Anemia treatment in MHD patients give poster form
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Generating Image
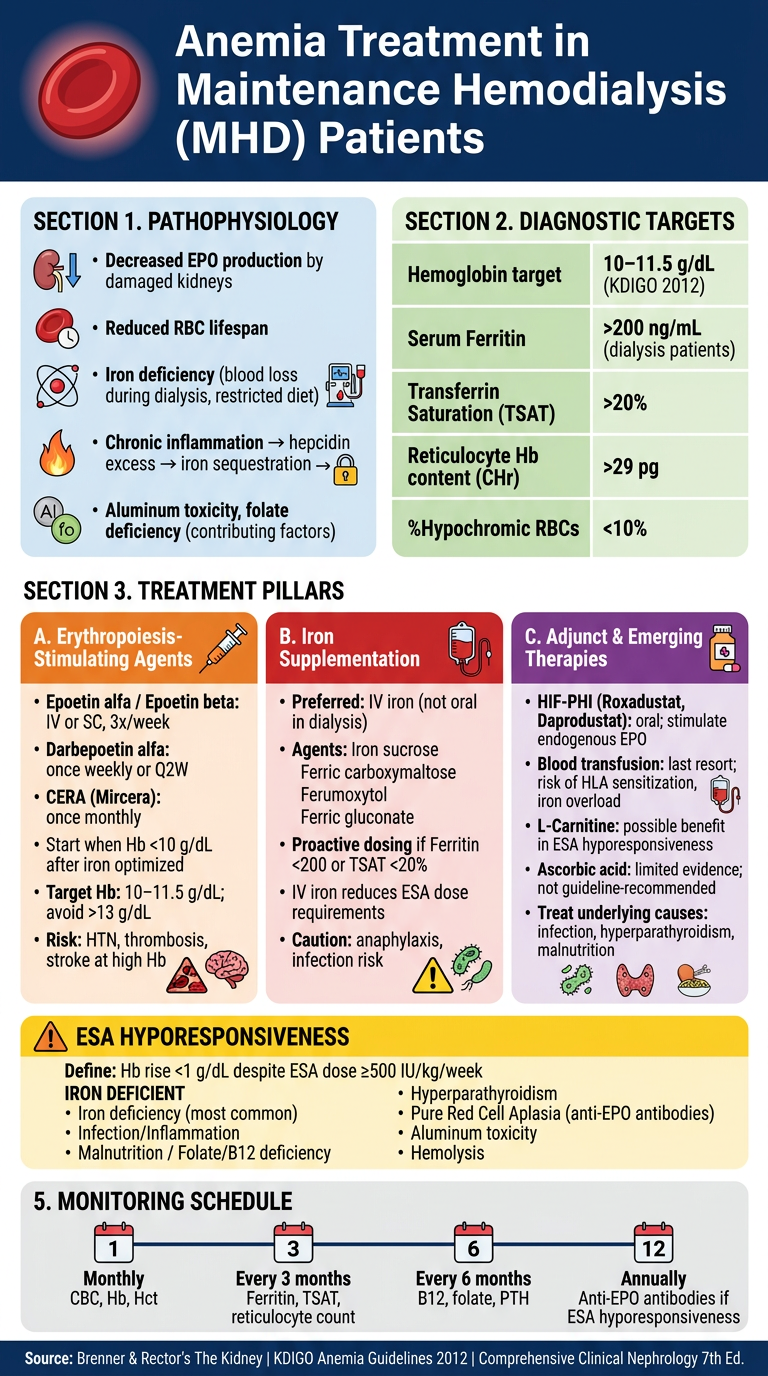
Here is the clinical poster on Anemia Treatment in Maintenance Hemodialysis (MHD) Patients, covering all key domains:
Poster Summary
Pathophysiology
- Primary cause: reduced EPO production by failed kidneys + iron deficiency from dialysis-related blood losses + hepcidin-mediated iron sequestration due to chronic inflammation
Diagnostic Targets (KDIGO 2012)
| Parameter | Target |
|---|---|
| Hemoglobin | 10–11.5 g/dL |
| Serum Ferritin | >200 ng/mL |
| TSAT | >20% |
| %Hypochromic RBCs | <10% |
Three Treatment Pillars
-
ESAs — Epoetin alfa/beta (3×/week IV/SC), Darbepoetin alfa (weekly/Q2W), CERA (monthly). Initiate when Hb <10 g/dL after iron replete. Avoid Hb >13 g/dL (↑ CVD/stroke risk).
-
IV Iron — Preferred over oral in dialysis patients. Agents: iron sucrose, ferric carboxymaltose, ferumoxytol, ferric gluconate. IV iron reduces ESA dose requirements significantly.
-
Adjuncts/Emerging — HIF-PHI (Roxadustat, Daprodustat) — oral agents stimulating endogenous EPO; Blood transfusion as last resort (risk: HLA sensitization, iron overload).
ESA Hyporesponsiveness — Defined as Hb rise <1 g/dL despite high ESA doses. Most common cause: iron deficiency. Others: infection, hyperparathyroidism, pure red cell aplasia (anti-EPO antibodies), B12/folate deficiency.
Monitoring — Monthly CBC/Hb; Every 3 months: ferritin, TSAT; Every 6 months: PTH, B12, folate.
Sources: Brenner & Rector's The Kidney | KDIGO Anemia Guidelines 2012 | Comprehensive Clinical Nephrology 7th Ed.
Generate a comparison table of ESA agents (epoetin vs darbepoetin vs CERA)
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Generating Image
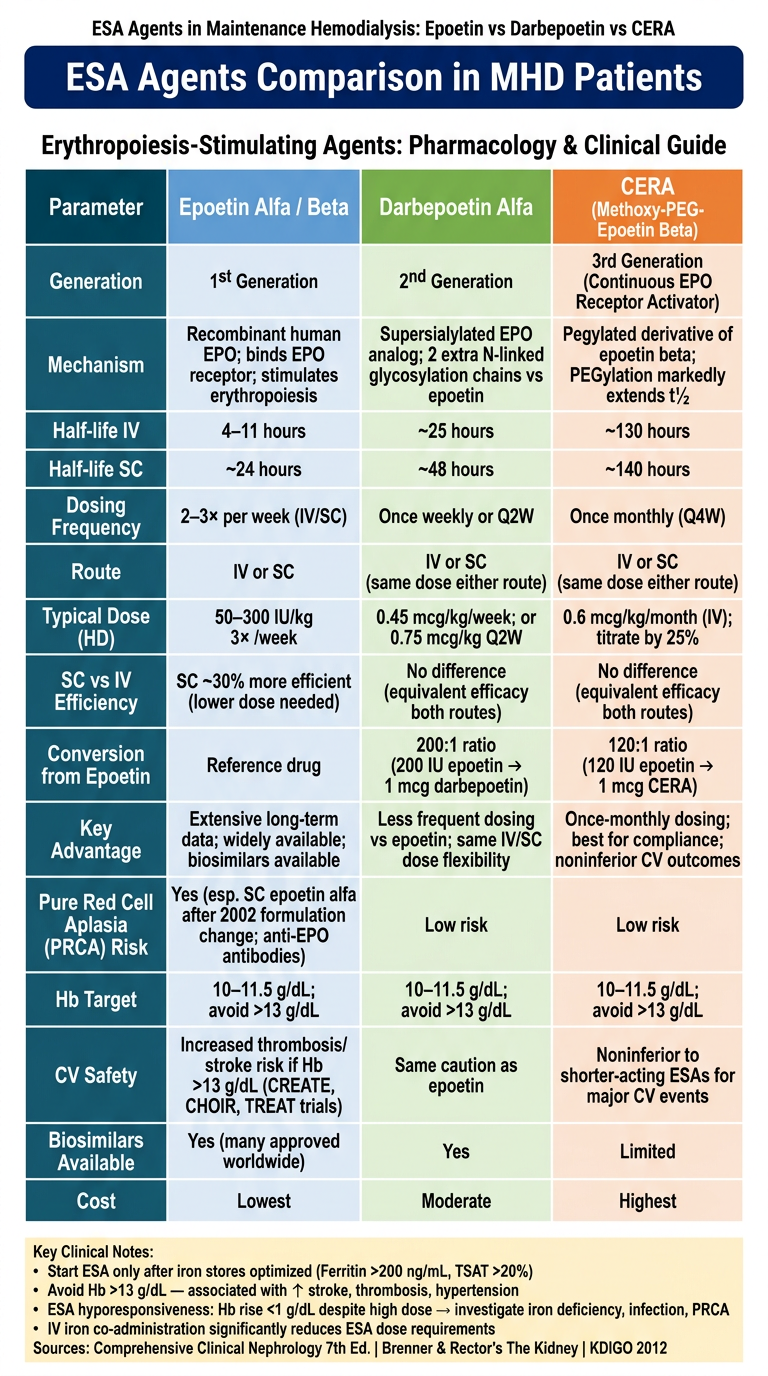
Here is the full comparison table. Key takeaways from the textbooks:
ESA Agents at a Glance
| Parameter | Epoetin α/β | Darbepoetin α | CERA |
|---|---|---|---|
| Generation | 1st | 2nd | 3rd |
| Half-life (IV) | 4–11 h | ~25 h | ~130 h |
| Half-life (SC) | ~24 h | ~48 h | ~140 h |
| Dosing | 2–3×/week | Weekly or Q2W | Once monthly |
| SC vs IV dose | SC ~30% more efficient | Same dose both routes | Same dose both routes |
| Conversion ratio | Reference | 200 IU epoetin = 1 mcg | 120 IU epoetin = 1 mcg |
| PRCA risk | Higher (esp. SC epoetin alfa) | Low | Low |
| Cost | Lowest | Moderate | Highest |
| Biosimilars | Many available | Yes | Limited |
Structural basis for prolonged half-life:
- Darbepoetin: 2 extra N-linked glycosylation chains → reduced clearance
- CERA: PEGylation of epoetin beta → dramatically slows clearance
Shared safety caveat: All ESAs carry risk of hypertension, thrombosis, and stroke when Hb exceeds 13 g/dL (demonstrated in CREATE, CHOIR, and TREAT trials). Target Hb remains 10–11.5 g/dL for all three agents per KDIGO 2012.
Sources: Comprehensive Clinical Nephrology 7th Ed. | Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.