30 year old male fell unconsocious after touching high tension wire. He regained consciousness after ten minutes. He is conscious, coherent and obeying commands. He is complaining of back pain
Reading File
Finding Sources
Finding Sources
Searching PubMed
"electrical injury"[MeSH Terms] AND "clinical management"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information to give a thorough, well-structured clinical answer. Let me compile everything.
High-Voltage Electrical Injury - Clinical Assessment & Management
Situation Overview
This is a high-voltage electrical injury (power lines typically carry >11,000 V, far above the 1000 V threshold). The patient has:
- Lost consciousness (LOC) for 10 minutes - now alert, coherent, obeying commands
- Back pain - a red flag symptom in this context
This patient must be treated as a multi-system trauma case until proven otherwise.
Why Back Pain is a Red Flag Here
High-voltage AC current causes tetanic muscular contractions. The powerful paraspinal and truncal muscle contractions can cause:
- Compression fractures of the vertebral bodies (especially thoracic)
- Spinal cord injury from the tetanic contraction or from a fall
- Direct electrical injury to the spinal cord
"Increased risk of compression spine fractures or spinal cord injury due to tetany" - Harriet Lane Handbook
High-voltage DC exposure can also throw the victim, causing blunt traumatic spinal injury from the fall.
Immediate spinal immobilization is mandatory until imaging rules out a fracture.
Immediate Priorities (ABC + C-spine)
| Priority | Action |
|---|---|
| Airway | Assess, secure early if any concern - edema can progress |
| C/T/L/S Spine | Immediate immobilization - do NOT move without imaging |
| Breathing | SpO2, supplemental O2, target SaO2 >92% |
| Circulation | IV access x2, continuous cardiac monitoring, 12-lead ECG |
| Exposure | Full skin exam for entry/exit wounds, burns |
Cardiac Concerns
- Ventricular fibrillation is the most common fatal arrhythmia in horizontal-pathway currents (up to 60% of cases)
- Any dysrhythmia is possible; new-onset atrial fibrillation is the most common arrhythmia seen in survivors
- Overall arrhythmia rate post-electrical injury: up to 15%; most are benign and occur within the first few hours
- The patient had LOC for 10 minutes - this mandates full cardiac evaluation
Action: 12-lead ECG now. Continuous telemetry monitoring for 24 hours minimum (up to 48 hours per Current Surgical Therapy). Treat dysrhythmias per ACLS guidelines.
Investigations to Order
| Test | Rationale |
|---|---|
| 12-lead ECG | Dysrhythmia, ischemia, cardiac injury pattern |
| Serum troponin | Myocardial damage; if elevated, echocardiogram + prolonged monitoring |
| Serum myoglobin | Rhabdomyolysis from muscle destruction |
| Urinalysis + urine myoglobin | Myoglobinuria -> risk of acute kidney injury |
| CBC, BMP (electrolytes, BUN, creatinine) | Baseline renal function, K+ (rises with rhabdo) |
| LFTs + lipase | If abdominal symptoms or suspected intra-abdominal current path |
| Coagulation studies | If significant injury suspected |
| MRI/CT spine | HIGH PRIORITY given back pain - rule out fracture and cord injury |
| CT head | If any focal neuro signs or concern for traumatic brain injury |
| X-rays of injured extremities | If pain, deformity, or bony tenderness |
Fluid Management
High-voltage injuries cause deep tissue destruction and rhabdomyolysis. Fluid requirements are similar to crush injuries and exceed standard burn protocols:
- IV crystalloid to maintain urine output >100 mL/hr in adults
- If myoglobinuria: aggressive IV fluids to flush myoglobin from renal tubules and prevent acute tubular necrosis
- Monitor serum potassium closely - rises with rhabdomyolysis and can trigger fatal arrhythmias
Neurological Assessment
The 10-minute LOC is significant. Perform:
- GCS (currently appears 15 - conscious, coherent, obeying commands)
- Full cranial nerve exam
- Motor and sensory examination of all four limbs
- Assess for evidence of spinal cord injury: weakness, paresthesias, bladder/bowel dysfunction
Note: Patients can develop delayed neuropsychiatric sequelae - arrange neurology follow-up at discharge if admitted.
Wounds
- Identify and document entry and exit wounds (typically entry on the hand/point of contact; exit where grounding occurred)
- High-voltage injuries produce deep tissue destruction that is far more extensive than surface appearance suggests - "iceberg effect"
- Assess extremities for compartment syndrome (pressure monitoring if clinical suspicion)
- Monitor for delayed vascular thrombosis
Disposition
Given this patient has:
- High-voltage exposure (power line)
- Loss of consciousness
- Back pain (possible spinal injury)
Admission is mandatory. Minimum 24-hour telemetry monitoring. Urgent MRI spine. Consider transfer to a burn center if significant burns are found.
Do NOT discharge this patient from the ED without spinal imaging and a period of monitored observation.
Summary of Key Points
- High-voltage injuries are deceptively severe - surface findings underestimate deep injury
- Back pain after electrical LOC = spinal fracture/cord injury until proven otherwise - immobilize now
- 10-minute LOC mandates full cardiac, neurological, and renal workup
- The injury path through the body (entry-to-exit) determines which organs are at risk - assess accordingly
- Rhabdomyolysis, acute kidney injury, and delayed arrhythmias are the main life-threatening complications in survivors
Sources: Rosen's Emergency Medicine, 9th Ed.; Current Surgical Therapy, 14th Ed.; Harriet Lane Handbook, 23rd Ed.; Current Surgical Therapy Table 5 (Critical Care Management of Electric Injury Patient)
X ray spine show wedge compression fracture
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Now I have everything needed for a comprehensive, structured response.
Wedge Compression Fracture - Management in High-Voltage Electrical Injury
This finding confirms what was clinically suspected. The tetanic muscle contractions from high-voltage AC current caused a hyperflexion force on the spine, producing the wedge compression fracture. The back pain was the clinical clue.
Step 1 - Maintain Spinal Immobilization
Do NOT move this patient without full spinal precautions.
- Hard collar + spine board / log-roll precautions
- Thoracolumbosacral orthosis (TLSO) if thoracolumbar level
- All transfers with full spinal precautions until fracture stability and neurological status are clearly defined
Step 2 - Urgent Neurological Assessment (ASIA Score)
This is the most important clinical step right now. The patient is conscious and coherent - a full ASIA (American Spinal Injury Association) classification must be done immediately.
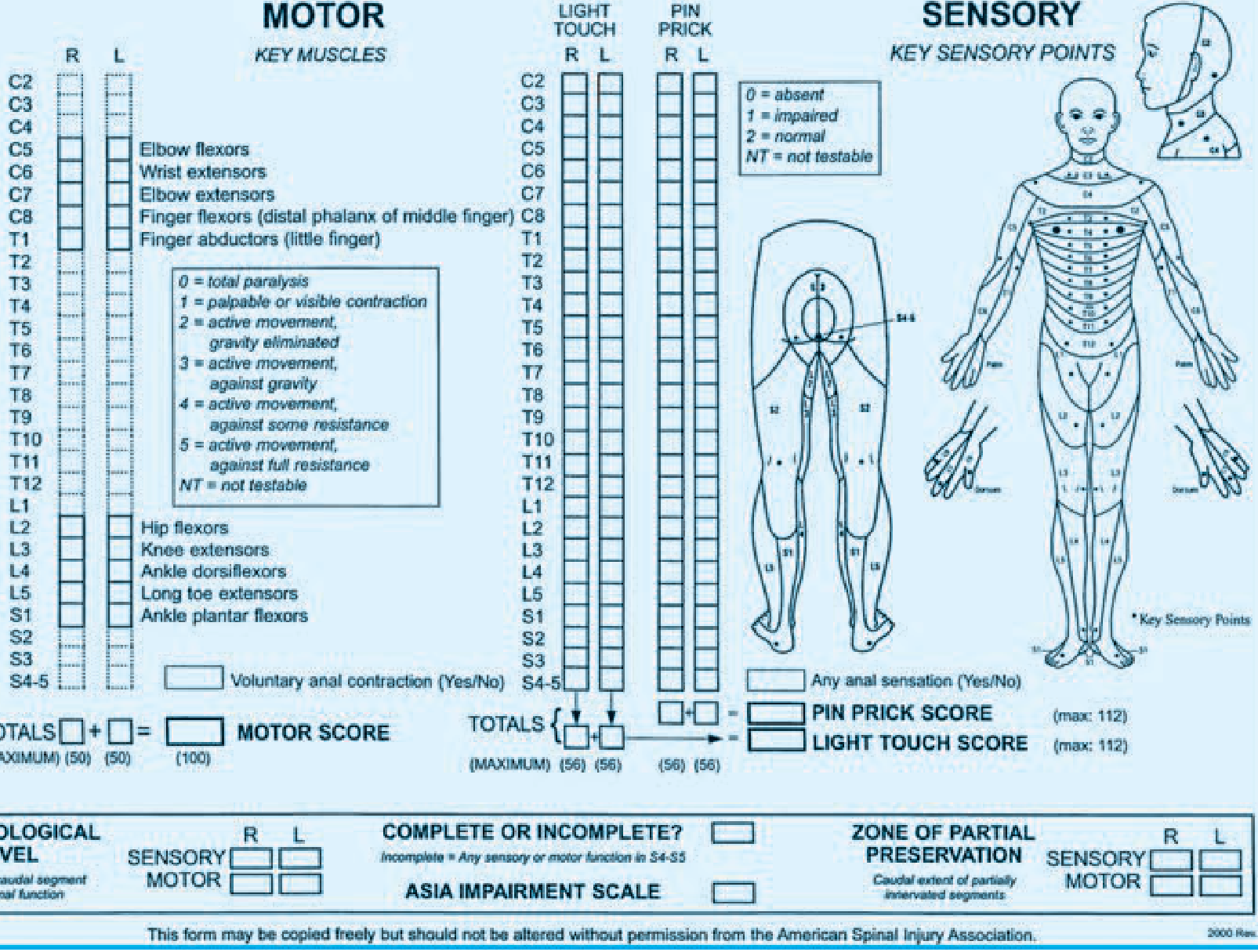
ASIA Standard Neurological Classification - Schwartz's Principles of Surgery, 11th Ed.
Examine systematically:
| Component | What to Test |
|---|---|
| Motor | Key muscles at each level (C5-T1, L2-S1); score each 0-5 |
| Sensory - Light Touch | Test each dermatome bilaterally |
| Sensory - Pin Prick | Test each dermatome bilaterally |
| Sacral function | Voluntary anal contraction (S4-5); perianal sensation |
| Complete vs Incomplete | ANY preserved motor/sensory at S4-S5 = incomplete injury |
ASIA Impairment Scale:
- A - Complete: no motor or sensory function below lesion including S4-5
- B - Sensory incomplete: sensation preserved but no motor below lesion
- C - Motor incomplete: motor preserved below, majority of key muscles <grade 3
- D - Motor incomplete: motor preserved below, majority of key muscles ≥grade 3
- E - Normal motor and sensory function
This patient obeying commands suggests upper limb function is intact. The key question is: are lower limbs affected? Check for weakness in hip flexors (L2), knee extensors (L3), ankle dorsiflexors (L4), toe extensors (L5), ankle plantarflexors (S1).
Step 3 - Imaging
X-ray has confirmed the fracture. Now you need:
MRI Spine (Priority)
- Defines cord compression - is there canal compromise?
- Identifies cord signal change (contusion, edema, hemorrhage)
- Assesses posterior ligamentous complex (PLC) integrity - determines stability
- Rules out multi-level involvement (electrical injury can cause multiple levels)
CT Spine
- Better bony detail than X-ray
- Quantifies degree of vertebral body height loss and retropulsion
- Determines kyphotic angle (Cobb angle)
- Helps classify fracture stability
Key radiological questions to answer:
- What level is the fracture? (Most electrical compression fractures occur in the mid-thoracic or thoracolumbar junction T12-L1)
- What is the degree of anterior wedging? (>50% height loss = unstable)
- Is there retropulsion into the spinal canal?
- Is the posterior ligamentous complex intact?
- Are there multiple levels involved?
Step 4 - Fracture Classification and Stability
Using the Denis Three-Column Model:
| Column | Components | Wedge Compression |
|---|---|---|
| Anterior | Anterior longitudinal ligament + anterior 2/3 vertebral body | Disrupted (compressed) |
| Middle | Posterior 1/3 vertebral body + posterior longitudinal ligament | Usually intact in simple wedge |
| Posterior | Posterior bony arch + posterior ligamentous complex | Usually intact |
A simple wedge compression fracture (anterior column only, <50% height loss, no retropulsion, intact middle and posterior columns) is generally stable. However, in this electrical injury context - where tetanic forces are enormous and the mechanism is violent - do not assume stability without CT/MRI confirmation.
Unstable fracture features requiring surgical consideration:
-
50% loss of vertebral body height
-
30 degrees kyphotic angulation
- Retropulsion into spinal canal
- Posterior ligamentous disruption
- Neurological deficit
Step 5 - Management Plan
If NEUROLOGICALLY INTACT + Stable Fracture (Most Likely in This Patient)
The patient is conscious and obeying commands, suggesting preserved motor function:
- Conservative management: TLSO brace immobilization
- Bed rest initially, then gradual mobilization with brace
- Analgesia: IV morphine or fentanyl acutely; avoid NSAIDs in the short term given risk of renal impairment from myoglobinuria
- Physiotherapy - early mobilization once stability confirmed
- Neurosurgical / orthopaedic spine consult for definitive management plan
If NEUROLOGICAL DEFICIT PRESENT or Unstable Fracture
- Neurosurgical emergency - urgent spine surgery consultation
- Timing: Surgery within 24 hours is associated with better neurological outcomes (higher odds of 2-point improvement in ASIA grade at 6 months) - Schwartz's Principles of Surgery
- Goals of surgery: Decompression of spinal cord/nerve roots + stabilization
- Maintain MAP >85 mmHg for 7 days post-injury to optimise spinal cord perfusion
Steroids (Methylprednisolone) - Controversial
High-dose methylprednisolone (30 mg/kg bolus then 5.4 mg/kg/hr infusion) has been studied in acute SCI:
- NASCIS II/III showed modest benefit if given within 8 hours of injury
- Benefits were only in post-hoc analyses; associated with increased rates of pneumonia, sepsis, poor wound healing
- A recent Cochrane review showed trend towards complications
- Current consensus: NOT routinely recommended; may be considered in selected incomplete injuries after shared decision-making with neurosurgery
Step 6 - Continue All Electrical Injury Monitoring in Parallel
The spinal fracture does not replace the systemic electrical injury workup - both must run simultaneously:
| System | Action |
|---|---|
| Cardiac | Continuous telemetry x24h, serial troponins |
| Renal | Hourly urine output, urine myoglobin, serial creatinine |
| IV fluids | Maintain UO >100 mL/hr (rhabdomyolysis protection) |
| Electrolytes | K+ monitoring (rhabdomyolysis raises K+) |
| Burns | Reassess entry/exit wounds, compartment syndrome monitoring |
| Analgesia | Adequate pain control (aids breathing, prevents splinting and atelectasis) |
Disposition
This patient requires:
- ICU or high-dependency admission (electrical + spinal injury)
- Neurosurgical consultation (urgent if any neurological deficit)
- Orthopedic spine consultation
- Full multidisciplinary team: Emergency medicine, Neurosurgery, Orthopedics, Burns surgery (if burns), Nephrology (if AKI develops)
- Transfer to spinal cord injury center once medically stabilized if significant neurological deficit is found
Summary of Priorities
- Full ASIA neurological examination now - defines urgency of surgery
- MRI spine urgently - cord compression? PLC intact? Canal compromise?
- CT spine - bony detail, Cobb angle, retropulsion
- Spinal immobilization until stability confirmed
- Neurosurgical/spine consult - surgery within 24h if neuro deficit
- Continue systemic electrical injury workup - cardiac monitoring, rhabdomyolysis management
- Adequate analgesia without compromising neurological monitoring
Sources: Schwartz's Principles of Surgery, 11th Ed.; Rosen's Emergency Medicine, 9th Ed.; Harriet Lane Handbook, 23rd Ed.; Current Surgical Therapy, 14th Ed.
Serum myoglobin or creatinine kinase
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
That's the definitive answer from the Tietz Textbook of Laboratory Medicine. Here is the complete response:
Serum Myoglobin vs Creatine Kinase (CK) - Which to Use?
Short Answer: Serum CK is superior
"Evidence that rhabdomyolysis has occurred is better provided by an increase in serum creatine kinase activity not attributable to a cardiac source. There is no strong evidence demonstrating that urinary myoglobin measurement provides useful prognostic information in this setting."
- Tietz Textbook of Laboratory Medicine, 7th Ed.
"Serum creatine kinase (CK) is cleared much more slowly, so measurement of serum CK levels is a more sensitive test."
- Rosen's Emergency Medicine, 9th Ed.
Why CK is Better Than Myoglobin
| Property | Serum Myoglobin | Serum CK |
|---|---|---|
| Molecular weight | Small (17.8 kDa) | Larger |
| Clearance | Rapidly cleared from serum (half-life ~1-3 hrs) | Slowly cleared (half-life ~36-48 hrs) |
| Sensitivity | Lower - may already be undetectable at presentation | Higher - remains elevated for days |
| Specificity for muscle | Present in cardiac + skeletal muscle | CK-MM isoform is skeletal-muscle specific |
| Prognostic value | No strong evidence for prognostic use | Correlates with degree of muscle destruction |
| Urine dipstick | False negatives and positives common | Not applicable |
| Timing of peak | 6-12 hours, then falls rapidly | 24-72 hours, sustained elevation |
The Problem with Myoglobin
Myoglobin is a small protein. After rhabdomyolysis:
- It floods the plasma
- Saturates renal tubular reabsorption
- Gets filtered and excreted into urine
- Is directly nephrotoxic - precipitates in renal tubules causing acute tubular necrosis
- But it is cleared from serum so rapidly that by the time the patient reaches hospital, serum levels may already be falling or undetectable - even if significant muscle destruction occurred
Urine dipstick for blood will be positive (myoglobin cross-reacts with the hemoglobin reagent) but this gives up to 50% false negative rate in rhabdomyolysis because myoglobin may already have been cleared from the urine.
What to Order in This Patient
Order BOTH, but rely on CK as the primary marker:
-
Serum CK (total + isoforms)
- The primary marker for diagnosis and monitoring
- CK-MM elevated = skeletal muscle (rhabdomyolysis)
- CK-MB elevated = cardiac muscle injury (also relevant here given electrical injury)
- Serial measurements every 6-12 hours
- CK >5000 U/L = significant rhabdomyolysis; >10,000 U/L = high risk for AKI
-
Serum myoglobin - Order on arrival; if already low it does NOT rule out rhabdomyolysis
-
Urine myoglobin / urine dipstick - Brown/red urine with positive dipstick for blood but no RBCs on microscopy = myoglobinuria; this is a clinical bedside clue
-
Serum creatinine + BUN - Monitor for developing AKI
-
Urine output - The most important monitoring parameter; maintain >100 mL/hr with IV fluids
Practical Takeaway
In this patient who touched a high-tension wire and has confirmed muscle injury (electrical + possibly from spinal fracture immobility) - serum CK is the test to follow serially. It will tell you:
- How much muscle has been destroyed
- Whether the rhabdomyolysis is improving or worsening
- When it is safe to reduce IV fluid rate
Myoglobin is gone from the serum too fast to be a reliable monitor. CK stays elevated and guides your fluid management.
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed.; Rosen's Emergency Medicine, 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.