Early a2 late p2
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
"Early A2, Late P2" describes reversed (paradoxical) splitting of S2 — where A2 occurs before P2 in a pathologically delayed sequence, and the split behaves paradoxically with respiration.
Reversed (Paradoxical) Splitting of S2
What It Means
In normal physiology, A2 always precedes P2, but by such a small interval during expiration (<30 ms) that S2 is heard as a single sound. On inspiration, P2 is delayed further (more RV filling → longer RV ejection), producing audible physiologic splitting.
In reversed splitting, there is a pathologic delay in A2 (not P2). This causes:
- P2 to precede A2 — the order is reversed
- S2 is split on expiration (because P2 and the delayed A2 are farther apart)
- S2 becomes single on inspiration (because normal inspiratory delay of P2 now brings it toward A2, narrowing the gap)
This is exactly what "early A2, late P2" means in context — the term is sometimes used loosely to describe the situation where A2 arrives earlier than expected relative to P2, i.e., the aortic valve closes prematurely or the pulmonic closes late, producing audible splitting where P2 follows A2 by a wide interval.
Causes of Reversed / Wide Paradoxical Splitting
| Mechanism | Examples |
|---|---|
| Delayed LV activation (most common) | Left bundle branch block (LBBB) |
| RV pacing | Promotes delayed LV activation, same effect as LBBB |
| Increased LV afterload / prolonged LV ejection | Severe aortic stenosis, hypertrophic obstructive cardiomyopathy (HOCM) |
| LV dysfunction | Prolonged LV ejection time >300 ms |
In severe AS, A2 is often absent or diminished, so paradoxical splitting is rarely heard despite the mechanism. HOCM is actually the more common clinical cause in practice. — Fuster and Hurst's The Heart, 15th Ed.
Wide Physiologic Splitting ("Early A2, Late P2" — Normal Order, Exaggerated)
If the phrase is used in the normal context (A2 still precedes P2, but the interval is exaggerated):
| Mechanism | Examples |
|---|---|
| Delayed P2 (prolonged RV ejection) | Right bundle branch block (RBBB), pulmonary hypertension, pulmonary stenosis |
| Early A2 (shortened LV ejection) | Severe mitral regurgitation (MR), VSD — rapid LV emptying → early aortic closure |
In severe MR, large regurgitant flow into the LA shortens the LV ejection period → A2 occurs early → wide gap to P2 → audible splitting even on expiration. This is wide physiologic (not reversed) splitting.
Diagram
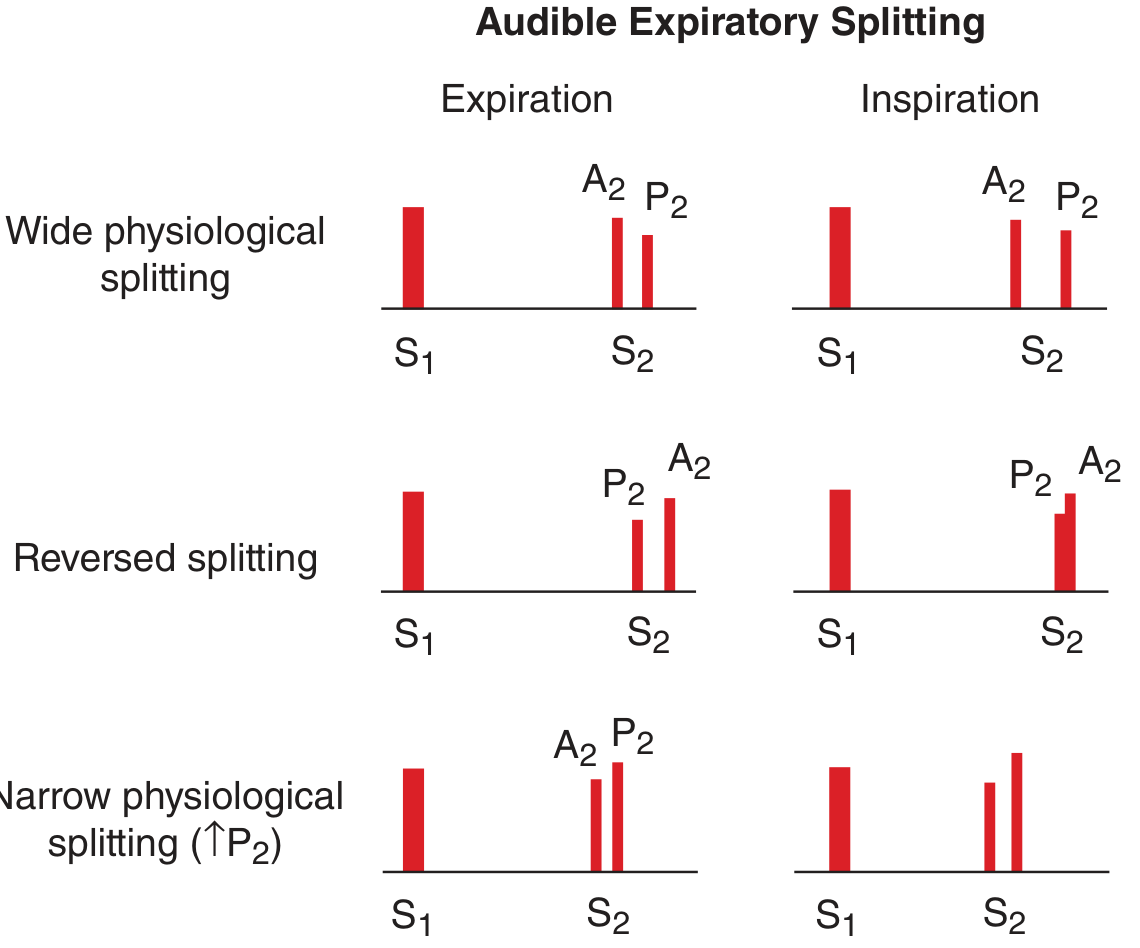
Top row: Wide physiologic splitting (A2 then P2, gap widens on inspiration). Middle row: Reversed splitting (P2 then A2; gap widens on expiration, narrows on inspiration). Bottom row: Narrow splitting with loud P2 (pulmonary hypertension). — Harrison's Principles of Internal Medicine, 22E
Quick Summary
| Pattern | Expiration | Inspiration | Key Causes |
|---|---|---|---|
| Normal physiologic | Single S2 | Split (A2·P2) | Normal |
| Wide physiologic | Split (A2·P2) | Wider split | RBBB, early A2 (MR) |
| Reversed/Paradoxical | Split (P2·A2) | Single | LBBB, HOCM, severe AS, RV pacing |
| Fixed | Split | Same width | ASD (ostium secundum) |
| Narrow | Split (close A2·P2) | Split | Pulmonary hypertension |
The hallmark of reversed splitting: the split is heard on expiration and disappears on inspiration — the opposite of normal. — Fuster and Hurst's The Heart, 15th Ed.; Harrison's Principles of Internal Medicine, 22E
Explain clearly
S2 Splitting — Clear Explanation
Step 1: What is S2?
S2 is the "dub" of "lub-dub." It has two components:
- A2 = aortic valve closing
- P2 = pulmonary valve closing
Normally, A2 comes first, then P2 — because the left ventricle finishes ejecting slightly before the right ventricle.
Step 2: Why does inspiration matter?
On inspiration, more blood is sucked into the right side of the heart. So the right ventricle takes longer to eject → pulmonary valve closes later → P2 is delayed.
The left side is unaffected.
So on inspiration, A2 and P2 move further apart → you hear two sounds (split S2).
On expiration, they come together → you hear one sound.
This is normal (physiologic) splitting.
Step 3: Now — what does "Early A2, Late P2" mean?
This phrase describes a situation where the gap between A2 and P2 is wider than normal — A2 comes earlier than it should, or P2 comes later than it should (or both).
There are two scenarios:
Scenario A: Early A2 (LV ejects too quickly)
The left ventricle empties faster than normal → aortic valve closes early → A2 moves forward in time → bigger gap to P2.
Classic cause: Severe Mitral Regurgitation (MR)
In MR, blood leaks backward into the left atrium during systole. The LV empties rapidly (both forward into aorta AND backward into LA) → LV finishes ejecting very early → A2 is early.
Result: Wide gap between A2 and P2, audible even on expiration = wide physiologic splitting.
Scenario B: Late P2 (RV ejects too slowly)
The right ventricle takes longer than normal to eject → pulmonary valve closes late → P2 is delayed → bigger gap from A2.
Classic causes:
- Right Bundle Branch Block (RBBB) — RV activation is delayed → RV contracts late → P2 is very late
- Pulmonary stenosis — RV has to work harder → takes longer → P2 delayed
- Pulmonary hypertension — RV faces high pressure → prolonged ejection
Result: Wide gap, audible on expiration = wide physiologic (persistent) splitting.
Scenario C: Reversed Splitting (P2 before A2)
Here the delay is so severe on the A2 side that A2 is pushed past P2 — now P2 comes first, A2 comes second. The order is reversed.
This happens when LV ejection is pathologically prolonged:
| Cause | Why A2 is delayed |
|---|---|
| LBBB | LV activated late → contracts late → A2 late |
| HOCM | LV outflow obstructed → LV takes longer to eject |
| RV pacing | RV paced first → LV activated late |
| Severe AS | LV fights high resistance → prolonged ejection |
Respiratory behavior is paradoxical (opposite of normal):
- On expiration: P2 and A2 are far apart → you hear a split
- On inspiration: normal inspiratory delay pulls P2 toward A2 (which is already late) → gap closes → you hear one sound
This is why it's called paradoxical splitting — the split appears on expiration and disappears on inspiration, exactly backwards from normal.
Summary Table
| Situation | A2 timing | P2 timing | Heard split on | Cause |
|---|---|---|---|---|
| Normal | Normal | Slightly delayed on inspiration | Inspiration only | Normal |
| Early A2 | Early | Normal | Expiration + Inspiration | Severe MR |
| Late P2 | Normal | Very late | Expiration + Inspiration | RBBB, PS |
| Reversed | Very late | Normal | Expiration only | LBBB, HOCM, RV pacing |
| Fixed | Normal | Late | Both, unchanged | ASD |
One-line Memory Aid
Normal: split on inspiration (P2 delayed by more RV blood) Wide physiologic: split on both phases (A2 early OR P2 late, but order preserved) Reversed/Paradoxical: split on expiration only (A2 so late it crosses past P2)
S3 s4 sounds
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent content. Here's a clear explanation:
S3 and S4 Heart Sounds
First, understand the cardiac cycle in diastole:
S1 ──────── SYSTOLE ──────── S2 ─── [diastole] ─── S1
↑ ↑
S3 S4
Diastole has two filling phases:
- Early rapid filling — mitral valve opens, blood rushes from LA into LV passively
- Late filling (atrial kick) — atria contract to push the last ~20% of blood into the ventricle
S3 and S4 arise from these two phases respectively.
S3 — The Early Diastolic Sound
When does it occur?
100–150 ms after S2, during early rapid filling.
What causes the sound?
When blood rushes from the LA into the LV rapidly, if the ventricle is either:
- Too full / overfilled (high filling pressure), or
- Too stiff to expand (poor compliance)
...the chordae tendineae and ventricular walls suddenly tense as the LV fills up quickly → vibration → S3.
Two completely opposite causes:
| Cause | What's happening | Who |
|---|---|---|
| Pathological | LV is stiff and non-compliant; high LA pressure drives blood in forcefully → tensing of walls | Heart failure (systolic), dilated cardiomyopathy, severe MR |
| Physiological | LV is very vigorous and "sucks" blood in powerfully in early diastole; higher preload, normal pressures | Young healthy people, athletes, pregnancy |
S3 in a person under 40 = likely normal. S3 in a person over 40 = assume organic heart disease until proven otherwise. — Fuster and Hurst's The Heart, 15th Ed.
How to hear it:
- Low-pitched — use the bell of the stethoscope (light pressure)
- Apex, patient in left lateral decubitus position
- Rhythm: lub-dub-ta → sounds like "Ken-tuc-ky"
Causes of pathological S3:
- Systolic heart failure (most classic — dilated, volume-overloaded LV)
- Severe mitral regurgitation (large volume returning in early diastole)
- Constrictive pericarditis (produces a variant called pericardial knock — slightly earlier, higher pitch)
S4 — The Late Diastolic Sound
When does it occur?
Just before S1, during late diastole — the atrial contraction (kick) phase.
What causes the sound?
Normally, atrial contraction quietly tops up the ventricle. But if the LV is stiff and non-compliant (diastolic dysfunction), the atrium has to contract forcefully to push blood into a resistant ventricle. This forceful late filling creates vibrations → S4.
Key rule: S4 requires atrial contraction
- S4 is absent in atrial fibrillation (no organized atrial contraction)
- This is a high-yield distinguishing feature
How to hear it:
- Low-pitched — bell of stethoscope, light pressure
- Apex (left-sided S4), or left lower sternal border (right-sided S4)
- Rhythm: ta-lub-dub → sounds like "Ten-nes-see"
Causes:
| Cause | Why |
|---|---|
| Hypertension (most common) | LV hypertrophy → stiff LV → atrium works hard |
| Aortic stenosis | LV hypertrophy from pressure overload |
| Hypertrophic cardiomyopathy (HOCM) | Stiff, hypertrophied LV |
| Acute MI / ischemia | Ischemic LV is transiently non-compliant |
| Aging | Natural reduction in LV compliance |
Right-sided S4 → pulmonary hypertension, pulmonary stenosis (increases with inspiration).
Gallop Rhythm
When heart rate increases (tachycardia), diastole shortens. S3 and S4 get pushed closer together and can fuse into a single loud sound called a summation gallop. This sounds like horse hooves — hence "gallop."
| Name | Components | Rhythm sound |
|---|---|---|
| S3 gallop | S1 + S2 + S3 | Ken-tuc-ky |
| S4 gallop | S4 + S1 + S2 | Ten-nes-see |
| Summation gallop | S4 + S1 + S2 + S3 fused | Loud triple rhythm |
S3 vs S4 — Side-by-Side
| Feature | S3 | S4 |
|---|---|---|
| Timing in diastole | Early (after S2) | Late (before S1) |
| Phase | Rapid filling | Atrial kick |
| Mechanism | Overfilled / rapidly filling LV | Stiff LV, forceful atrial contraction |
| Present in AF? | Yes | No |
| Normal in young? | Yes | No (always pathological) |
| Key association | Systolic HF, MR | HTN, LVH, AS, HOCM, ischemia |
| Pitch | Low | Low |
| Best heard with | Bell (light pressure), apex, left lateral | Bell, apex |
— Fuster and Hurst's The Heart, 15th Ed.; Guyton and Hall Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.