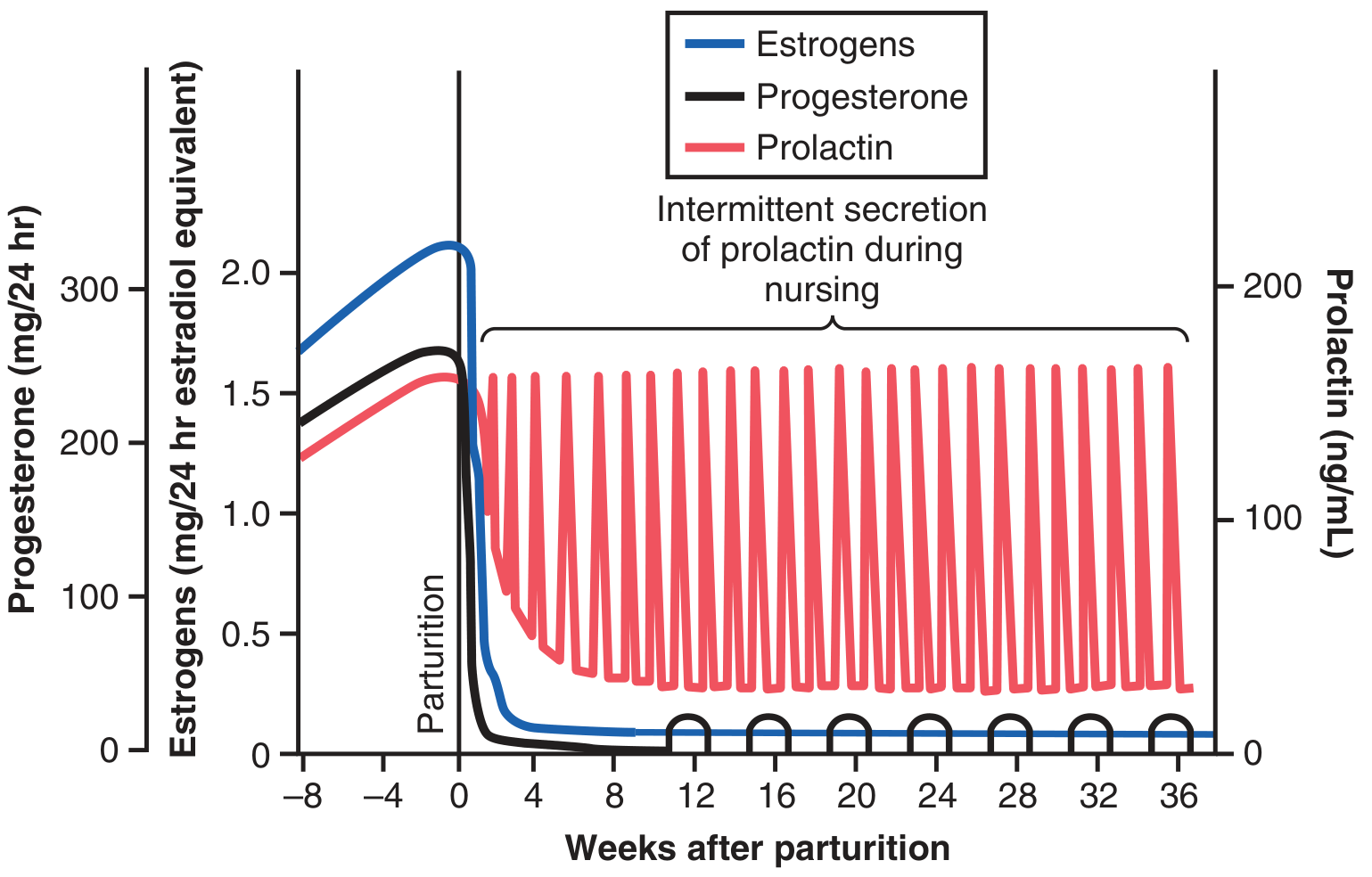
Fig: Changes in estrogen, progesterone, and prolactin around parturition. Note the sharp fall in estrogen/progesterone at birth, and the intermittent prolactin surges with each nursing episode.
Summary Table
| Phase | Key Hormone | Action |
|---|---|---|
| Breast development | Estrogen + Progesterone | Duct + lobulo-alveolar growth |
| Milk suppression (pregnancy) | Estrogen + Progesterone | Block prolactin action |
| Initiation post-partum | Prolactin (unopposed) | Triggers milk secretion |
| Milk production maintenance | Prolactin surge (suckling) | Keeps alveoli secreting |
| Milk ejection | Oxytocin | Myoepithelial contraction |
| Lactational amenorrhea | Prolactin | Suppresses GnRH → no ovulation |
Sources: Guyton and Hall Textbook of Medical Physiology, pp. 1044-1046 | Ganong's Review of Medical Physiology, 26th ed., pp. 419-420 | Costanzo Physiology, 7th ed., p. 484
Give the answer again
Physiology of Lactation
1. Development of the Breast (Mammogenesis)
Breast development for lactation occurs in stages under hormonal control:
- Estrogens stimulate growth of the ductal system and fat deposition. During pregnancy, placental estrogens cause the ductal system to grow and branch extensively.
- Progesterone drives full development of the lobule-alveolar system - stimulates budding of alveoli and secretory differentiation of alveolar cells.
- Supporting hormones: growth hormone, prolactin, adrenal glucocorticoids, and insulin - all involved in protein metabolism needed for breast tissue growth.
2. Initiation of Lactation (Lactogenesis) - Role of Prolactin
Prolactin is the key lactogenic hormone, secreted by the anterior pituitary.
- During pregnancy, prolactin levels rise steadily from the 5th week to 10-20 times the normal level by term.
- Why doesn't lactation occur during pregnancy? Despite high prolactin, high estrogen and progesterone from the placenta block prolactin's action on the breast - suppressing actual milk secretion.
- At parturition, the sudden fall in estrogen and progesterone (after placental delivery) removes this inhibition - milk secretion begins within 1-7 days.
- The fluid secreted in the first few days is colostrum - rich in proteins and immunoglobulins, low in fat.
3. Maintenance of Lactation - Suckling Reflex
Continued lactation depends on the neuroendocrine suckling reflex, involving two key hormones:
a) Prolactin (milk production):
- Suckling → afferent nerve impulses from nipple mechanoreceptors → hypothalamus → 10-20-fold surge in prolactin lasting ~1 hour.
- This surge keeps alveolar cells secreting milk for the next nursing period.
- Without regular suckling, milk production ceases within ~1 week.
b) Oxytocin (milk ejection / let-down reflex):
- Suckling (and also auditory, visual, olfactory stimuli associated with the baby) → hypothalamic nuclei → posterior pituitary releases oxytocin.
- Oxytocin causes contraction of myoepithelial cells surrounding the alveoli and ducts → milk is ejected through the nipple.
- Emotional stress can inhibit oxytocin release and thus inhibit milk let-down.
4. Hypothalamic Control of Prolactin
The hypothalamus uniquely inhibits prolactin (unlike its stimulatory control of other pituitary hormones):
- Prolactin Inhibitory Hormone (PIH) = Dopamine, secreted by the arcuate nucleus, travels via the hypothalamo-hypophysial portal system to suppress prolactin secretion up to 10-fold.
- Suckling suppresses dopamine release → allows the prolactin surge.
- Drugs blocking dopamine (e.g., antipsychotics) can cause galactorrhea; dopamine agonists (e.g., bromocriptine) suppress lactation.
- TRH has a minor prolactin-releasing effect.
5. Lactation Amenorrhea
As long as suckling continues:
- Elevated prolactin → inhibits GnRH secretion from hypothalamus → suppresses FSH and LH from anterior pituitary → ovulation is suppressed.
- This is the basis of lactational amenorrhea - breast-feeding acts as a natural (though not 100% effective) contraceptive.
Estrogen and progesterone fall sharply at parturition; prolactin shows intermittent surges with each nursing episode (Guyton & Hall, Fig. 83.12)
Summary Table
| Phase | Key Hormone | Action |
|---|---|---|
| Breast development | Estrogen + Progesterone | Duct + lobulo-alveolar growth |
| Milk suppression (pregnancy) | Estrogen + Progesterone | Block prolactin action on breast |
| Initiation post-partum | Prolactin (unopposed) | Triggers copious milk secretion |
| Milk production maintenance | Prolactin surge (suckling) | Keeps alveoli secreting |
| Milk ejection | Oxytocin | Myoepithelial contraction (let-down) |
| Lactational amenorrhea | Prolactin | Suppresses GnRH → no ovulation |
Sources: Guyton and Hall Textbook of Medical Physiology, pp. 1044-1046 | Ganong's Review of Medical Physiology, 26th ed., pp. 419-420 | Costanzo Physiology, 7th ed., p. 484

Screenshot_20260618-231335_Image to PDF Converter.png
Can you provide the answers for the physiological basis qns for 4 marks ? 1st year mbbs level strictly
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
All 14 answers are covered. Here's a quick reference summary of the key points for each:
Quick Revision Bullets:
| Q | Key Concept |
|---|---|
| 1 | Puberty = pulsatile GnRH → FSH/LH → sex steroids |
| 2 | Sertoli cells = nurse + blood-testis barrier + ABP + inhibin |
| 3 | Cryptorchidism = higher temp → heat-sensitive germinal epithelium destroyed |
| 4 | Hot work environment = elevated scrotal temp → same as cryptorchidism |
| 5 | Testosterone → EPO + bone marrow stimulation → RBC; loss = anemia |
| 6 | Post-ovulation = corpus luteum → progesterone → thermogenic → ↑BBT by 0.2-0.5°C |
| 7 | Menstrual blood = fibrinolysin lyses clots as fast as they form |
| 8 | hCG (from trophoblast) has antigenicity → anti-hCG antibodies used for detection |
| 9 | Blocked tube → embryo implants in tube → tube ruptures (can't expand) |
| 10 | Preterm = no cortisol surge → no surfactant → RDS; betamethasone matures lungs |
| 11 | Ovum lives 12-24h, sperm 48-72h; avoid Day 10-17 of 28-day cycle |
| 12 | OCP = negative feedback on pituitary → no LH surge → no ovulation (primary) |
| 13 | IUCD = foreign body inflammation → hostile to sperm + implantation |
| 14 | Copper-T = IUCD + Cu²⁺ ions directly toxic to sperm (spermicidal) |
Can you give the answer for the physiological basis again
Section IV – Explain the Physiological Basis (4 Marks Each)
1. Puberty
- The primary event at puberty is the initiation of pulsatile GnRH secretion from the hypothalamus (previously suppressed by a CNS inhibitory mechanism in childhood).
- Pulsatile GnRH → pulsatile FSH and LH release from anterior pituitary.
- Males: LH → Leydig cells → testosterone → secondary sexual characters (beard, voice change, muscle growth). FSH + testosterone → spermatogenesis.
- Females: FSH → follicular development → estrogen → breast development, uterine growth, menarche. LH surge → ovulation.
- Adrenarche: Adrenal androgens (DHEA) cause pubic and axillary hair in both sexes.
- Early puberty shows nocturnal LH pulses (sleep-entrained gonadotropin surges).
2. Sertoli Cells are Important in Spermatogenesis
Sertoli cells (lining the seminiferous tubules) are essential for spermatogenesis through multiple functions:
| Function | Role |
|---|---|
| Nurse/sustentacular cells | Provide nutrients and energy to developing germ cells |
| Blood-testis barrier | Tight junctions between Sertoli cells protect spermatocytes from immune attack (immune privilege) |
| Secrete ABP (Androgen Binding Protein) | Concentrates testosterone inside tubule - essential for spermatogenesis |
| Secrete inhibin | Negative feedback on FSH - regulates sperm output |
| Phagocytosis | Remove residual bodies and defective germ cells |
| FSH target | FSH acts on Sertoli cells to initiate and maintain spermatogenesis |
Without functional Sertoli cells, spermatogenesis completely fails.
3. Sterility in Undescended Testis / Spermatogenesis Markedly Reduced
- Normally the testes descend into the scrotum where the temperature is 2-3°C lower than core body temperature (scrotal temp ~34°C vs. body temp 37°C).
- Spermatogenesis requires this lower temperature - the enzymes involved in meiosis and spermiogenesis are heat-sensitive.
- In cryptorchidism, the testis remains in the inguinal canal or abdomen at 37°C.
- This higher temperature damages the germinal epithelium (spermatogonia degenerate) → markedly reduced or absent spermatogenesis → sterility.
- Leydig cells are more heat-resistant - so testosterone secretion and secondary sexual characters are usually preserved.
- The scrotum maintains low temperature via the pampiniform plexus (countercurrent heat exchange) and cremaster muscle reflexes.
4. Sterility in Man Working in Hot Surroundings
- Same fundamental principle: spermatogenesis requires scrotal temperature 2-3°C below core body temperature.
- Men working continuously in hot environments (furnace workers, bakers, welders) have persistently elevated scrotal temperatures.
- Even a rise of 1-2°C above normal scrotal temperature impairs spermatogenesis.
- Prolonged heat exposure → degeneration of germinal epithelium → oligospermia or azoospermia → infertility.
- The normal thermoregulatory mechanisms (pampiniform plexus, cremaster muscle) are overwhelmed by sustained environmental heat.
- This is potentially reversible if heat exposure is removed and the germinal epithelium recovers.
- Same principle explains why tight underwear, hot baths, and laptop use on the lap can reduce sperm counts.
5. Anemia in Hypogonadism of Male
- Testosterone has a direct stimulatory effect on erythropoiesis (RBC production) through two mechanisms:
- Stimulates the kidneys to secrete erythropoietin (EPO) → EPO acts on bone marrow → increases RBC production.
- Direct stimulation of bone marrow erythroid stem cells.
- In hypogonadism (testicular failure or hypopituitarism), testosterone levels are very low.
- Low testosterone → decreased EPO → decreased RBC production → normocytic normochromic anemia.
- This explains why normal males have higher hemoglobin (15.5 g/dL) than females (14 g/dL) - due to testosterone.
- Testosterone replacement therapy in hypogonadal males corrects the anemia.
6. Body Temperature is Slightly Elevated After Ovulation
- After ovulation, the ruptured Graafian follicle becomes the corpus luteum, which secretes large amounts of progesterone.
- Progesterone has a thermogenic (heat-producing) effect - acts on the hypothalamic thermoregulatory center to raise the temperature set-point.
- Basal body temperature (BBT) rises by 0.2-0.5°C (about 0.5°F) after ovulation and remains elevated throughout the luteal phase (~14 days).
- When corpus luteum regresses before menstruation → progesterone falls → BBT drops back to baseline.
- Clinical use: BBT charting confirms ovulation has occurred (biphasic chart = ovulatory cycle). However, since the rise occurs 1-2 days after ovulation, it predicts the next cycle rather than the current one.
7. Menstrual Blood Does Not Clot
Normal blood clots due to the coagulation cascade, but menstrual blood does not, for the following reasons:
- Fibrinolysin (Plasmin): The shedding endometrium produces large amounts of fibrinolysin - this enzyme breaks down fibrin clots as quickly as they form, preventing coagulation.
- Prostaglandins (PGE2, PGF2α): Present in high amounts in menstrual blood; promote fibrinolysis.
- Tissue thromboplastin released is minimal compared to the overwhelming fibrinolytic activity.
- Menstrual bleeding is from small spiral arterioles - the flow dynamics differ from wound bleeding.
- If flow is excessively heavy (menorrhagia), fibrinolysin is insufficient to lyse all clots → clots appear in heavy flow, which is considered abnormal.
8. Immunological Test of Pregnancy
- After implantation (~day 8-10), the trophoblast cells secrete human Chorionic Gonadotropin (hCG) into maternal blood and urine.
- hCG is a glycoprotein with antigenic properties and a unique β subunit (β-hCG).
- Animals (rabbits/sheep) immunized with hCG produce anti-hCG antibodies.
Principle of the test:
- Patient's urine + anti-hCG antibodies + hCG-coated particles:
- Pregnant (hCG present in urine): hCG neutralizes antibodies → agglutination inhibited = Positive.
- Not pregnant (no hCG): Antibodies react with particles → agglutination occurs = Negative.
- Modern home pregnancy tests use monoclonal anti-β-hCG antibodies on a lateral flow strip.
- Also positive in: hydatidiform mole, choriocarcinoma, ectopic pregnancy (all produce hCG).
9. Ectopic Pregnancy
Definition: Implantation of the fertilized ovum outside the uterus (~90% in the fallopian tube).
Physiological Basis - Why it occurs:
- Fertilization normally occurs in the ampulla of the fallopian tube. The embryo is transported to the uterus by:
- Ciliary beating of tubal epithelium
- Peristaltic muscular contractions of the tube
- Tubal fluid current
- If transport is impaired, the embryo implants in the tube.
Common causes:
- Salpingitis/PID - scarring destroys cilia and impairs muscular contractions
- Previous tubal surgery, endometriosis, congenital tubal abnormality
Why it is dangerous:
- The fallopian tube cannot expand like the uterus to accommodate the growing embryo.
- The trophoblast erodes through the thin tubal wall → tube ruptures at 6-8 weeks → life-threatening intraperitoneal hemorrhage.
10. Corticosteroids are Administered to a Lady in Preterm Labour
- The major risk of premature birth (before 34 weeks) is Respiratory Distress Syndrome (RDS) / Hyaline Membrane Disease in the newborn.
- RDS occurs because fetal lungs are immature - insufficient pulmonary surfactant.
- Surfactant (dipalmitoyl phosphatidylcholine) is produced by Type II pneumocytes. It reduces alveolar surface tension and prevents alveolar collapse at end-expiration.
- Surfactant production is triggered by cortisol - fetal cortisol normally rises in the last weeks of pregnancy (34-36 weeks) to mature the lungs naturally.
- In preterm labour, this cortisol surge has not yet occurred.
Why corticosteroids are given:
- Betamethasone or Dexamethasone (given to mother) → cross the placenta → act on fetal Type II pneumocytes → accelerate surfactant synthesis within 24-48 hours → lung maturity is achieved.
- Significantly reduces RDS, neonatal mortality, and intraventricular hemorrhage.
11. Safe Period as a Contraceptive Method
Physiological Basis:
- Conception requires a viable sperm to meet a viable ovum.
- Ovum viability: Ovum survives only 12-24 hours after ovulation.
- Sperm viability: Sperms survive in the female tract for 48-72 hours (up to 5 days).
- Therefore, pregnancy is only possible during a narrow fertile window around ovulation.
Calculation (28-day regular cycle):
- Ovulation on Day 14 (±2 days).
- Unsafe (fertile) period = Day 10 to Day 17.
- Safe period = Day 1-9 (post-menstrual) and Day 18-28 (pre-menstrual).
Limitations:
- Unreliable in women with irregular cycles.
- Relatively high failure rate (~20%).
- Also called the rhythm method / calendar method.
12. Contraceptive Pills
Combined OCPs contain synthetic estrogen + progestin. They prevent pregnancy through multiple mechanisms:
| Mechanism | Effect |
|---|---|
| Negative feedback on hypothalamus-pituitary | ↓GnRH → ↓FSH and LH → no LH surge → no ovulation (PRIMARY mechanism) |
| Hostile cervical mucus | Progestin thickens mucus → impenetrable to sperms |
| Endometrial changes | Atrophic endometrium → unsuitable for implantation |
| Altered tubal motility | Impairs sperm and ovum transport |
- Pills create an artificial luteal-phase environment - the pituitary "thinks" the woman is already pregnant (high estrogen + progesterone) → suppresses gonadotropins.
- Taken for 21 days, 7-day pill-free interval → withdrawal bleed occurs.
- Failure rate: <1% with perfect use.
13. Intra-Uterine Contraceptive Devices (IUCDs) Prevent Pregnancy
IUCDs prevent pregnancy through several mechanisms:
- Foreign body reaction: IUCD causes a sterile inflammatory reaction in the endometrium → increased leucocytes, macrophages, and prostaglandins → hostile environment for sperms (phagocytosed) and implantation.
- Altered uterine and tubal motility: Prostaglandins impair sperm transport and ovum pick-up.
- Endometrial changes: Inflammatory reaction makes endometrium biochemically unsuitable for implantation of the blastocyst.
- Hormone-releasing IUDs (Mirena): Additionally thicken cervical mucus and suppress endometrium.
- IUCDs generally do not prevent ovulation (except hormonal IUDs partially).
- Failure rate: ~0.5-1% per year - highly effective.
14. Copper-T
Copper-T is a T-shaped IUCD with copper wire wound around it. It works through all IUCD mechanisms plus additional copper-specific effects:
- Spermicidal action of copper ions (Cu²⁺):
- Cu²⁺ ions released continuously into uterine cavity.
- Directly toxic to sperms - impairs sperm motility, inhibits acrosomal enzyme activity, alters sperm membrane → sperms cannot fertilize the ovum.
- Enhanced inflammatory reaction - copper intensifies leucocytic response in endometrium.
- Endometrial biochemical changes - copper ions further impair implantation.
- Cervical mucus changes - copper ions make mucus more hostile to sperms.
Advantages:
- More effective than plain IUCDs due to added spermicidal effect.
- Effective for 5-10 years.
- Can be used as emergency contraception if inserted within 5 days of unprotected intercourse.
- Failure rate: 0.6-0.8% per year.
Sources: Guyton & Hall Textbook of Medical Physiology | Ganong's Review of Medical Physiology (26th ed.) | Costanzo Physiology (7th ed.) | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.