Treatment for Premature ejaculation with Erectile Dysfunction
Reading File
Finding Sources
Finding Sources
Searching PubMed
"premature ejaculation" AND "erectile dysfunction" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I have excellent, comprehensive data. Now I'll compile the full answer.
Treatment of Premature Ejaculation (PE) with Comorbid Erectile Dysfunction (ED)
Understanding the Comorbidity
As many as 50% of men with ED also experience PE. The mechanism works in two ways: men with ED may need higher stimulation to achieve erection, or they intentionally "rush" intercourse to prevent detumescence of a partial erection - both resulting in brief ejaculatory latency. High performance anxiety from the underlying ED compounds the problem further.
Important diagnostic caveat: 33.3% of potent men with PE falsely score positive on the SHIM (Sexual Health Inventory for Men / IIEF) questionnaire for ED - particularly on questions Q3 and Q4 - because they confuse the ability to maintain erections before versus after ejaculation. Always confirm true ED before treating it as comorbid.
- Campbell Walsh Wein Urology, p. 2080
Management Algorithm
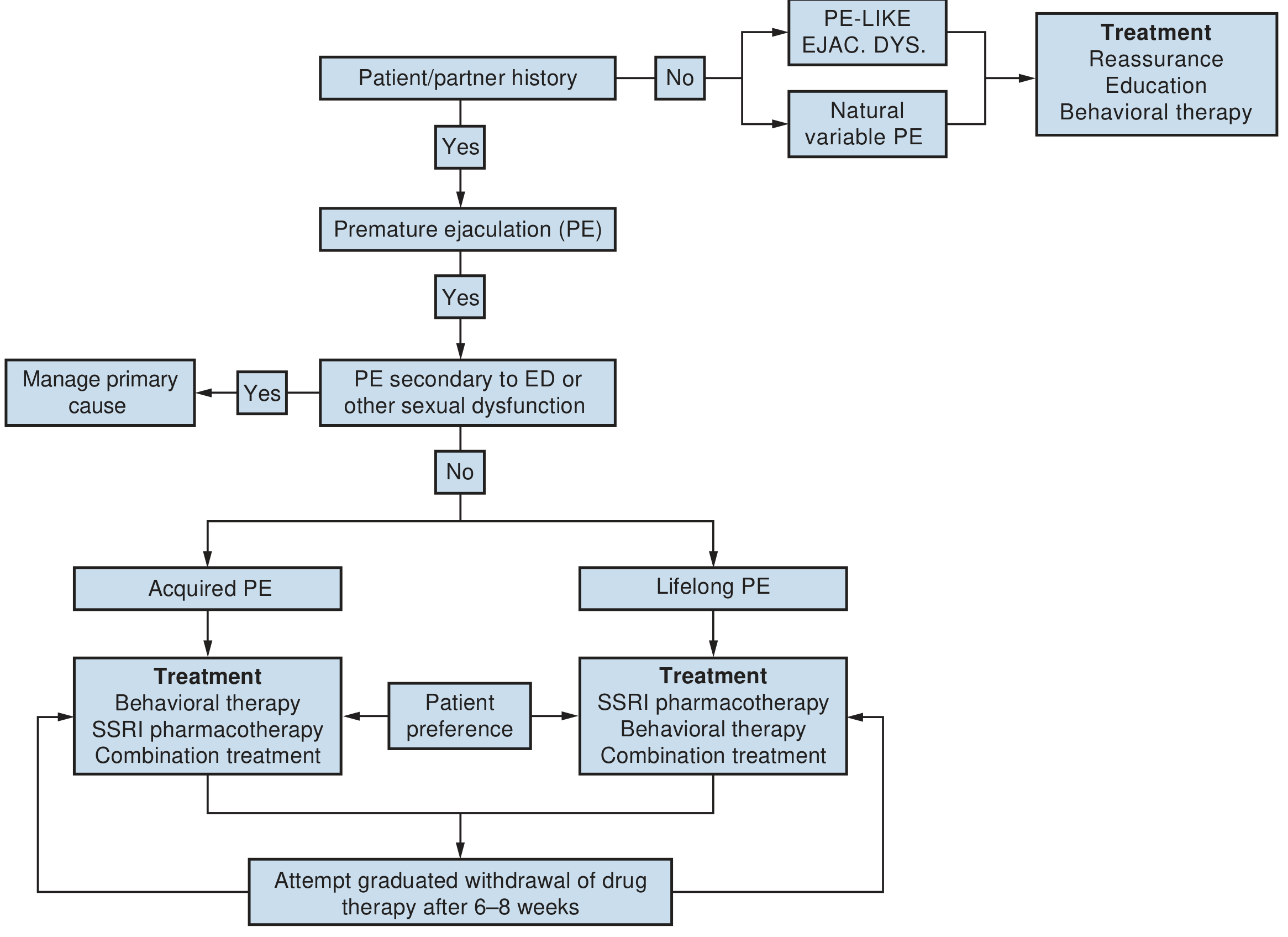
Fig. 71.3 - Campbell Walsh Wein Urology
Key decision point for the PE + ED patient: If PE is clearly secondary to ED, the first step is to manage the ED as the primary cause. Once ED is treated (e.g., with PDE5 inhibitors), PE may resolve on its own. If PE persists despite adequate ED management, add specific PE pharmacotherapy.
Step 1: Treat the Underlying ED First (When PE is Secondary to ED)
For acquired PE secondary to ED:
- PDE5 inhibitors (sildenafil, tadalafil, vardenafil) - these address the ED, which in turn reduces performance anxiety and the "rushing" behavior that causes PE
- Even when PE is not purely secondary, PDE5Is still have independent benefit on PE: they reduce performance anxiety, delay the ejaculatory reflex by increasing smooth muscle relaxation and nitric oxide tone, and improve ejaculatory control
- PDE5I drugs show efficacy for PE even in men without objective ED, likely via central and peripheral pathways
Step 2: Pharmacologic Treatment of PE
SSRIs and TCAs (First-Line for PE)
SSRIs block axonal serotonin reuptake, enhancing 5-HT neurotransmission at postsynaptic receptors - this directly inhibits the ejaculatory reflex.
| Drug | Dosing | IELT Fold-Increase | Notes |
|---|---|---|---|
| Dapoxetine 30-60 mg | On-demand, 1-2 hrs before sex | 2.5-3.0x | Only SSRI approved for PE (>50 countries, not FDA approved); safe with PDE5Is |
| Paroxetine 20 mg | Daily (off-label) | Highest among SSRIs (~22x vs tramadol's 5x) | Best delay effect |
| Sertraline 50 mg | Daily or on-demand (off-label) | Moderate | Good tolerability |
| Fluoxetine 20 mg | Daily (off-label) | Moderate | Long half-life |
| Clomipramine 15-25 mg | On-demand or daily (off-label) | Moderate-good | TCA; anticholinergic side effects |
In men with PE + comorbid ED treated with PDE5Is: Dapoxetine was shown in RCTs to be equally effective and well-tolerated as in men without ED - no dose adjustment needed. No drug-drug interactions between dapoxetine and PDE5 inhibitors have been reported.
- Campbell Walsh Wein Urology, p. 2083-2086
Combination: SSRI + PDE5 Inhibitor
This is the key combination strategy for PE + ED:
- Adding a PDE5 inhibitor to an SSRI produces better prolongation of ejaculatory latency than SSRI alone (Goldman-Cecil Medicine)
- The PDE5I treats the underlying ED, reduces performance anxiety, and appears to independently delay ejaculation
- The SSRI (especially dapoxetine) provides direct ejaculatory inhibition
- Multiple studies confirm superior outcomes with combination therapy vs. monotherapy in this population
Topical Local Anesthetics
- Lidocaine/prilocaine cream, gel, or spray (e.g., EMLA cream, lidocaine 2.5% + prilocaine 2.5%)
- Applied to the glans penis 20-30 minutes before intercourse, wiped off before penetration
- Inhibit the spinal reflex arc responsible for ejaculation by reducing glans sensitivity
- Caution: May cause penile hypoanesthesia and can be transferred vaginally causing female partner numbness/anorgasmia unless a condom is used
- Useful alternative when SSRIs are contraindicated or not tolerated
- Campbell Walsh Wein Urology, p. 2086
Tramadol (On-Demand, Off-Label)
- Centrally-acting synthetic opioid analgesic; delays ejaculation via μ-opioid binding and weak SNRI activity
- IELT increase ~2.49x in double-blind trials (inferior to paroxetine: 22x vs 5x for tramadol)
- Reserve as a second-line option given modest efficacy and opioid dependence risk
- Campbell Walsh Wein Urology, p. 2087
Step 3: Psychosexual and Behavioral Therapy
All men with PE + ED should receive psychosexual education and therapy - this is especially important in this combined population:
- Behavioral techniques: Stop-start method (Semans), pause-squeeze technique (Masters and Johnson) - teach men to recognize pre-ejaculatory sensations and voluntarily delay
- Cognitive-behavioral therapy (CBT): Addresses performance anxiety, rigid sexual scripts, avoidance behaviors, and partner relationship issues
- Goals include: improving ejaculatory control, reducing anxiety, improving self-confidence, and enhancing couple communication
- Partner involvement is strongly recommended - a cooperative partner enhances confidence, self-esteem, and sense of control
In PE + ED specifically: Combination of medication + psychotherapy is particularly useful because the psychosocial burden of both conditions compounds each other. Once confidence and control improve, gradual withdrawal of medication can be attempted (after 6-8 weeks per the algorithm).
- Campbell Walsh Wein Urology, p. 2085-2086
Step 4: Treat Underlying Causes of Acquired PE
For acquired PE (where PE developed after a period of normal ejaculatory function), always assess and treat reversible causes:
| Cause | Treatment |
|---|---|
| Erectile dysfunction | PDE5 inhibitors (first priority) |
| Chronic prostatitis / CPPS | Antibiotics if bacterial; symptom management |
| Hyperthyroidism | Thyroid normalization (50% prevalence of PE in hyperthyroid men dropped to 15% after treatment) |
| Performance anxiety | Psychosexual CBT |
| Relationship problems | Couples therapy |
Emerging and Investigational Therapies
- Oxytocin receptor antagonists (e.g., IX-01): Phase IIA trial showed 3.6x IELT increase (vs 1.8x placebo); promising CNS-penetrating agent under development - Goldman-Cecil Medicine, p. 879; Campbell Walsh Wein, p. 2089
- Botulinum toxin-A injection: 2025 meta-analysis (PMID: 40445933) supports efficacy and safety as a PE treatment option
- Modafinil: Preclinical data suggest ejaculation delay via serotonergic/dopaminergic pathways; not yet in routine clinical use
Key Points Summary
- First, confirm true comorbid ED - rule out false-positive SHIM scores from PE patients
- If PE is secondary to ED, treat ED first with PDE5Is - PE may resolve
- SSRI + PDE5 inhibitor combination is the pharmacologic mainstay for true PE + ED comorbidity
- Dapoxetine is the preferred on-demand SSRI (safe with PDE5Is, effective in this population)
- Topical anesthetics are useful alternatives when systemic therapy is not preferred
- Psychosexual therapy must accompany pharmacotherapy - especially in acquired PE with performance anxiety
- Treat reversible causes (prostatitis, hyperthyroidism) in acquired PE
Sources:
- Campbell Walsh Wein Urology, pp. 2080-2089
- Goldman-Cecil Medicine, p. 879
Recent evidence note: A 2025 meta-analysis (PMID 41031773) confirmed that dapoxetine + PDE5I combination is superior to dapoxetine monotherapy for PE. A 2025 meta-analysis on botulinum toxin-A (PMID 40445933) also supports its emerging role. These are consistent with and reinforce the textbook recommendations above.
Desmopressin nasal spray, age group and dose . Brands in india
Finding Sources
Searching the Web
desmopressin nasal spray brands India dose age group
Reading File
Reading File
Searching the Web
desmopressin nasal spray brand names India minirin octim nocutil 2025
Searching the Web
desmopressin nasal spray available brands India pharmacy DDAVP minirin nocutil
I now have comprehensive data. Here is the complete answer:
Desmopressin Nasal Spray - Indications, Age Groups, Doses & Indian Brands
Formulation
- Concentration: 0.01% w/v (0.1 mg/mL = 10 mcg per 0.1 mL spray)
- Delivery: Each pump spray delivers 10 mcg per actuation
- Pack size: Typically 5 mL bottle = 50 sprays
- Nasal bioavailability: 3-4% (intranasal is ~10-40x more potent than oral tablets)
- Katzung's Basic & Clinical Pharmacology, 16th Ed.
Indications
| Indication | Formulation Used |
|---|---|
| Central (Cranial) Diabetes Insipidus | Standard 0.01% (10 mcg/spray) |
| Nocturnal Enuresis (bedwetting) | Standard 0.01% (10 mcg/spray) |
| Hemophilia A / von Willebrand Disease (Type I) | High-strength 1.5 mg/mL (150 mcg/spray) - Stimate/Octim |
| Nocturia (nocturnal polyuria in adults) | Low-dose nasal spray |
Dosing by Age Group
1. Central Diabetes Insipidus
| Age Group | Dose | Frequency |
|---|---|---|
| Infants < 3 months | Not established / not recommended | - |
| Children 3 months - 12 years | 5-30 mcg/day (0.05-0.3 mL) | Single dose or divided into 2 doses |
| Children ≥ 4 years (newer FDA guidance) | Start 10 mcg once daily; titrate up to 30 mcg/day | Once daily or divided |
| Adults | 10-40 mcg/day (1-4 sprays) | Single dose or divided into 2-3 doses; most adults need 20 mcg/day in 2 divided doses |
| Elderly | More sensitive; use lower adult doses | Monitor for hyponatremia |
The morning and evening doses should be adjusted separately for adequate diurnal rhythm of water turnover. About 1/3 of patients can be controlled by a single daily dose.
2. Nocturnal Enuresis (Bedwetting)
| Age Group | Dose | Timing |
|---|---|---|
| Children ≥ 6 years | 20-40 mcg intranasally | At bedtime |
| Adults | 20-40 mcg | At bedtime |
Fluid restriction is mandatory after the evening dose - restrict fluids 1 hour before and 8 hours after administration to prevent hyponatremia/water intoxication. Note: Many guidelines now prefer oral desmopressin (0.2-0.4 mg tablet or melt) over nasal spray for nocturnal enuresis due to more predictable absorption.
3. Hemophilia A / von Willebrand Disease (High-Strength Spray - 1.5 mg/mL)
| Patient | Dose |
|---|---|
| < 2 years | Not recommended |
| ≥ 2 years, < 50 kg | 150 mcg (1 spray into one nostril) |
| ≥ 2 years, ≥ 50 kg | 300 mcg (1 spray into each nostril = 2 sprays total) |
- Tintinalli's Emergency Medicine; Campbell Walsh Wein Urology
Key Prescribing Notes
- Fluid restriction is mandatory in all age groups to avoid dilutional hyponatremia and water intoxication - this is especially dangerous in young children and elderly
- The nasal spray pump delivers only multiples of 10 mcg (0.1 mL); for doses < 10 mcg, a calibrated rhinal tube must be used
- Efficacy may be reduced by nasal congestion - consider switching to oral/parenteral route if congested
- Re-prime the pump if not used for > 1 week
- Storage: Refrigerate at 2-8°C; stable at room temperature (≤ 22°C) for up to 3 weeks during travel
Brands Available in India
| Brand Name | Manufacturer | Notes |
|---|---|---|
| Minirin | Ferring Pharmaceuticals Pvt Ltd (Mumbai) | Originator brand; most widely used; 0.1 mg/mL nasal spray; ₹499-₹2520 |
| D-Pressin / Dpressin | United Biotech Pvt Ltd (New Delhi) | 0.1 mg/mL; 5 mL spray; ₹1,380-₹1,695; available at Apollo Pharmacy |
| Adiuretin | Sun Pharmaceutical Industries Ltd | 2 variants; ₹394-₹1,169 |
| D Void / D Viod | Sun Pharmaceutical Industries Ltd | ₹973-₹1,012 |
| Repressin | Adexa Pharma Private Ltd | ₹1,350 |
| Enurex | Oriental Pharma | ₹356 |
| Dossmirin | Dossmegt Pharmaceuticals | 0.01% w/v intranasal solution; ₹800 |
| Canurin Nasal Spray | RMPL Pharma LLP | ₹1,402 |
| Dessin | Chemo Healthcare Pvt Ltd | ₹506-₹1,209 |
Note: The high-strength Octim/Octostim nasal spray (1.5 mg/mL) used for hemophilia was subject to a global voluntary recall by Ferring Pharmaceuticals (initiated 2020, announced March 2025) due to packaging tightness issues. Confirm current availability with your supplier before prescribing for coagulation indications.
Summary Table
| Parameter | Detail |
|---|---|
| Concentration (standard) | 10 mcg per spray (0.01% w/v) |
| Minimum age (DI) | 3 months (titrated carefully); ≥ 4 years per newer FDA guidance |
| Minimum age (enuresis) | ≥ 6 years |
| Minimum age (hemophilia nasal) | ≥ 2 years |
| Adult dose (DI) | 10-40 mcg/day in 1-3 divided doses |
| Child dose (DI, 3m-12y) | 5-30 mcg/day |
| Enuresis dose | 20-40 mcg at bedtime |
| Key risk | Hyponatremia / water intoxication - always restrict fluids |
Desmopressin nasal spray, age group and dose . Brands in India
This was just covered in detail in our previous exchange. Here is the complete answer again for reference:
Desmopressin Nasal Spray - Indications, Age Groups, Doses & Indian Brands
Formulation
- Concentration: 0.01% w/v (0.1 mg/mL = 10 mcg per 0.1 mL spray)
- Delivery: Each pump actuation = 10 mcg
- Pack size: 5 mL bottle = 50 sprays
- Nasal bioavailability: 3-4% (intranasal is ~10-40x more potent than oral tablets)
Indications & Dosing by Age Group
1. Central (Cranial) Diabetes Insipidus
| Age Group | Dose | Schedule |
|---|---|---|
| < 3 months | Not established | - |
| 3 months - 12 years | 5-30 mcg/day | Single or 2 divided doses |
| ≥ 4 years (newer FDA guidance) | Start 10 mcg once daily; titrate up to 30 mcg/day | Once daily or divided |
| Adults | 10-40 mcg/day | 2-3 divided doses; most need 20 mcg/day in 2 doses |
| Elderly | Start at lower adult dose | Higher risk of hyponatremia; monitor closely |
Morning and evening doses adjusted separately for adequate diurnal rhythm. ~1/3 of patients can be managed with a single daily dose.
2. Nocturnal Enuresis (Bedwetting)
| Age Group | Dose | Timing |
|---|---|---|
| Children ≥ 6 years | 20-40 mcg | Bedtime |
| Adults | 20-40 mcg | Bedtime |
Mandatory: Restrict fluids 1 hour before and 8 hours after the bedtime dose to prevent hyponatremia/water intoxication. Many current guidelines prefer oral desmopressin (tablet/melt) over nasal spray for enuresis due to more predictable absorption.
3. Hemophilia A / von Willebrand Disease Type I
Uses the high-strength formulation: 1.5 mg/mL (150 mcg per spray) - not the standard 0.01% spray.
| Patient | Dose |
|---|---|
| < 2 years | Not recommended |
| ≥ 2 years, weight < 50 kg | 150 mcg - 1 spray into one nostril |
| ≥ 2 years, weight ≥ 50 kg | 300 mcg - 1 spray into each nostril (total 2 sprays) |
Key Prescribing Points
- Pump delivers only multiples of 10 mcg - for doses < 10 mcg, use a calibrated rhinal tube
- Reduced efficacy during nasal congestion - switch to oral/SC route when congested
- Storage: Refrigerate 2-8°C; stable at room temperature (≤ 22°C) for up to 3 weeks while travelling
- Re-prime pump if unused for > 1 week
- Chief risk: dilutional hyponatremia and water intoxication - especially dangerous in young children and the elderly
Brands Available in India
| Brand | Manufacturer | Approx. Price |
|---|---|---|
| Minirin | Ferring Pharmaceuticals Pvt Ltd, Mumbai | ₹499 - ₹2,520 |
| D-Pressin / Dpressin | United Biotech Pvt Ltd, New Delhi | ₹1,380 - ₹1,695 |
| Adiuretin | Sun Pharmaceutical Industries Ltd | ₹394 - ₹1,169 |
| D Void | Sun Pharmaceutical Industries Ltd | ₹973 - ₹1,012 |
| Repressin | Adexa Pharma Pvt Ltd | ₹1,350 |
| Enurex | Oriental Pharma | ₹356 |
| Dossmirin | Dossmegt Pharmaceuticals | ₹800 |
| Canurin | RMPL Pharma LLP | ₹1,402 |
| Dessin | Chemo Healthcare Pvt Ltd | ₹506 - ₹1,209 |
Important note on high-strength spray (Octim/Octostim 1.5 mg/mL): Ferring Pharmaceuticals issued a global voluntary recall of this product in 2025 due to a packaging tightness issue. Verify current availability before prescribing for hemophilia/vWD indications.
Quick Reference Summary
| Parameter | Value |
|---|---|
| Standard concentration | 10 mcg per spray |
| Minimum age - Diabetes Insipidus | 3 months (with caution) |
| Minimum age - Enuresis | 6 years |
| Minimum age - Hemophilia (nasal) | 2 years |
| Adult dose (DI) | 10-40 mcg/day |
| Child dose (DI, 3m-12y) | 5-30 mcg/day |
| Enuresis dose | 20-40 mcg at bedtime |
| Critical safety concern | Hyponatremia - always restrict fluid intake |
This is a shared conversation. Sign in to Orris to start your own chat.