Diabetes and its correlation with Chronic kidney disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetic nephropathy" AND "chronic kidney disease"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information to write a detailed, well-structured response. Let me compile everything.
Diabetes and Its Correlation with Chronic Kidney Disease (Diabetic Kidney Disease)
Diabetic kidney disease (DKD), also called diabetic nephropathy, is the leading cause of end-stage kidney disease (ESKD) worldwide. Around 30-40% of patients with type 2 diabetes develop diabetic nephropathy, and it represents the most important microvascular complication of both type 1 and type 2 diabetes.
1. Epidemiology
-
Diabetes is responsible for approximately 44% of new ESKD cases in developed countries.
-
In Japan, diabetic nephropathy overtook glomerulonephritis as the leading underlying cause of ESKD since 1997; in China, it has surpassed glomerulonephritis as the leading cause of CKD among hospitalized patients.
-
In Singapore, 53% of patients with type 2 diabetes were found to have concomitant CKD in a cross-sectional survey of 1,861 patients.
-
Globally, deaths from CKD due to diabetes increased by nearly 107% between 1990 and 2013 (Global Burden of Disease Study).
-
The International Diabetes Federation projected the number of adults with diabetes would rise from 415 million (2015) to 642 million by 2040, with the highest growth rates expected in Africa.
-
Brenner and Rector's The Kidney, 2-Volume Set, pp. 3381, 3295
2. Pathophysiology - How Diabetes Damages the Kidney
2a. Glomerular Hyperfiltration (Early Stage)
The earliest functional change is glomerular hyperfiltration - an increase in GFR driven by afferent arteriolar dilation and efferent arteriolar constriction from the renin-angiotensin-aldosterone system (RAAS) activation. This increased intraglomerular pressure initiates structural injury over time.
2b. Structural Kidney Lesions
The kidneys are prime targets of diabetes, with three main categories of lesions:
1. Glomerular Lesions (most important)
- GBM thickening - the very first change detectable by electron microscopy, developing within 2 years of onset of type 1 diabetes; associated with increased α₃ and α₄ chains of type IV collagen.
- Diffuse mesangial sclerosis - increase in mesangial matrix with mesangial cell proliferation; found in most individuals with >10 years of diabetes. When severe, causes nephrotic syndrome (proteinuria, hypoalbuminemia, edema).
- Nodular glomerulosclerosis (Kimmelstiel-Wilson lesion) - the pathognomonic lesion of diabetic nephropathy; ball-like deposits of laminated matrix in the periphery of the glomerulus, seen in 15-30% of long-term diabetics.
2. Renal Vascular Lesions
- Hyaline arteriolosclerosis affects both the afferent AND efferent arterioles - efferent arteriolar involvement is virtually unique to diabetes and distinguishes it from hypertensive nephrosclerosis.
- Vascular compromise leads to ischemia and diffuse cortical scarring (nephrosclerosis).
3. Pyelonephritis / Tubular Lesions
- Both acute and chronic pyelonephritis are more severe in diabetics.
- Necrotizing papilitis (papillary necrosis) is much more prevalent in diabetics.
- Tubular basement membrane thickening also occurs.
Below: Biopsy findings in DKD - (A) Kimmelstiel-Wilson nodules (asterisks) with mesangial expansion and arteriolar hyalinosis (arrowhead); (B) GBM thickening by electron microscopy; (C) tubular BM thickening; (D) linear IgG on immunofluorescence.
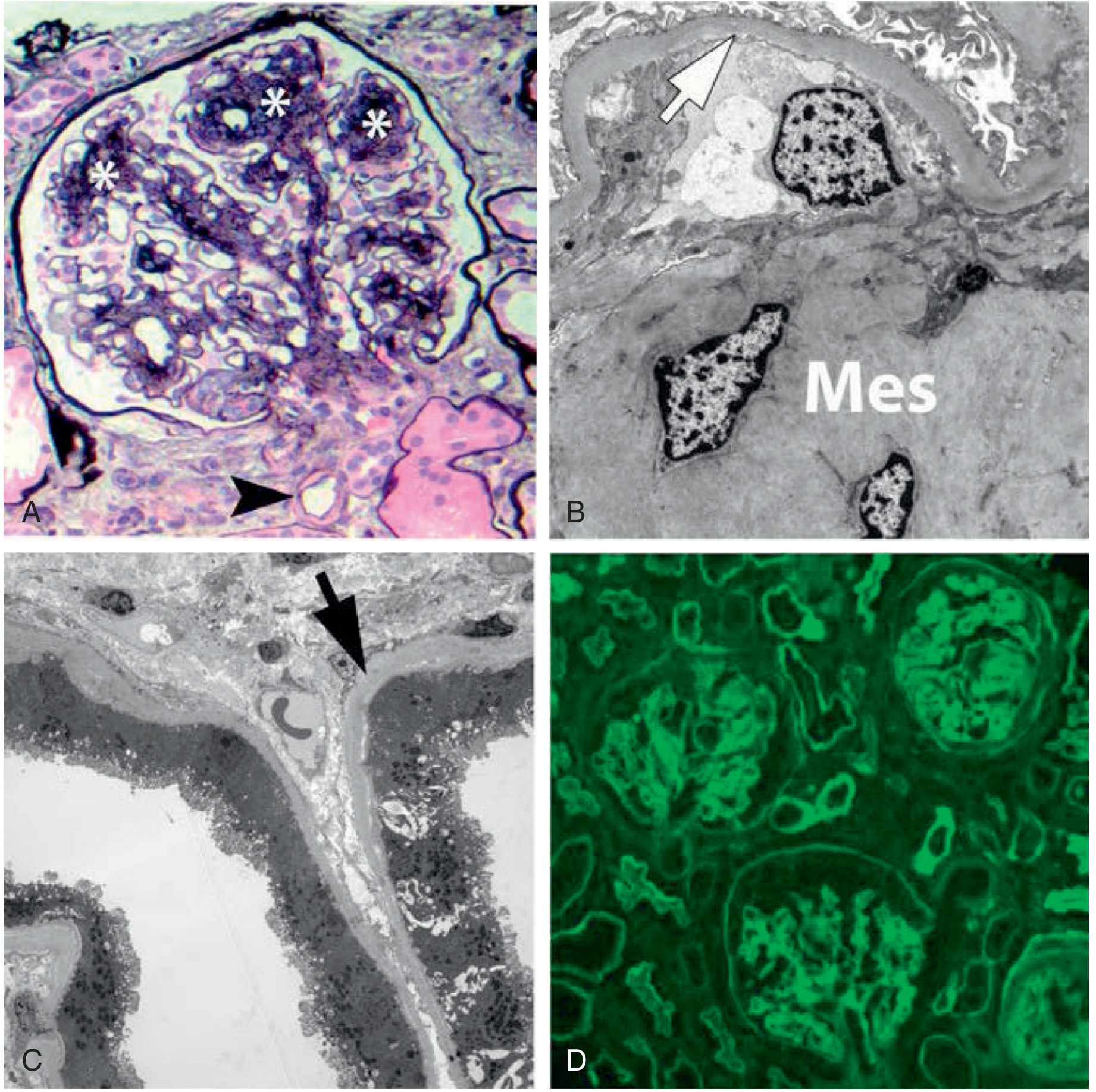
Fig. - Classical biopsy findings in diabetic kidney disease. Brenner and Rector's The Kidney
Below: Severe renal hyaline arteriolosclerosis (PAS stain) - markedly thickened, tortuous afferent arteriole:
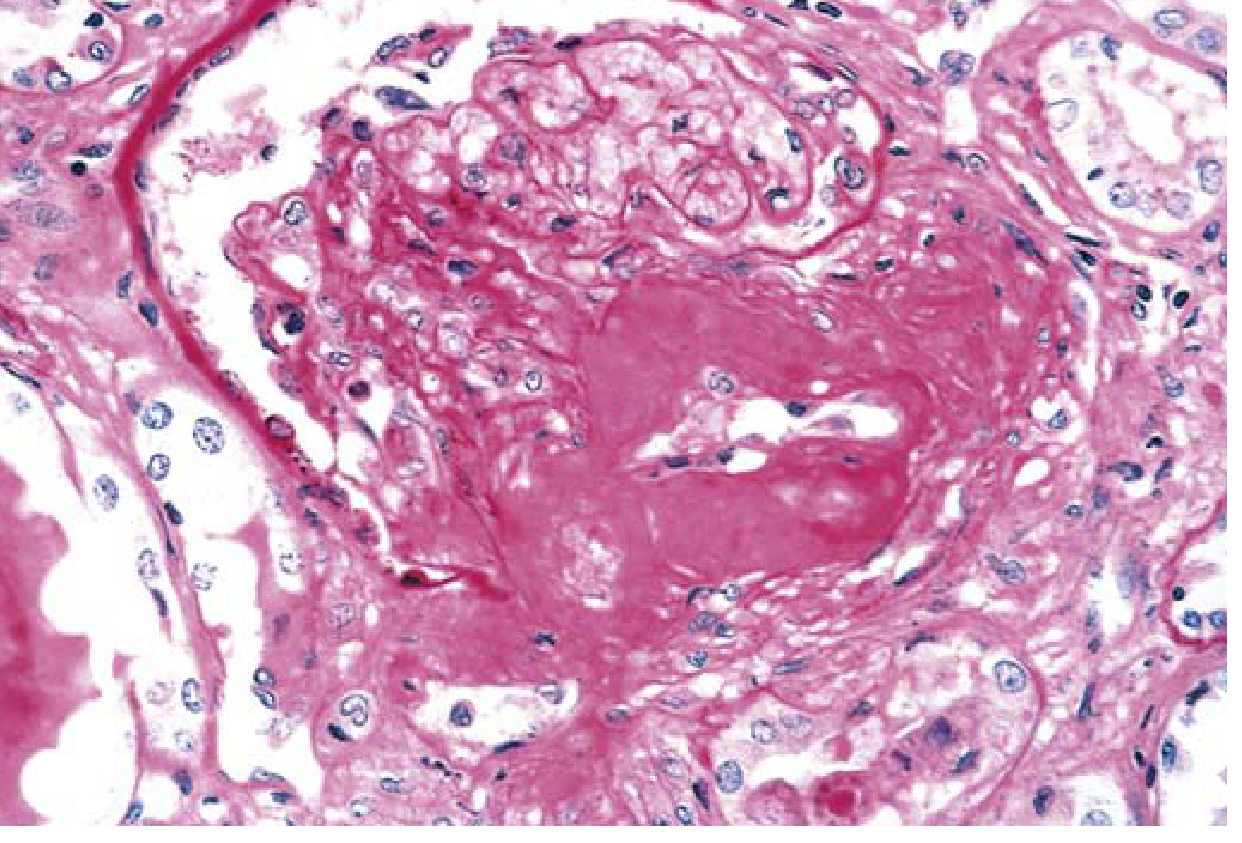
Fig. - Severe renal hyaline arteriolosclerosis. Robbins & Kumar Basic Pathology
- Robbins & Kumar Basic Pathology, pp. 751-752
- Brenner and Rector's The Kidney, pp. 1777-1778
3. Molecular & Genetic Mechanisms
-
RAAS activation plays a central role - ACE gene polymorphisms (especially the DD genotype) are associated with higher susceptibility to ESKD.
-
Advanced glycation end products (AGEs) from chronic hyperglycemia damage glomerular structures.
-
Oxidative stress and inflammation: TNF receptor 1 and 2 are strongly associated with impaired GFR and ESKD progression; MCP-1 (monocyte chemoattractant protein-1) predicts renal function decline; IL-6, IL-10, and ICAM-1 gene polymorphisms have been linked to progression.
-
Podocyte injury and loss - progressive reduction in podocyte number correlates with mesangial expansion and GFR decline.
-
TGF-β drives extracellular matrix accumulation and fibrosis.
-
Microalbuminuria concentrations increase logarithmically at HbA1c levels above 8%.
-
Brenner and Rector's The Kidney, pp. 1774, 3381
4. Clinical Stages and Progression
DKD follows a well-characterized progression:
| Stage | Feature |
|---|---|
| Stage 1 | Glomerular hyperfiltration, normal albumin excretion |
| Stage 2 | Structural damage, normoalbuminuria (silent) |
| Stage 3 | Microalbuminuria (30-300 mg/day) - "incipient nephropathy" |
| Stage 4 | Macroalbuminuria (>300 mg/day), declining GFR - "overt nephropathy" |
| Stage 5 | ESKD requiring dialysis or transplant |
The flowchart below (from the UK Prospective Diabetes Study, UKPDS) shows annual transition rates between stages, highlighting that at each stage more patients die per year than progress to the next stage:
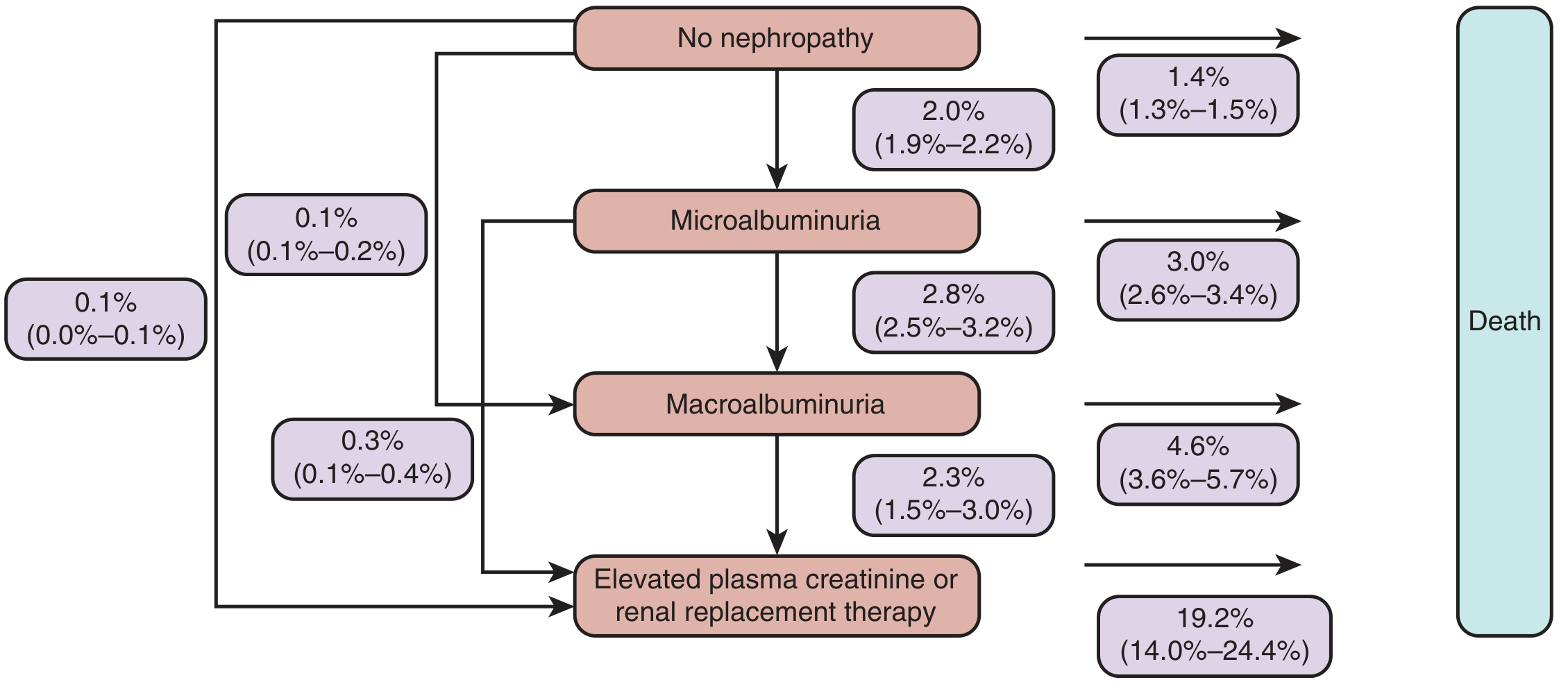
Fig. 39.4 - Annual transition rates between stages of DKD in type 2 diabetes. Brenner and Rector's The Kidney
Key point: After developing microalbuminuria, more patients die each year than transition to the next stage, underscoring the cardiovascular mortality risk of even early DKD.
- Brenner and Rector's The Kidney, p. 1776
5. Prognosis and Mortality
The graph below shows 10-year mortality in type 2 diabetes by degree of kidney involvement:
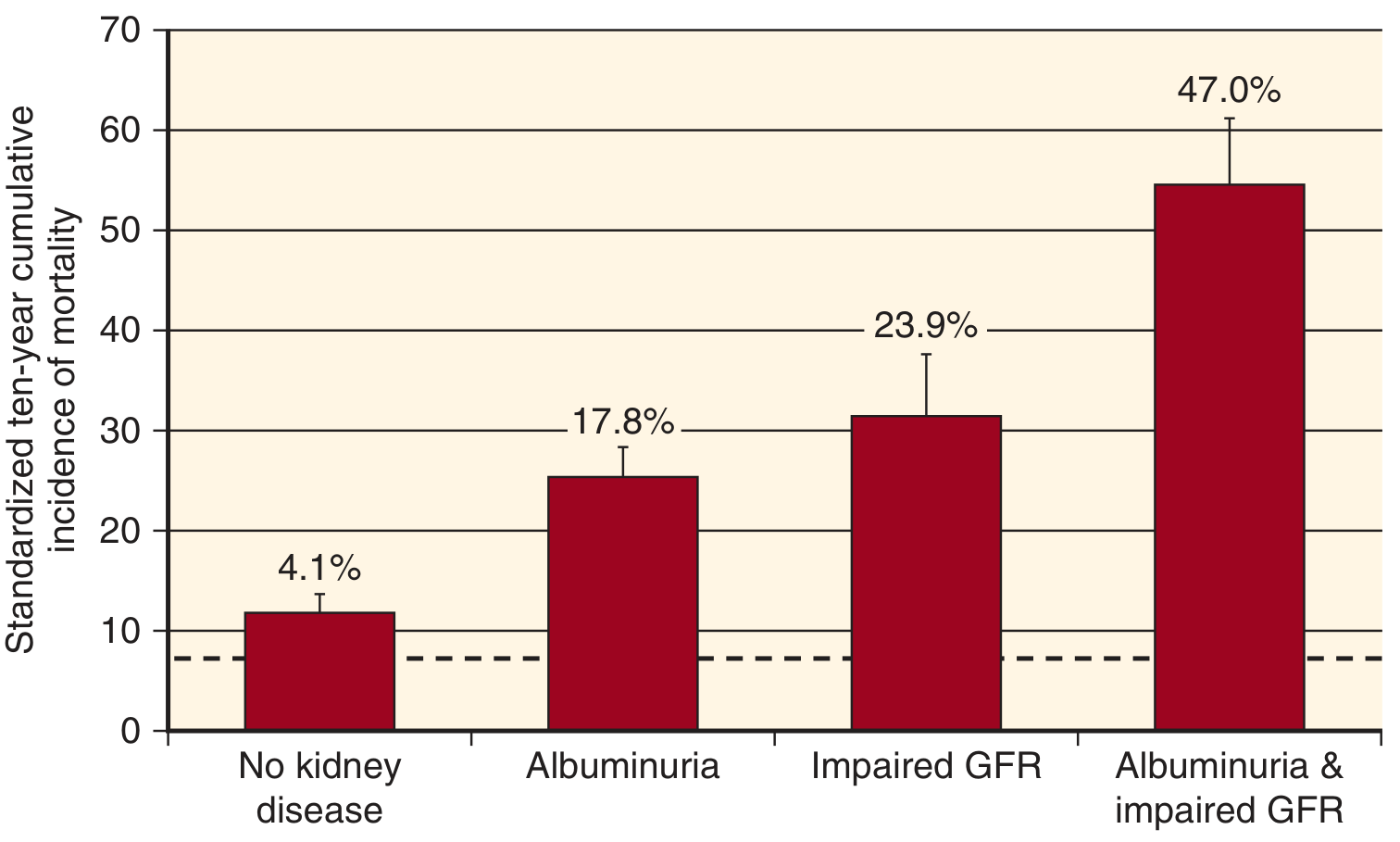
Fig. 39.5 - 10-year mortality in type 2 diabetes. Patients with both albuminuria AND impaired GFR carry a 47% 10-year cumulative mortality. Brenner and Rector's The Kidney
Key statistics:
- Type 2 diabetes + no kidney disease: ~12% (4.1% excess)
- Type 2 diabetes + albuminuria only: ~25% (17.8% excess)
- Type 2 diabetes + impaired GFR only: ~32% (23.9% excess)
- Type 2 diabetes + both albuminuria AND impaired GFR: ~55% (47% excess)
Meta-analyses confirm that albuminuria even in the microalbuminuric range is a strong predictor of all-cause mortality, cardiovascular mortality, stroke, and ESKD - both in diabetics and non-diabetics.
- Brenner and Rector's The Kidney, p. 1776
6. Management
Glycemic Control
- Intensive glucose control in type 1 diabetes clearly prevents development and progression of DKD.
- In type 2 diabetes, evidence is less certain; treating to HbA1c <7.0% (53 mmol/mol) is not recommended in CKD stages 3-5 due to the risk of severe hypoglycemia counterbalancing benefits.
Blood Pressure Control
- The vast majority of patients with DKD require 3 or more antihypertensive drugs to achieve target BP.
- ACE inhibitors and ARBs are first-line agents - they slow progression at both early (microalbuminuria) and late (proteinuria with reduced GFR) stages, independent of BP-lowering effects.
- Dual RAAS blockade (ACE inhibitor + ARB) is NOT recommended - the VA NEPHRON-D and ONTARGET trials showed increased acute kidney injury and hyperkalemia without benefit.
- The ADVANCE trial showed ACE inhibitor (perindopril) + thiazide diuretic (indapamide) significantly reduces BP and risk of kidney and cardiovascular complications in type 2 diabetes.
SGLT2 Inhibitors
SGLT2 inhibitors (empagliflozin, canagliflozin, dapagliflozin) have transformed DKD management:
- Reduce intraglomerular hypertension by promoting natriuresis.
- The 2026 network meta-analysis (PMID 41147324) confirms their superiority in renal outcomes among novel antidiabetic agents in T2DM with CKD.
- Current guidelines recommend SGLT2 inhibitors in CKD and non-CKD patients with CVD and/or multiple cardiovascular risk factors alongside RAAS blockade.
GLP-1 Receptor Agonists
- Also reduce cardiovascular events in patients with type 2 diabetes at high cardiovascular risk, with some renoprotective benefit, especially by reducing obesity and BP.
Finerenone (Non-steroidal Mineralocorticoid Receptor Antagonist)
- The FIDELIO-DKD trial (5,734 patients with type 2 diabetes, eGFR 25-75 mL/min/1.73 m²) showed finerenone added to ACE inhibitor or ARB significantly reduced the composite of death, kidney failure, or sustained eGFR decline.
- It significantly reduced cardiovascular mortality and morbidity in DKD compared with placebo.
Lipid Management & Lifestyle
-
Dyslipidemia treatment is integral to managing diabetic CKD patients.
-
Physical inactivity is associated with albuminuria and cardiovascular mortality - physical activity should be encouraged.
-
Smoking is associated with CKD progression in diabetic patients.
-
Harrison's Principles of Internal Medicine 22E, p. (Diabetic Nephropathy section)
-
Comprehensive Clinical Nephrology, 7th Edition, p. 1144
-
National Kidneys Foundation Primer on Kidney Diseases, 8e
7. Biomarkers for Monitoring
| Biomarker | Significance |
|---|---|
| Urine albumin-creatinine ratio (UACR) | Screening and staging; microalbuminuria = 30-300 mg/g |
| eGFR | Staging CKD severity |
| HbA1c | Glycemic control; microalbuminuria increases logarithmically above 8% |
| TNFR1 and TNFR2 | Predict ESKD, macroalbuminuria, and cardiovascular events |
| Urine MCP-1 | Predicts renal function decline and progression to dialysis |
| Urine EGF | Lower levels predict progressive CKD |
| Serum uric acid | Induces oxidative stress and fibrosis, emerging predictor |
8. Summary Table
| Aspect | Key Point |
|---|---|
| Prevalence | 30-40% of T2DM patients develop DKD |
| Hallmark lesion | Kimmelstiel-Wilson nodules (nodular glomerulosclerosis) |
| Pathognomonic finding | Efferent arteriolar hyalinosis |
| First functional change | Glomerular hyperfiltration |
| First structural change (EM) | GBM thickening (within 2 years) |
| First structural change (LM) | Mesangial expansion |
| Key drivers | Hyperglycemia, RAAS activation, oxidative stress, inflammation |
| Cornerstone therapy | RAAS blockade (ACEi or ARB) + SGLT2 inhibitor |
| New addition | Finerenone (FIDELIO-DKD trial) |
| Prognosis signal | Albuminuria + reduced GFR = 47% 10-year mortality |
Recent evidence note: A 2026 network meta-analysis (PMID 41147324) comparing novel antidiabetic agents in T2DM with CKD confirms that SGLT2 inhibitors show the best renal outcomes, consistent with current guidelines. A 2024 Cochrane review (PMID 39171639) also highlights the role of structured education programmes in managing patients with CKD and diabetes, supporting a holistic approach.
This is a shared conversation. Sign in to Orris to start your own chat.