Explain common heart disease with ecg changes and ecg diagram of those diseases
Reading File
Finding Sources
Finding Sources
Searching the Web
common heart disease ECG changes diagrams STEMI atrial fibrillation heart block
Finding Sources
Finding Sources
Searching the Web
ECG diagrams atrial fibrillation ventricular tachycardia heart block LBBB images
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Searching the Web
STEMI ECG diagram ST elevation myocardial infarction lead changes image
Loading Image
Loading Image
Loading Image
I now have rich textbook content and multiple ECG diagrams. Let me now generate a comprehensive, well-illustrated answer.
Common Heart Diseases and Their ECG Changes
Understanding the Normal ECG First
A normal ECG has:
- P wave - atrial depolarization
- PR interval - 0.12-0.20 sec (AV nodal conduction)
- QRS complex - ventricular depolarization (<0.12 sec)
- ST segment - isoelectric (on the baseline)
- T wave - ventricular repolarization
- QT interval - total ventricular activity
1. Myocardial Infarction (Heart Attack)
Pathophysiology
Coronary artery occlusion causes three zones: necrosis (center), injury (surrounding), and ischemia (outer). Each zone produces distinct ECG changes.
ECG Changes - Acute STEMI (ST-Elevation MI)
According to Ganong's Review of Medical Physiology, three major membrane abnormalities produce ECG changes:
| Defect in Infarcted Cells | Current Flow | ECG Change |
|---|---|---|
| Rapid repolarization | Out of infarct | ST elevation |
| Decreased resting membrane potential | Into infarct | TQ depression (appears as ST elevation) |
| Delayed depolarization | Out of infarct | ST elevation |
Acute phase (minutes-hours):
- Hyperacute tall, peaked T-waves (earliest sign)
- ST elevation in leads overlying the infarct
- Reciprocal ST depression in opposite leads
Evolving phase (hours-days):
- T-wave inversion
- Pathological Q waves develop (>0.04 sec wide, >25% of R height)
- Q waves = electrically silent scar/necrosis
Old MI:
- Persistent Q waves
- T-wave inversion may normalize
- Loss of R-wave progression ("failure of R-wave progression")
Localizing the Infarct by Leads
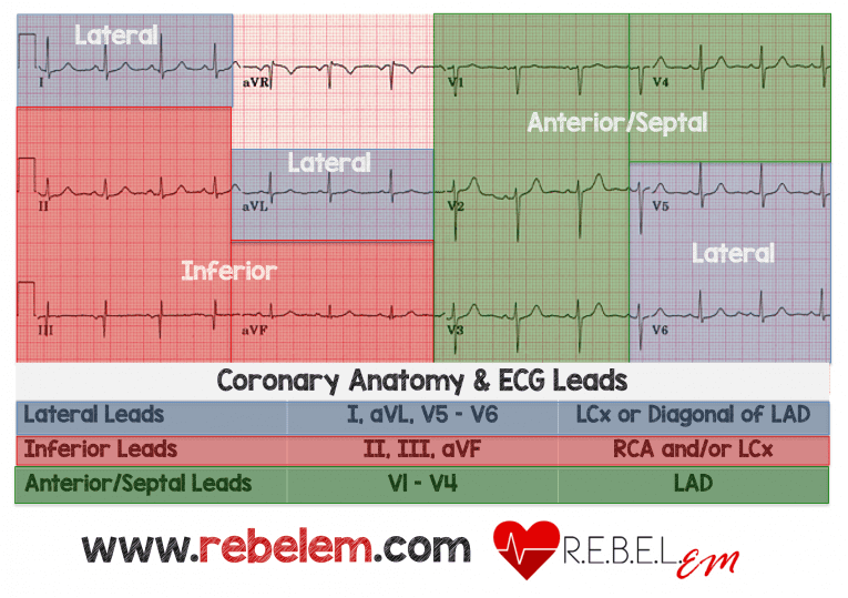
| Territory | Leads with ST Elevation | Artery |
|---|---|---|
| Anterior/Septal | V1-V4 | LAD |
| Lateral | I, aVL, V5-V6 | LCx or LAD diagonal |
| Inferior | II, III, aVF | RCA (or LCx) |
| Posterior | ST depression V1-V4 (mirror image) | RCA/LCx |
STEMI Equivalent Patterns (Advanced)

- Wellens pattern A - Biphasic T-waves in V2-V3 = critical LAD stenosis
- Wellens pattern B - Deep T-wave inversion in V2-V3 = critical LAD stenosis
- De Winter T-wave - Upsloping ST depression + tall T-wave in V1-V6 = LAD occlusion without ST elevation
- Hyperacute T-waves - Broad, bulky disproportionately large T-waves = earliest STEMI sign
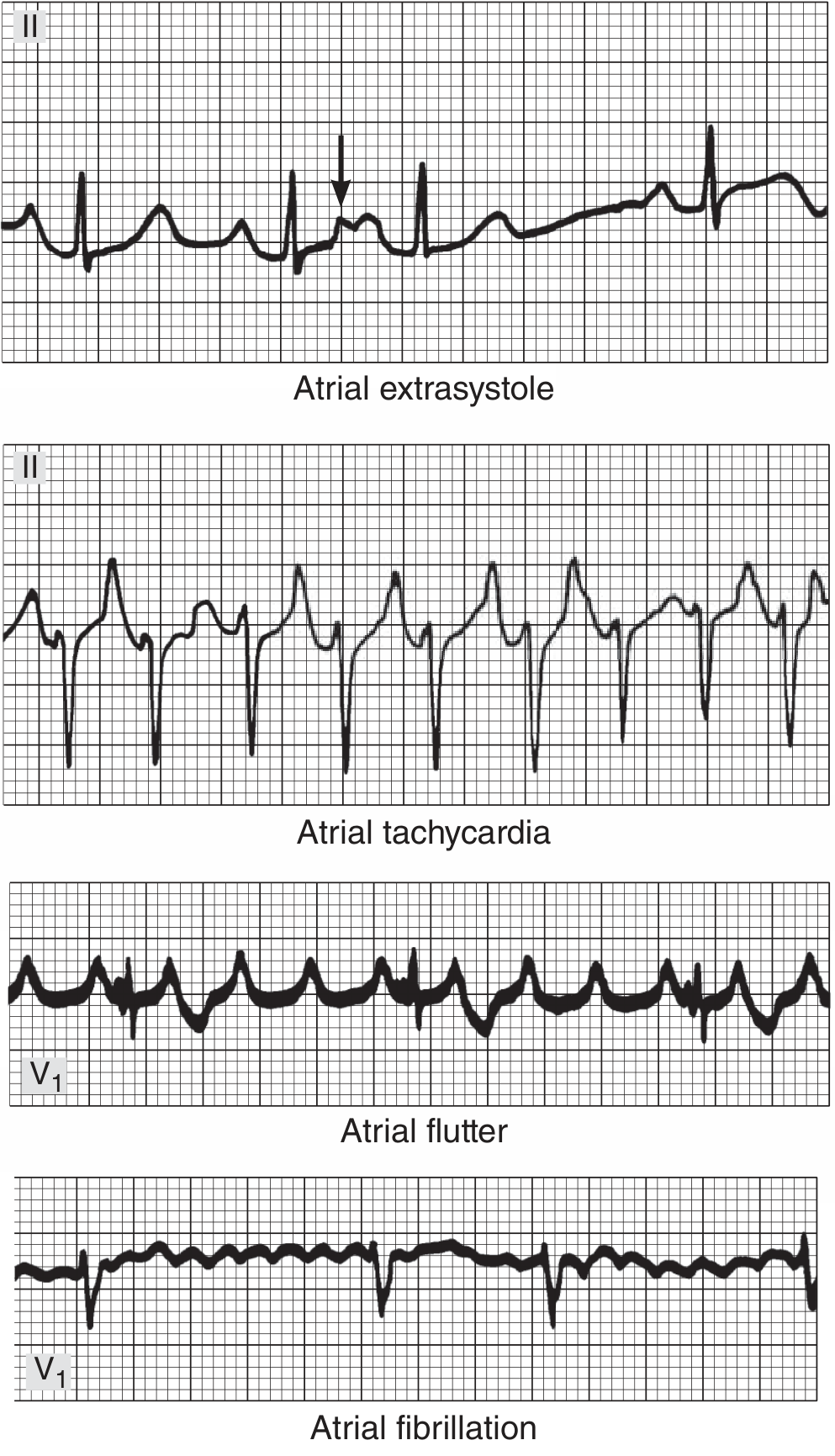
2. Atrial Fibrillation (AF)
Disease
AF is the most common cardiac arrhythmia. The atria beat chaotically at 300-500/min in a disorganized fashion due to multiple circulating reentrant excitation waves. The AV node receives irregular impulses and passes them irregularly to the ventricles.
ECG Changes
| Feature | Finding |
|---|---|
| P waves | Absent - replaced by rapid, irregular fibrillatory (f) waves |
| Baseline | Chaotic, undulating (especially in V1) |
| R-R intervals | Completely irregular ("irregularly irregular") |
| QRS complex | Usually narrow (normal), unless aberrant conduction |
| Rate | Ventricular rate 80-160/min (uncontrolled) |
Key distinguishing feature: No two R-R intervals are the same, and no identifiable P waves precede QRS complexes.
3. Atrial Flutter
Disease
Atrial flutter is a macro-reentrant arrhythmia in the right atrium, typically circling the tricuspid annulus at 250-350/min. The AV node usually conducts at 2:1, giving a ventricular rate of ~150/min.
ECG Changes
| Feature | Finding |
|---|---|
| P waves | "Sawtooth" flutter waves at ~300/min |
| Classic look | Negative sawtooth in II, III, aVF |
| AV conduction | Usually 2:1 (rate ~150), or 3:1, 4:1 |
| QRS | Narrow (normal morphology) |
The sawtooth pattern is most visible in leads II, III, aVF, and V1.
4. Ventricular Tachycardia (VT)
Disease
VT arises from an ectopic ventricular focus firing rapidly. Impulses spread slowly through ventricular muscle (not through the fast His-Purkinje system), producing wide, bizarre QRS complexes. VT can degenerate to ventricular fibrillation, causing sudden cardiac death.
ECG Changes
| Feature | Finding |
|---|---|
| Rate | 100-250/min |
| QRS | Wide (>0.12 sec), bizarre morphology |
| P waves | Present but dissociated from QRS (AV dissociation) |
| Fusion beats | Occasional normal QRS when sinus beat "fuses" with VT |
| Capture beats | Occasional normal narrow QRS (proves AV dissociation) |
| Axis | Usually left axis deviation |
Key diagnostic clues for VT vs SVT with aberrancy:
- AV dissociation (P waves march through at a different rate than QRS) = confirms VT
- Concordance in precordial leads (all QRS pointing same direction) = VT
- QRS width >0.16 sec = VT more likely
5. Ventricular Fibrillation (VF)
Disease
VF is disorganized electrical activity in the ventricles with no effective contraction. It causes cardiac arrest and death within minutes without defibrillation.
ECG Changes
| Feature | Finding |
|---|---|
| QRS | Absent - no recognizable QRS complexes |
| Baseline | Chaotic, irregular oscillations of varying amplitude |
| P waves | Absent |
| Rate | Cannot be determined |
Coarse VF = large amplitude oscillations (more responsive to defibrillation)
Fine VF = small amplitude oscillations (worse prognosis, may resemble asystole)
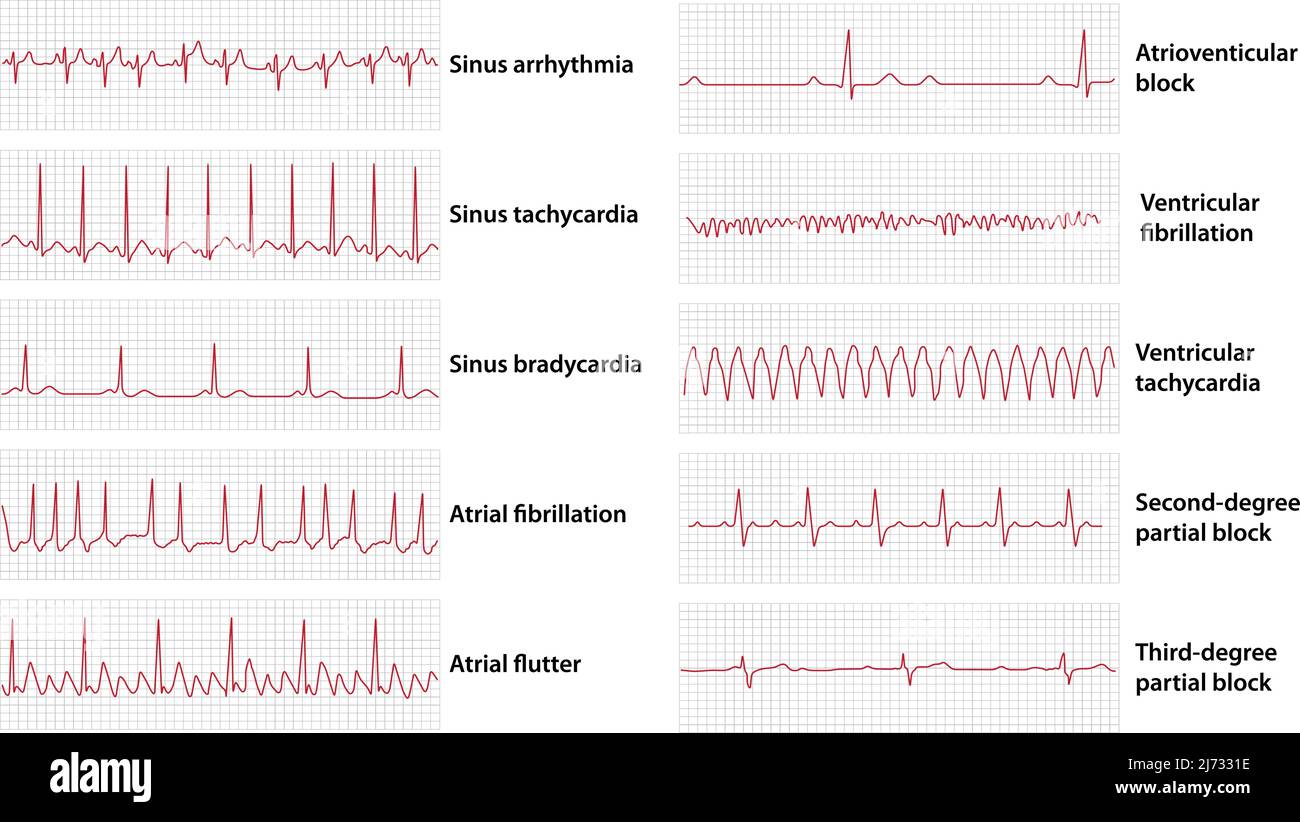
6. AV Heart Blocks
Overview of ECG pattern diagrams:

First-Degree AV Block
| Feature | Finding |
|---|---|
| PR interval | Prolonged >0.20 sec (>5 small squares) |
| All P waves | Conducted (every P followed by QRS) |
| QRS | Normal morphology |
| Significance | Usually benign; can occur in athletes, inferior MI, drugs (digoxin, beta-blockers) |
Second-Degree AV Block - Mobitz Type I (Wenckebach)
| Feature | Finding |
|---|---|
| PR interval | Progressively lengthening each beat |
| Then | A P wave is suddenly not followed by a QRS ("dropped beat") |
| After drop | PR interval resets to normal, cycle repeats |
| QRS | Normal morphology |
| Site of block | AV node |
Second-Degree AV Block - Mobitz Type II
| Feature | Finding |
|---|---|
| PR interval | Fixed and constant |
| Dropped beats | P waves suddenly not conducted without prior PR prolongation |
| QRS | Wide (often with bundle branch block) |
| Significance | More serious - often progresses to complete heart block |
| Site of block | Below the AV node (His-Purkinje) |
Third-Degree (Complete) AV Block
| Feature | Finding |
|---|---|
| P waves | Present at regular atrial rate |
| QRS | Present but at independent, SLOWER rate (30-60/min) |
| Relationship | P waves and QRS have NO fixed relationship (complete AV dissociation) |
| QRS morphology | Wide (junctional escape) or very wide (ventricular escape) |
| Significance | Medical emergency - requires pacing |
7. Bundle Branch Blocks
Right Bundle Branch Block (RBBB)
The right ventricle is activated late, after the left. This causes the characteristic pattern:
| Feature | Finding |
|---|---|
| QRS duration | ≥0.12 sec |
| V1 | RSR' pattern ("M" or "rabbit ears" - broad R') |
| V5-V6, I, aVL | Broad, slurred S-wave |
| Axis | Normal |
| Secondary changes | ST-T changes in V1-V3 |
Causes: Pulmonary embolism (new RBBB), right heart strain, congenital, anterior MI
Left Bundle Branch Block (LBBB)
The left ventricle is activated abnormally via the right bundle then slowly through muscle:
| Feature | Finding |
|---|---|
| QRS duration | ≥0.12 sec |
| V1-V2 | Deep and broad QS or rS complex |
| V5-V6 | Broad, clumsy, positive R-wave (no Q wave in V5-V6) |
| Secondary changes | Discordant ST-T changes (T-wave opposite to QRS main deflection) |
Important: New LBBB with chest pain = STEMI equivalent until proven otherwise
8. Wolff-Parkinson-White (WPW) Syndrome
Disease
An accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting part of the ventricle. This creates a hybrid QRS of fast accessory pathway conduction + slow AV nodal conduction.
ECG Changes
| Feature | Finding |
|---|---|
| PR interval | Short (<0.12 sec) |
| QRS | Widened with a "delta wave" (slurred upstroke at start of QRS) |
| ST-T changes | Secondary (discordant) |
| Arrhythmias | SVT, atrial fibrillation (life-threatening if fast conduction via accessory pathway) |
9. Left Ventricular Hypertrophy (LVH)
Disease
Chronic pressure overload (hypertension, aortic stenosis) causes LV muscle thickening, generating larger electrical forces.
ECG Changes (Sokolow-Lyon criteria)
| Feature | Finding |
|---|---|
| Voltage | S in V1 + R in V5 or V6 ≥35mm |
| Or | R in aVL ≥11mm |
| ST-T changes | "Strain pattern" - downsloping ST depression + T-wave inversion in I, aVL, V5-V6 |
| Axis | Left axis deviation |
| P wave | Broad, notched P in II = left atrial enlargement (often coexists) |
10. Pericarditis
Disease
Inflammation of the pericardium causes ST changes due to subepicardial myocardial irritation - diffuse in nature (unlike MI which is regional).
ECG Changes - Classic Four Stages
| Stage | Timing | ECG Changes |
|---|---|---|
| Stage 1 | Days 1-2 | Diffuse concave ("saddle-shaped") ST elevation in most leads (I, II, aVL, V2-V6); PR depression in same leads |
| Stage 2 | Days 3-7 | ST normalizes; T-waves flatten |
| Stage 3 | Week 2 | T-wave inversions diffusely |
| Stage 4 | Weeks later | ECG normalizes |
Key distinguishing features from MI:
- Concave (saddle-shaped) vs convex (tombstone) ST elevation
- Diffuse in all leads vs regional
- PR depression is unique to pericarditis
- No reciprocal ST depression (unlike MI)
Summary Table
| Condition | Key ECG Feature |
|---|---|
| STEMI | Regional ST elevation + reciprocal depression + Q waves |
| NSTEMI/Unstable Angina | ST depression, T-wave inversion, or no changes |
| Atrial Fibrillation | No P waves, chaotic baseline, irregularly irregular RR |
| Atrial Flutter | Sawtooth flutter waves at 300/min, 2:1 conduction |
| Ventricular Tachycardia | Wide QRS >0.12s, AV dissociation, rate >100 |
| Ventricular Fibrillation | Chaotic baseline, no QRS |
| 1st Degree Heart Block | PR >0.20 sec, all P waves conducted |
| 2nd Degree (Wenckebach) | Progressive PR lengthening then dropped beat |
| 2nd Degree (Mobitz II) | Fixed PR, sudden dropped beats |
| Complete Heart Block | P and QRS independent, bradycardia |
| RBBB | RSR' in V1, broad S in V5-V6 |
| LBBB | QS in V1, broad R in V5-V6, no Q in V5-V6 |
| LVH | High voltage + strain pattern |
| Pericarditis | Diffuse saddle-shaped ST elevation + PR depression |
| WPW | Short PR + delta wave |
Combined ECG Patterns Overview
Sources:
- Ganong's Review of Medical Physiology, 26th Ed., pp. 531-534
- Braunwald's Heart Disease, 2 Vol Set, Chapters 61
- Harrison's Principles of Internal Medicine 22E (2025)
- Goldman-Cecil Medicine - Electrocardiography section
- The Washington Manual of Medical Therapeutics - AV Conduction Disturbances
This is a shared conversation. Sign in to Orris to start your own chat.