Most coomon ecgs in clinical practice in detailed picture
Reading File
Finding Sources
Searching Images
common ECG patterns clinical practice 12-lead electrocardiogram
Searching Images
atrial fibrillation ECG irregular rhythm no P waves
Searching Images
STEMI ST elevation myocardial infarction ECG
Searching Images
left bundle branch block right bundle branch block ECG
Searching Images
ventricular tachycardia ventricular fibrillation ECG arrhythmia
Searching Images
sinus bradycardia tachycardia normal sinus rhythm ECG
Searching Images
complete heart block first degree second degree AV block ECG
Searching Images
atrial flutter ECG sawtooth pattern
Searching Images
left ventricular hypertrophy ECG criteria
I have comprehensive image results for all major ECG patterns. Now I'll compile a detailed, well-organized response with all the images.
Most Common ECGs in Clinical Practice — Detailed Visual Guide
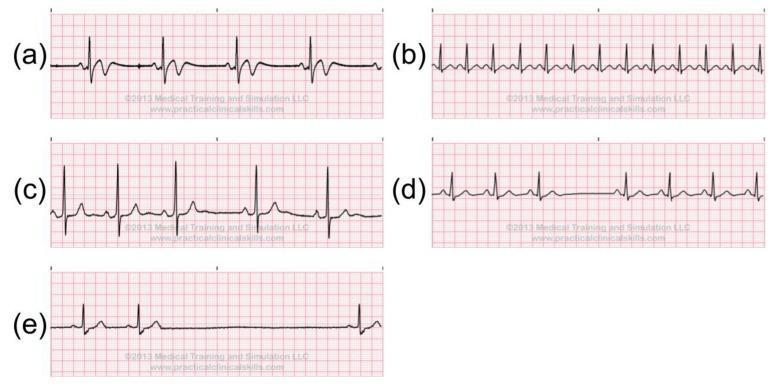
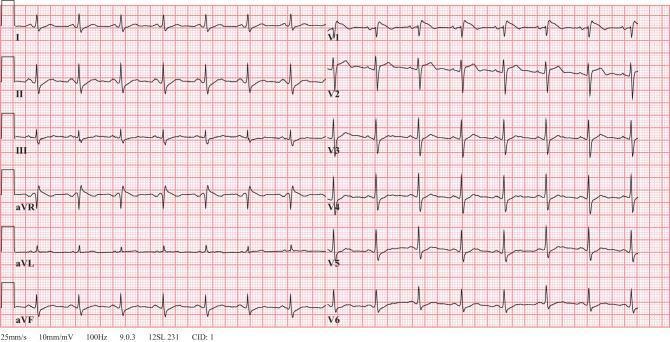
1. Normal Sinus Rhythm & Sinus Rate Variants
Normal sinus rhythm: Rate 60–100 bpm, regular P waves before every QRS, PR interval 120–200 ms, narrow QRS (<120 ms), positive P in II, negative in aVR.
Key variants shown below — sinus bradycardia (<60 bpm), sinus tachycardia (>100 bpm), sinus arrhythmia, sinus block, sinus arrest:
| Feature | Bradycardia | Normal | Tachycardia |
|---|---|---|---|
| Rate | <60 bpm | 60–100 bpm | >100 bpm |
| P–QRS relationship | 1:1, upright in II | 1:1 | 1:1 |
| QRS width | Narrow | Narrow | Narrow |
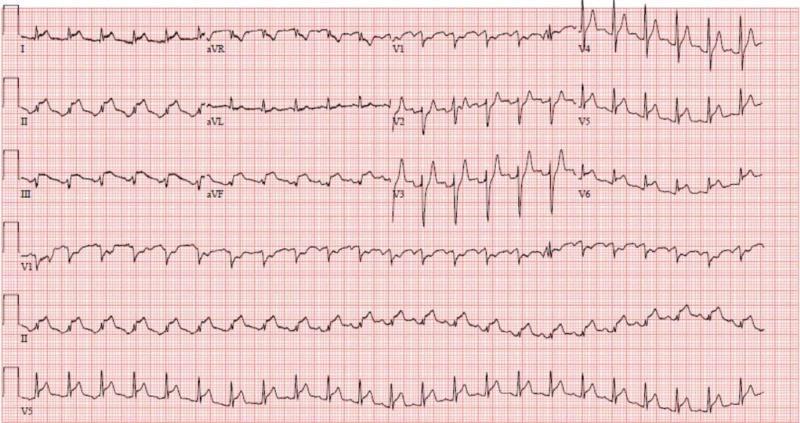
2. Atrial Fibrillation (AF)
The most common sustained arrhythmia in clinical practice.
ECG hallmarks:
- Irregularly irregular R–R intervals (no two are the same)
- Absent P waves — replaced by chaotic fibrillatory (f) waves, best seen in V1 and II
- Narrow QRS (unless aberrant conduction or accessory pathway)
- Ventricular rate varies (controlled <100 bpm; rapid response >100 bpm)

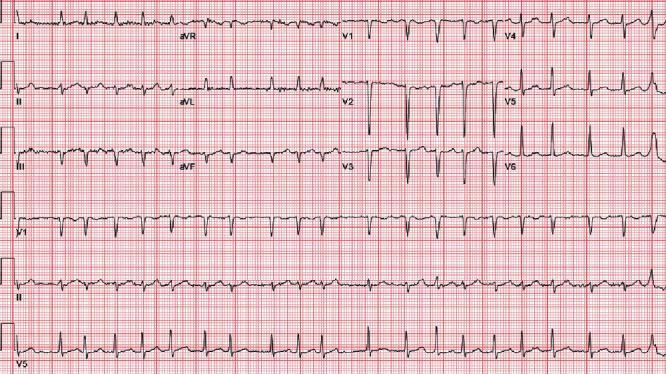
Coarse AF (large f-waves) can mimic atrial flutter — distinguish by lack of consistent sawtooth baseline.
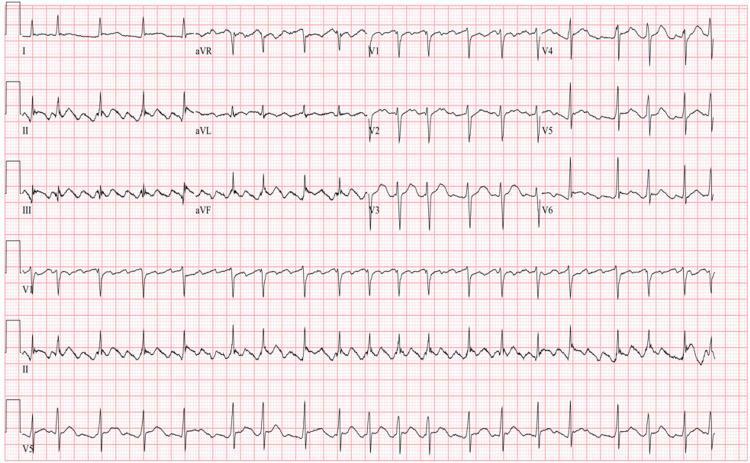
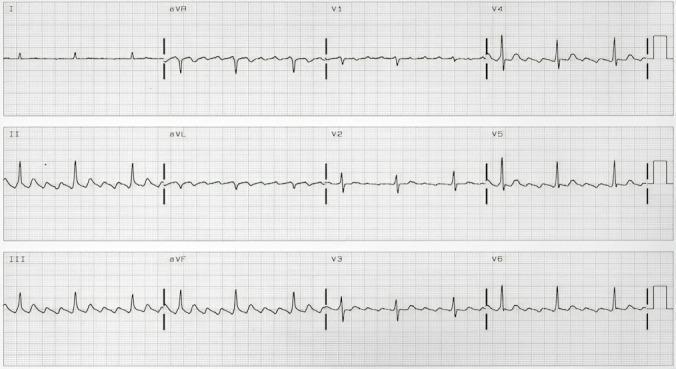
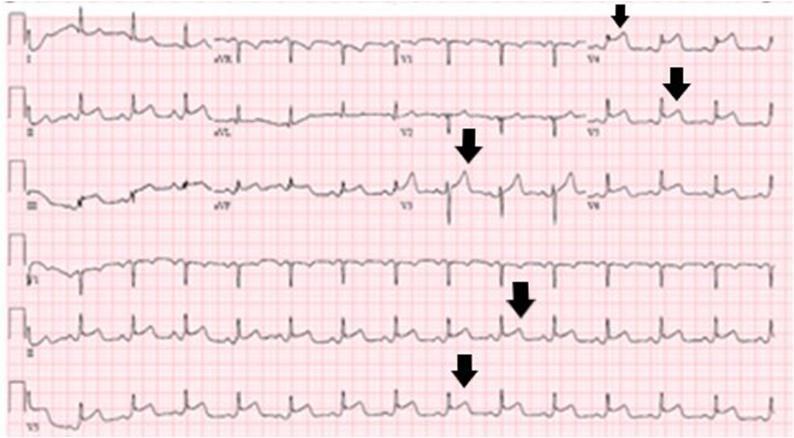
3. Atrial Flutter
ECG hallmarks:
- Classic "sawtooth" flutter waves (F-waves), rate ~300 bpm atrial
- Best seen in inferior leads (II, III, aVF) and V1
- Regular or variable ventricular response — commonly 2:1 conduction → ventricular rate ~150 bpm
- Narrow QRS
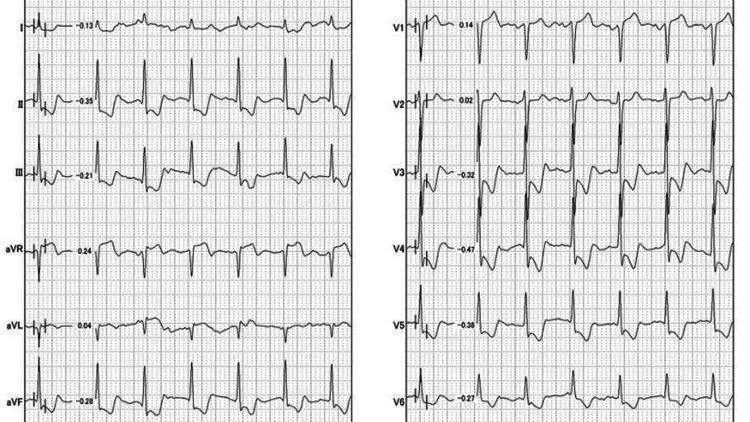
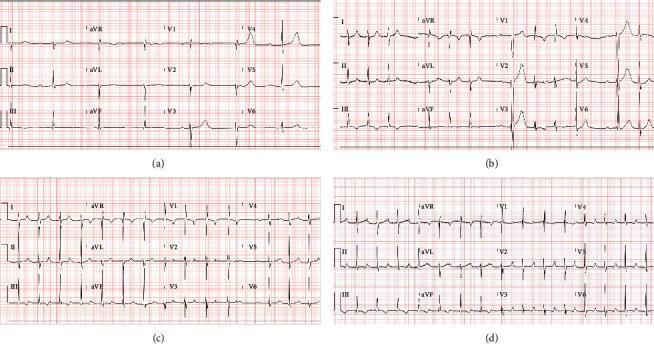
4. ST-Elevation Myocardial Infarction (STEMI)
ECG hallmarks:
- ST elevation ≥1 mm in ≥2 contiguous leads (≥2 mm in precordial leads)
- Convex/tombstone morphology in hyperacute phase
- Reciprocal ST depression in mirror leads
- Evolving Q waves = transmural necrosis
- Hyperacute T waves = earliest finding
Anterior STEMI (LAD territory — V1–V6, I, aVL):

Anterolateral STEMI (proximal LAD — V1–V6, I, aVL, reciprocal changes in II/III/aVF):

Inferolateral STEMI (RCA/LCx — II, III, aVF, V4–V6; reciprocal aVL depression):
STEMI Territory Localization:
| Leads | Territory | Artery |
|---|---|---|
| V1–V4 | Anterior | LAD |
| I, aVL, V5–V6 | Lateral | LCx |
| II, III, aVF | Inferior | RCA (80%), LCx (20%) |
| V1–V6 + I, aVL | Anterolateral | Proximal LAD / Left main |
| aVR elevation + diffuse ST↓ | Global ischemia | Left main / 3-vessel disease |
5. Global Ischemia / aVR Sign (Left Main / 3-Vessel Disease)
- ST elevation in aVR (≥1 mm) + diffuse ST depression in multiple leads
- Suggests severe hemodynamic compromise
- Associated with cardiogenic shock
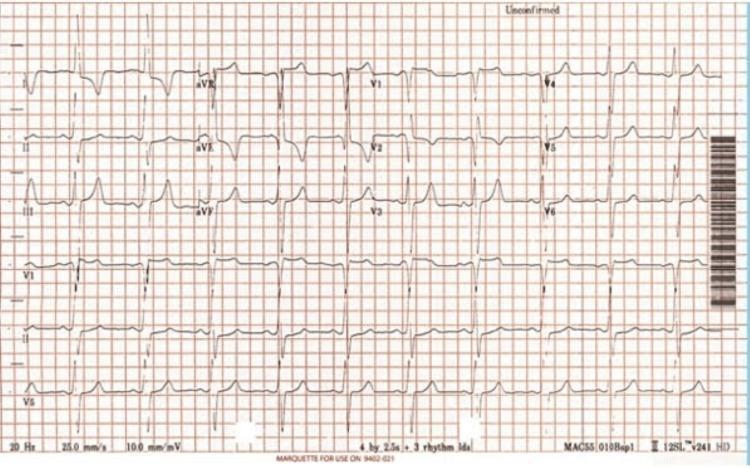
6. Bundle Branch Blocks
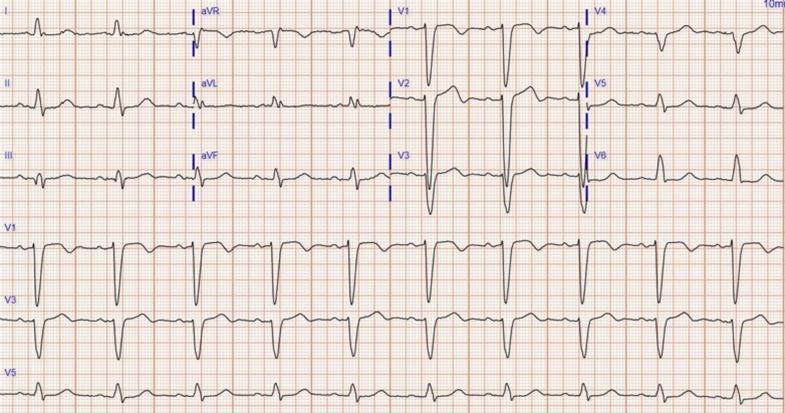
Left Bundle Branch Block (LBBB)
- Wide QRS ≥120 ms
- Broad monophasic R in I, aVL, V5, V6
- QS or rS pattern in V1 ("W" in V1, "M" in V6 — WiLLiaM)
- Secondary ST-T changes discordant to QRS
- New LBBB + chest pain = STEMI equivalent (Sgarbossa criteria)
Right Bundle Branch Block (RBBB)
- Wide QRS ≥120 ms
- rSR' ("rabbit ears") in V1–V2
- Wide S wave in I, V5–V6 ("M" in V1, "W" in V6 — MaRRoW)
- T-wave inversion in V1–V3
7. AV Blocks (Heart Blocks)
Comparison of all degrees:
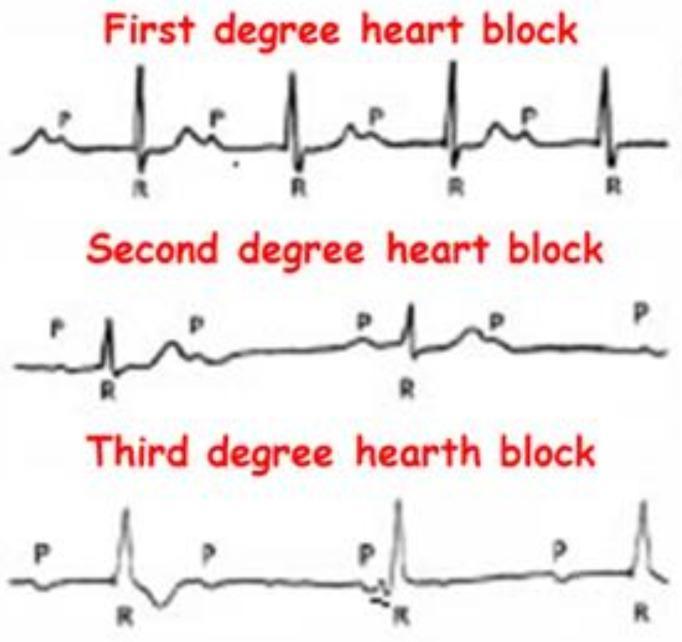
Clinical series — progression from 1st-degree to complete heart block:
| Type | PR Interval | P:QRS | QRS | Key Feature |
|---|---|---|---|---|
| 1st degree | >200 ms (prolonged) | 1:1 | Narrow | Every P conducts |
| 2nd degree Mobitz I (Wenckebach) | Progressive lengthening | >1:1 | Narrow | Dropped beat after PR lengthening |
| 2nd degree Mobitz II | Fixed (normal or long) | >1:1 | Wide | Sudden dropped beat, no PR change |
| 3rd degree (Complete) | AV dissociation | None | Wide or narrow | P and QRS independent |
Complete heart block (3rd degree):
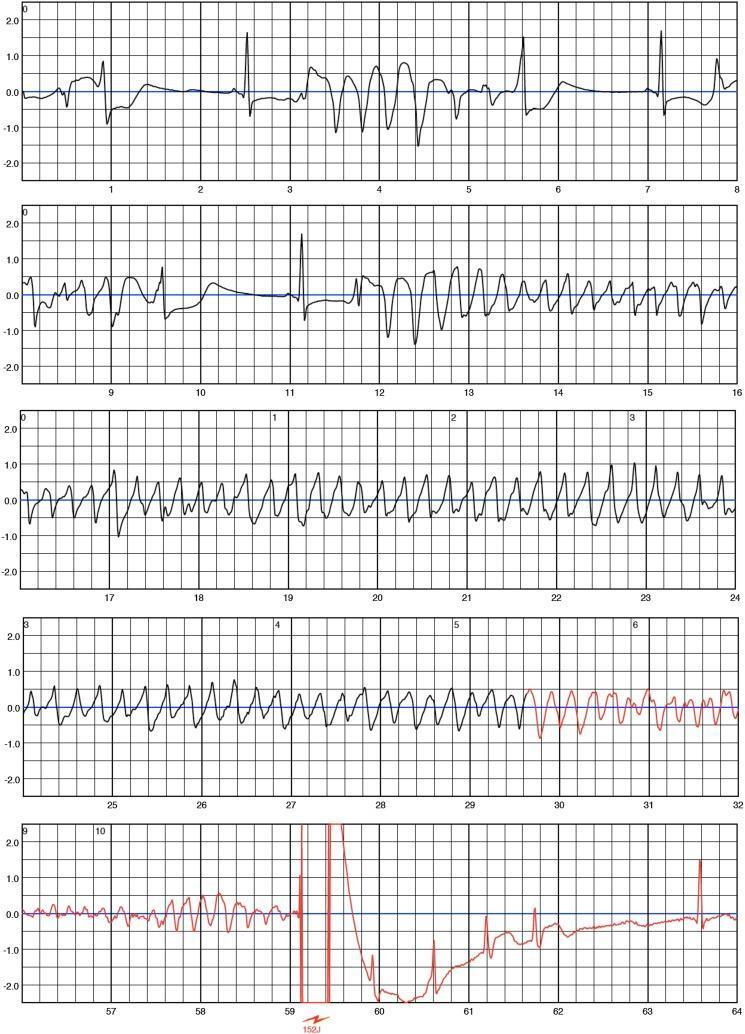
8. Ventricular Tachycardia (VT) & Ventricular Fibrillation (VF)
Ventricular Tachycardia (VT)
- Wide QRS (>120 ms) tachycardia, rate >100 bpm (usually 150–250)
- AV dissociation (P waves march through independently) — pathognomonic when seen
- Fusion beats and capture beats confirm VT
- LBBB-pattern VT with inferior axis → RVOT origin
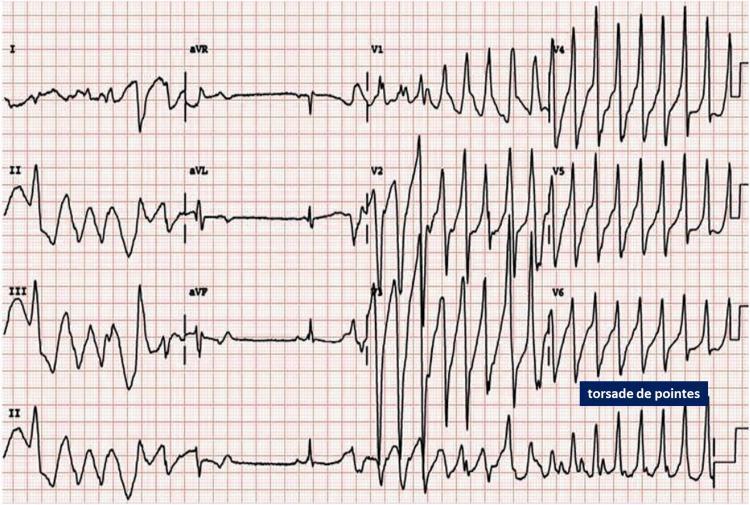
Torsades de Pointes (TdP)
- Polymorphic VT with twisting QRS axis around the isoelectric line
- Preceded by long QT (QTc >500 ms) and "short-long-short" RR sequence
- Causes: drugs (antiarrhythmics, antibiotics, antipsychotics), electrolyte disturbances
Ventricular Fibrillation (VF)
- Chaotic, disorganized deflections — no identifiable P, QRS, or T
- No cardiac output — cardiac arrest
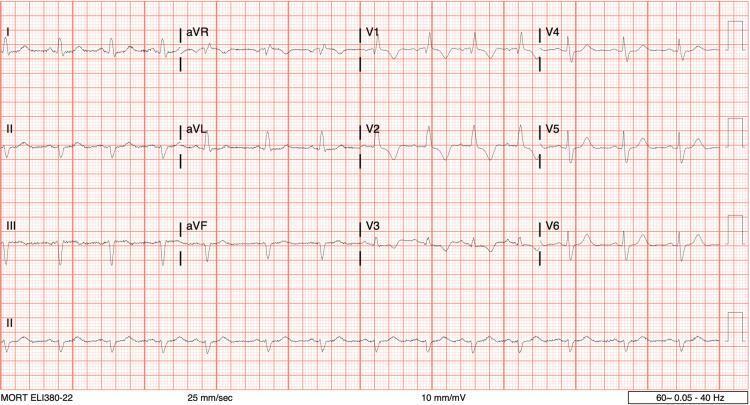
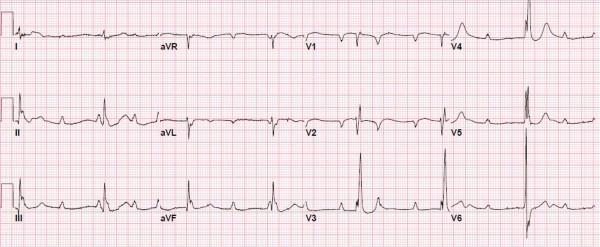
9. Left Ventricular Hypertrophy (LVH)
ECG criteria (any one meets threshold):
| Criterion | Threshold |
|---|---|
| Sokolow-Lyon | S in V1 + R in V5 or V6 ≥35 mm |
| Cornell | R in aVL + S in V3 >28 mm (men) / >20 mm (women) |
| R in aVL | >12 mm alone |
LVH strain pattern: ST depression + T-wave inversion in I, aVL, V5–V6 (discordant repolarization).
Note: Obesity and horizontal cardiac position reduce ECG voltage sensitivity — a normal ECG does not exclude LVH. Echocardiography remains the gold standard.
10. Brugada Pattern
- Type 1 (diagnostic): Coved ST elevation ≥2 mm in V1–V2 with negative T wave
- Type 2 (saddle-back): Less specific
- Associated with sudden cardiac death from VF in structurally normal hearts
- Unmasked by fever, sodium channel blockers, cocaine, hyperkalemia
11. Myocarditis / Takotsubo (STEMI Mimic)
- Diffuse ST elevation (not confined to one vascular territory)
- Inferolateral pattern without coronary occlusion
- Elevated troponin + normal coronaries on angiography
Quick-Reference Summary Table
| ECG Pattern | Key Finding | Rate | QRS Width | Clinical Urgency |
|---|---|---|---|---|
| Sinus tachycardia | Regular, P before every QRS | >100 | Narrow | Investigate cause |
| Sinus bradycardia | Regular, P before every QRS | <60 | Narrow | Symptomatic? Consider pacing |
| Atrial fibrillation | Irregularly irregular, no P waves | Variable | Narrow | Rate/rhythm control, anticoagulate |
| Atrial flutter | Sawtooth F-waves, regular | ~150 (2:1) | Narrow | Rate control, cardioversion |
| 1st degree AV block | PR >200 ms, all P conduct | Normal | Narrow | Usually benign |
| Mobitz II | Fixed PR, sudden dropped QRS | Slow | Wide | Permanent pacemaker |
| Complete heart block | AV dissociation | Slow | Wide | Emergency pacing |
| STEMI | ST elevation + reciprocal changes | Normal/fast | Narrow | Emergency PCI |
| LBBB | Wide QRS, WiLLiaM pattern | Variable | ≥120 ms | New = STEMI equivalent |
| RBBB | Wide QRS, MaRRoW pattern | Variable | ≥120 ms | Often benign |
| VT | Wide-complex tachycardia, AV dissoc. | >150 | >120 ms | Cardioversion/amiodarone |
| VF | Chaotic, no organized complexes | — | — | Immediate defibrillation |
| Torsades de Pointes | Twisting polymorphic VT, long QT | >200 | Wide | Mg²⁺ IV, correct QT |
| LVH | High voltage, strain pattern | Normal | Narrow | Echo confirmation |
| Brugada Type 1 | Coved V1–V2, ≥2 mm | Normal | Normal | ICD consideration |
This is a shared conversation. Sign in to Orris to start your own chat.