Gerd 101
Reading File
Finding Sources
Searching PubMed
"gastroesophageal reflux disease" management
Searching the Web
GERD gastroesophageal reflux disease overview 2025 guidelines
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed. Let me compile the complete GERD 101 overview.
GERD 101 - Gastroesophageal Reflux Disease
Definition
GERD is a condition characterized by chronic symptoms or complications resulting from the retrograde flow of gastric contents across an inappropriately relaxed or compromised lower esophageal sphincter (LES) into the esophagus. The Montreal Consensus defines it as occurring when reflux "causes troublesome symptoms and/or complications." It affects 20-30% of the US population and costs an estimated $12-20 billion annually in direct healthcare expenditure.
- Current Surgical Therapy 14e
- Murray & Nadel's Textbook of Respiratory Medicine
Pathophysiology
GERD results from an imbalance between the transdiaphragmatic pressure gradient and the valve mechanism at the esophagogastric junction (EGJ).
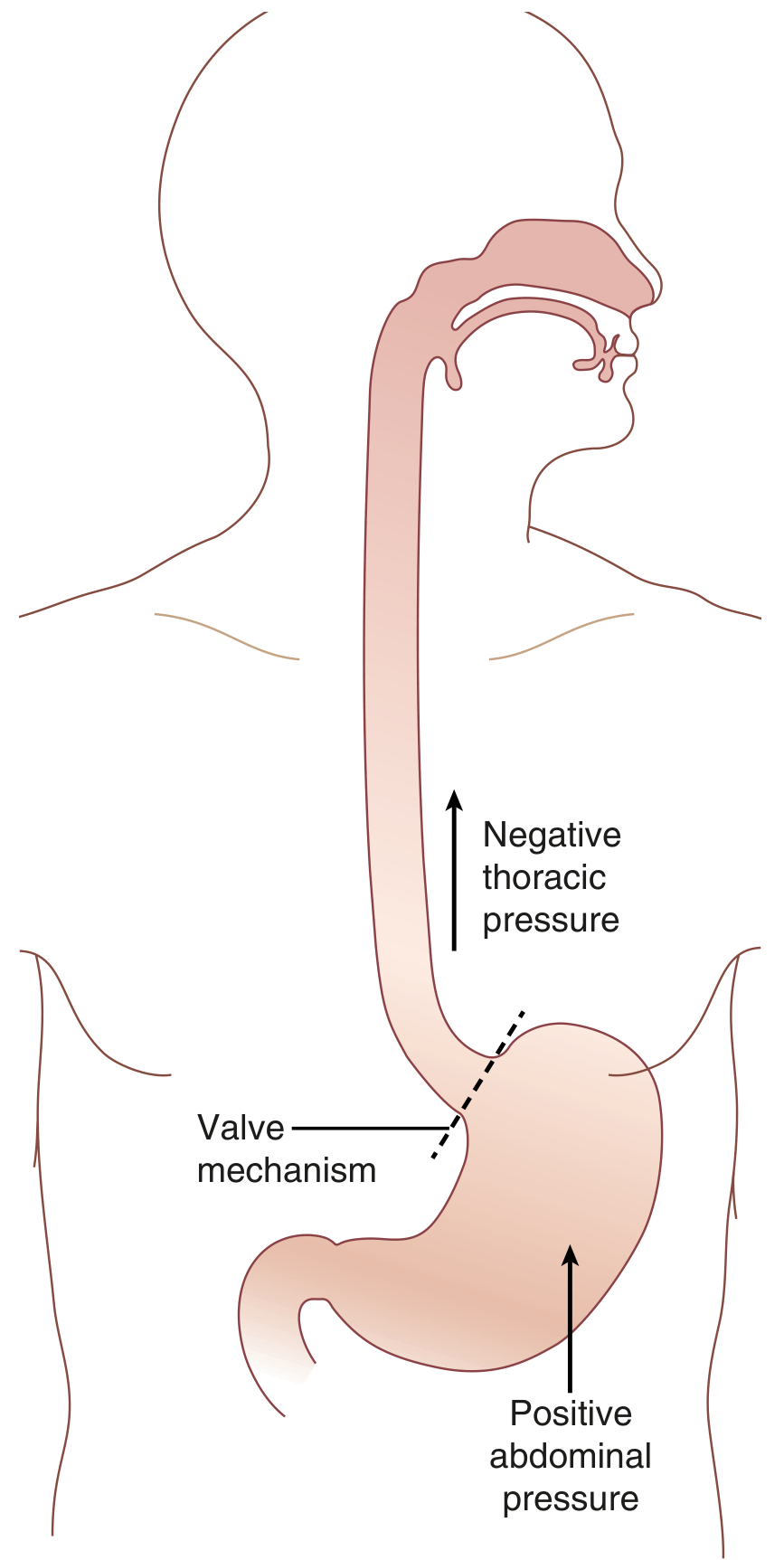
GERD pathophysiology: the valve mechanism at the EGJ must overcome negative thoracic pressure (drawing contents upward) and positive abdominal pressure (compressing gastric contents upward). - Sabiston Textbook of Surgery
The Anti-Reflux Barrier - 5 Components
The EGJ valve is composed of:
-
Lower Esophageal Sphincter (LES) - a 3-4 cm smooth muscle segment creating a sustained high-pressure zone. Most GERD patients have a defective LES. Additionally, excessive transient LES relaxations (TLESRs) are a major contributing mechanism.
-
Diaphragmatic crus - provides extrinsic compression on the LES, pinching the lower esophagus during increased abdominal pressure.
-
Angle of His - the acute angle between the esophagus and gastric fundus acts as a barrier to refluxate rise.
-
Gubaroff valve - a thickening of esophageal mucosa at the EGJ acting as a cushion keeping the area closed.
-
Intraabdominal esophageal segment - positive abdominal pressure collapses this segment, contributing to the valve effect.
- Sabiston Textbook of Surgery
What Breaks the Barrier?
| Mechanism | Clinical Example |
|---|---|
| Increased abdominal pressure | Obesity (especially central), pregnancy, athletes |
| Decreased thoracic pressure | Obstructive pulmonary disease, glass blowers, singers |
| Defective valve | Hiatal hernia (most common) - disrupts all 5 components |
| Reduced LES tone | Scleroderma, pregnancy (progesterone), certain drugs |
| Excessive TLESRs | Gastric distention after meals |
| Delayed gastric emptying | Gastroparesis (contributes in ~1/3 of cases) |
Hiatal hernia is the most important structural cause: it eliminates intraabdominal esophageal length, makes the angle of His obtuse, places the LES in a negative pressure environment, and prevents the diaphragm from reinforcing the LES.
- Sabiston Textbook of Surgery, Harrison's Principles of Internal Medicine 22E
Obesity and GERD
Obesity (OR = 2.15, 95% CI 1.89-2.45) is a major independent risk factor. Abdominal obesity raises intraabdominal pressure, reduces LES pressure and intraabdominal LES length, increases gastric acid production, and induces esophageal motor dysfunction. The association is stronger in Caucasians and in women (partly due to estrogen levels).
- Yamada's Textbook of Gastroenterology, 7e
Symptoms
Symptoms are classified as typical, atypical, or alarm:
Typical Symptoms
- Heartburn (pyrosis) - burning sensation rising from the stomach/lower chest toward the neck and throat; usually postprandial; worsened by spicy food, citrus, fats, chocolate, alcohol, supine position, bending over. GERD is usually diagnosed symptomatically when heartburn occurs ≥2 days/week, though less frequent symptoms don't exclude the diagnosis.
- Regurgitation - perception of refluxed gastric contents flowing into the mouth or pharynx. Patients with daily regurgitation often have low LES pressure, associated gastroparesis, and esophagitis.
- Acid brash
Atypical (Extraesophageal) Symptoms
- Chronic cough
- Wheezing / asthma
- Dysphonia / voice changes
- Sore throat
- Globus sensation
- Noncardiac chest pain
- Dental erosions
- Laryngitis
Alarm Symptoms - Require Further Workup
These raise suspicion for malignancy or complications and should never be attributed solely to uncomplicated GERD:
- Dysphagia / odynophagia
- Unintended weight loss
- Anorexia / early satiety
- GI bleeding
Important caveat: Symptom severity does not predict the degree of esophageal damage. Heartburn + regurgitation have a sensitivity and specificity of only ~63% each for GERD by objective criteria (the Diamond Study). A positive PPI trial is seen in 69% of GERD patients and 51% of non-GERD patients - so the PPI trial alone is not a reliable diagnostic tool.
- Sleisenger & Fordtran's GI and Liver Disease, Current Surgical Therapy 14e
Diagnosis
Step-Up Approach
1. Clinical diagnosis - sufficient for typical symptoms (heartburn ≥2x/week) without alarm features.
2. Ambulatory pH monitoring - the gold standard. Options:
- 24-hour dual-probe catheter (transnasal)
- 48-hour wireless capsule (endoscopic placement)
- Thresholds: DeMeester score >14.72 or total distal esophageal acid exposure time >5-6% indicates pathologic reflux
3. Upper endoscopy - confirms diagnosis if LA Grade C/D esophagitis, Barrett's metaplasia, or peptic stricture are found. Also identifies hiatal hernias, retained food (delayed gastric emptying).
LA Classification of Esophagitis:
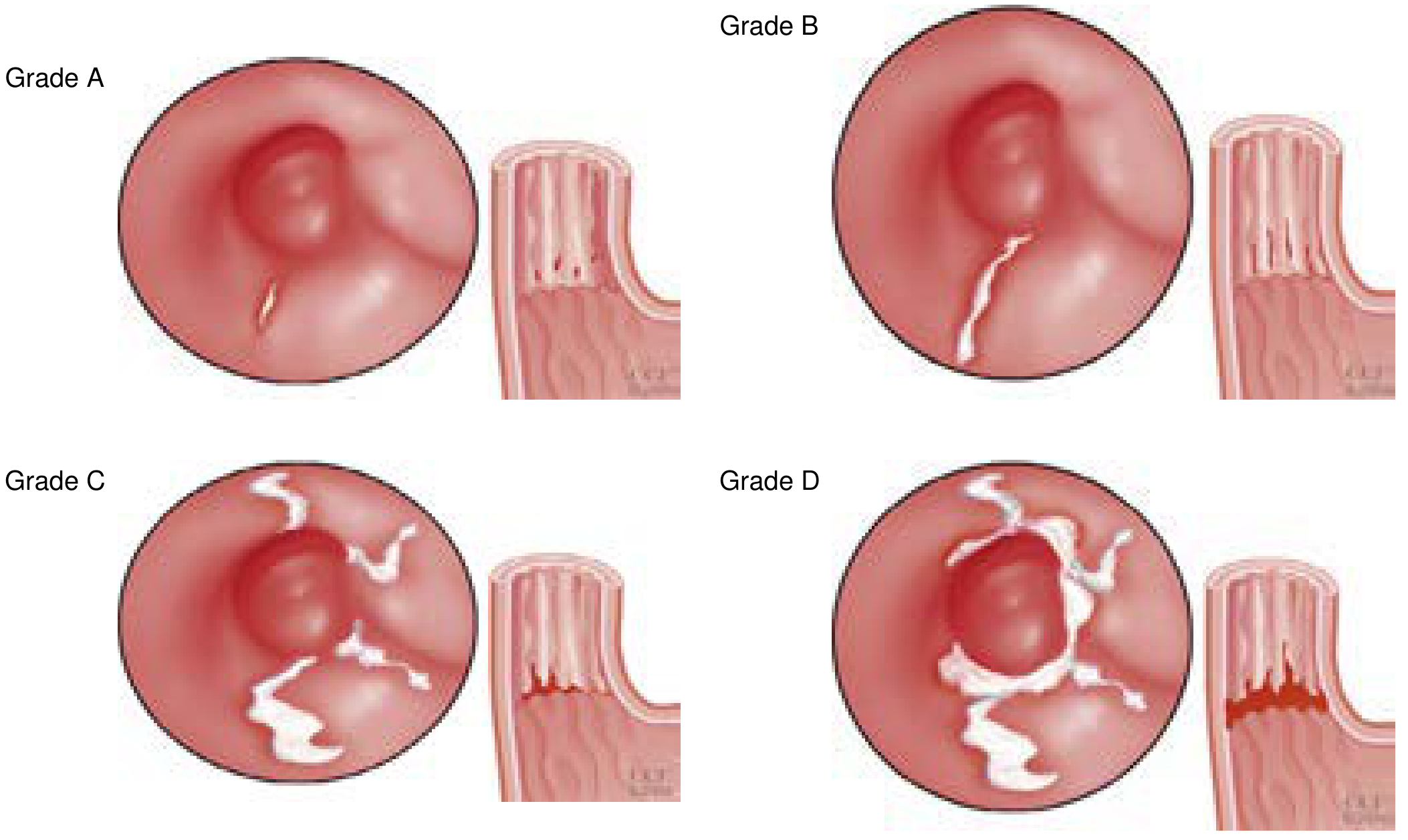
| Grade | Finding |
|---|---|
| A | ≥1 mucosal break <5 mm, not extending between fold tops |
| B | ≥1 mucosal break >5 mm, not extending between fold tops |
| C | ≥1 mucosal break continuous between fold tops, <75% circumference |
| D | ≥1 mucosal break involving ≥75% of esophageal circumference |
4. Esophageal manometry - used to:
- Assess esophageal motility (guides fundoplication choice)
- Rule out achalasia (which can mimic GERD)
- Chicago Classification v4.0: if ineffective esophageal motility is present, prefer partial (Toupet 270°) over complete (Nissen 360°) fundoplication to reduce postoperative dysphagia
5. Barium swallow - useful for anatomical assessment (hiatal hernia size, esophageal shortening).
- Current Surgical Therapy 14e, Sabiston Textbook of Surgery
Complications
| Complication | Notes |
|---|---|
| Erosive esophagitis | ~50% of GERD patients; graded by LA Classification |
| Peptic stricture | From chronic inflammation; presents with dysphagia; treated with dilation |
| Barrett's esophagus | Intestinal metaplasia replacing squamous epithelium; OR = 4.0 (1.4-11.1) with obesity; requires surveillance |
| Esophageal adenocarcinoma | Most feared complication; RR up to 4.8x in obesity; rising incidence directly linked to GERD epidemic |
| Extraesophageal complications | Laryngitis, dental erosions, chronic cough, aspiration pneumonia |
Factors predisposing to Barrett's include early-onset GERD, abnormal LES, abnormal esophageal body physiology, and mixed reflux (both gastric and duodenal contents).
- Yamada's, Mulholland & Greenfield's Surgery
Treatment
Step 1 - Lifestyle Modifications
- Weight loss (strongest evidence; proven in RCTs)
- Head-of-bed elevation (for nocturnal symptoms)
- Avoid large meals; avoid lying down within 2-3 hours of eating
- Avoid triggers: fatty foods, chocolate, coffee, alcohol, citrus, spicy food
- Quit smoking
Step 2 - Medical Therapy
Antacids: Fast-acting (minutes) but short-lived (1-2 hours); appropriate for infrequent, mild symptoms.
H2 Receptor Antagonists (H2RAs): e.g., famotidine, ranitidine (withdrawn from market)
- Onset slower than antacids, duration 6-10 hours
- Can be used prophylactically before meals
- Healing rate in erosive esophagitis: <50% - inadequate for significant disease
- Useful for infrequent heartburn (<3x/week)
Proton Pump Inhibitors (PPIs): e.g., omeprazole, pantoprazole, esomeprazole, lansoprazole
-
First-line for frequent heartburn, erosive esophagitis, and Barrett's
-
Superior acid suppression; once-daily dosing controls symptoms and heals erosive esophagitis in >80%
-
Should be taken 30-60 min before meals for optimal efficacy
-
Approximately 50% of Barrett's patients on full-dose PPIs still have abnormal acid exposure on pH monitoring - highlighting limits of medical therapy
-
Long-term use concerns: hypomagnesemia, C. difficile risk, bone density (controversial), B12 deficiency
-
Katzung's Basic and Clinical Pharmacology 16e, Yamada's Textbook of Gastroenterology
Step 3 - Surgical/Interventional Therapy
Indications for antireflux surgery (ARS):
- Failure or intolerance of medical therapy
- Patient preference (to avoid lifelong PPIs)
- Objective confirmation of GERD on pH testing
Laparoscopic Nissen fundoplication (360° posterior wrap):
- Standard of care for patients with normal esophageal motility
- Wraps the gastric fundus around the LES to recreate the valve mechanism
- Highly effective; most durable antireflux procedure
Laparoscopic Toupet fundoplication (270° posterior wrap):
- Preferred when ineffective esophageal motility is present (Chicago Classification v4.0)
- Reduces risk of postoperative dysphagia
Newer options: Transoral incisionless fundoplication (TIF), LINX magnetic sphincter augmentation device.
- Current Surgical Therapy 14e, Sabiston Textbook of Surgery
Special Populations
- Pregnancy: Reduced LES pressure from progesterone (in the setting of elevated estrogen) is the primary mechanism; symptoms are nearly universal in the third trimester; lifestyle measures first; antacids and H2RAs are generally safe.
- Elderly: May lack classic symptoms; can present with severe GERD or complications (ulceration, bleeding) as their first presentation; dysphagia and regurgitation are more common presenting features than heartburn.
- Obesity: Weight loss is a primary therapeutic target; bariatric surgery (particularly Roux-en-Y gastric bypass) resolves GERD in >85% of patients.
Summary Algorithm
Typical symptoms (heartburn/regurgitation ≥2x/week)
↓
No alarm symptoms → Empiric PPI trial (4-8 weeks)
↓
Responds → GERD confirmed → Lowest effective dose; lifestyle meds
↓
Fails OR alarm symptoms → Upper endoscopy + ambulatory pH testing
↓
Objective GERD confirmed → Optimize PPI; consider surgery if refractory
↓
Barrett's found → Surveillance endoscopy per protocol
Sources:
- Sabiston Textbook of Surgery (Antireflux Mechanism chapter)
- Current Surgical Therapy 14e (GERD chapter)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- Yamada's Textbook of Gastroenterology, 7e
- Katzung's Basic and Clinical Pharmacology, 16e
- Harrison's Principles of Internal Medicine, 22e (2025)
- Mulholland & Greenfield's Surgery, 7e
Sle 101 in detail please
Reading File
Finding Sources
Searching PubMed
"systemic lupus erythematosus" management guidelines
Searching the Web
systemic lupus erythematosus SLE 2024 2025 classification criteria treatment overview
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.