EVLA in depth research procedure steps and steps which can be updated based on outcome Give real ultrasound images Also various types of fibres use pros and cons Instrument requirements for EVLA and its alternative less cost effective with same results Also divide procedure into preop things to be done intra op and post op care If complications how to prevent and treat Compare EVLA done of below Short shafenous Reticular Giacomi vein Vs GSV its outcome which is more important for symptoms relief Also give me idea about scope of research in EvLa and how can I improve this at In India
"endovenous laser ablation" AND "great saphenous vein" AND outcomes
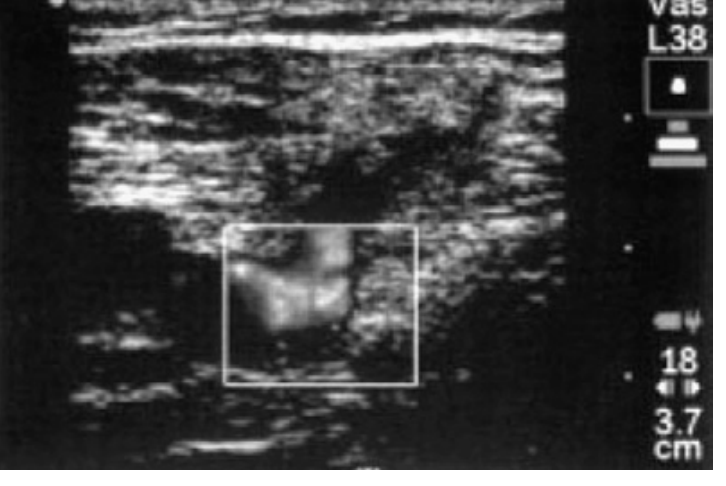
EVLA endovenous laser ablation procedure steps fiber types 1470nm 980nm ultrasound images
"endovenous laser" AND "small saphenous" OR "Giacomini" OR "reticular vein" ablation outcomes
PMID: 37779391
PMID: 40449724
EVLA ultrasound guided duplex small saphenous vein Giacomini reticular vein procedure real ultrasound images
EVLA India scope research varicose veins cost 1470nm laser diode affordable alternative radiofrequency
PMID: 34378180
EVLA complications EHIT deep vein thrombosis nerve injury prevention treatment management 2023 2024
ENDOVENOUS LASER ABLATION (EVLA) - Complete Clinical Reference
1. MECHANISM OF ACTION
- Endothelial destruction
- Vein wall contraction (collagen shrinkage)
- Luminal obliteration
- Eventual vein fibrosis and degeneration
- 810/980 nm: deoxygenated hemoglobin is the primary target (blood heated -> steam bubbles damage wall)
- 1320 nm: water in the vein wall is the target
- 1470 nm: water in the vein wall - more direct wall effect, less steam, less pain
2. INDICATIONS
- Symptomatic varicose veins (leg heaviness, aching, throbbing, edema)
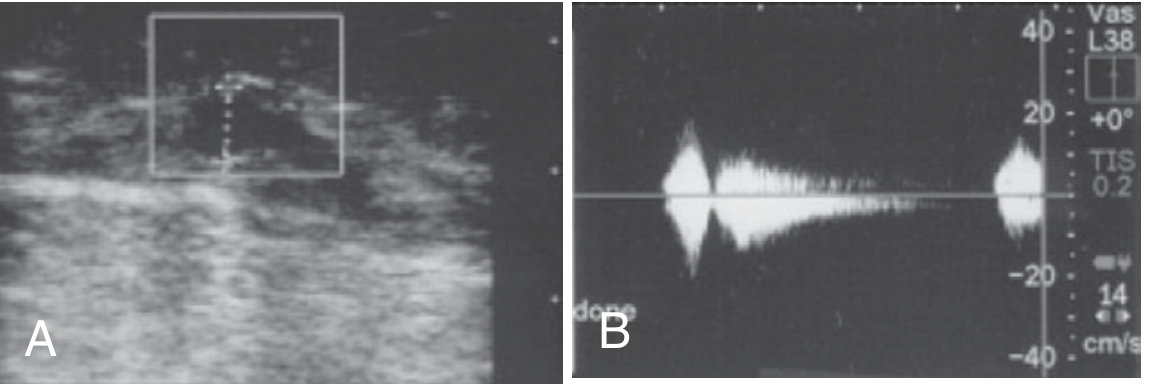
- Duplex-confirmed reflux in GSV, SSV, Giacomini vein, or accessory saphenous veins (reflux >0.5-1 sec; clinically significant >2 sec)
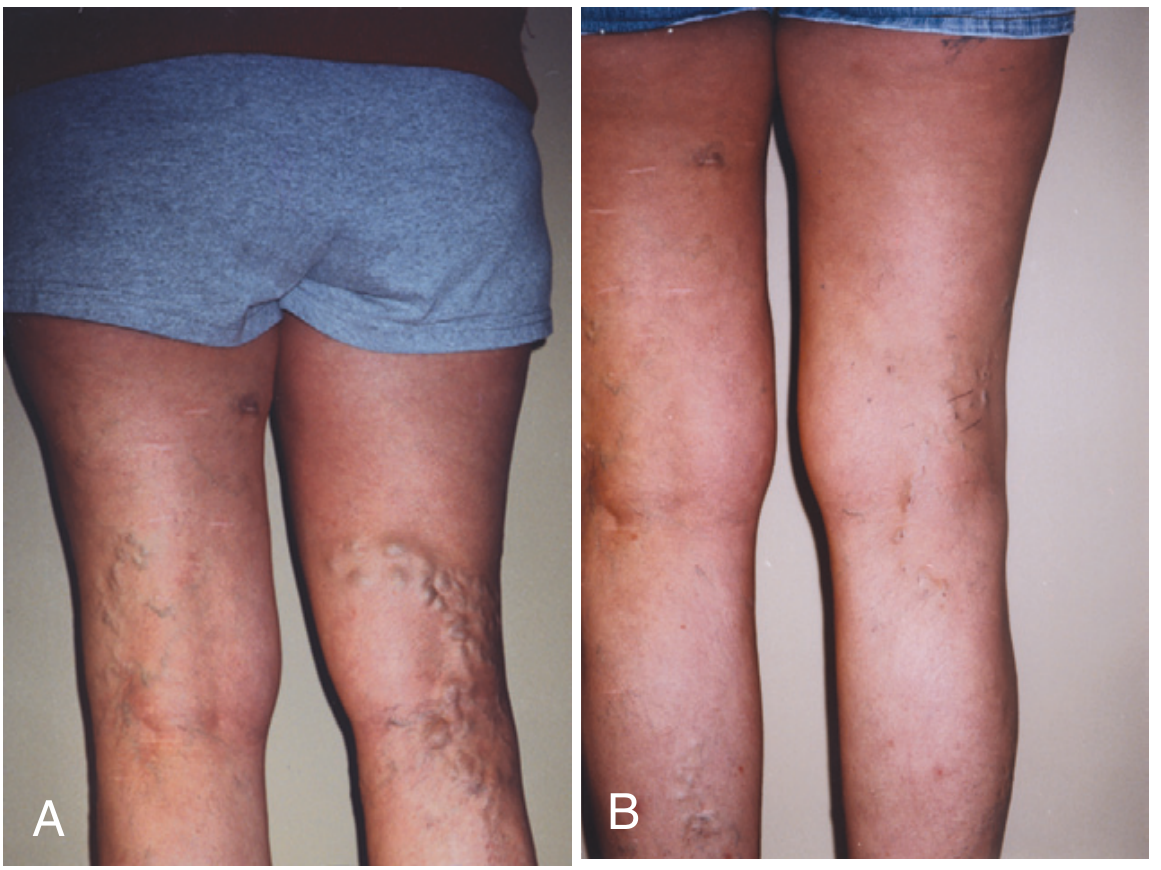
- CEAP C2-C6 venous disease
- Skin changes from chronic venous insufficiency: hyperpigmentation, lipodermatosclerosis, corona phlebectasia, venous ulceration
- Minimal tortuosity of the target vein to allow catheter passage
- Fully ambulatory patient
- Inability to ambulate post-procedure
- Active superficial or deep venous thrombosis
- Hypoplastic deep venous system
- Pregnancy
- RFA (not EVLA) is also contraindicated with pacemakers
3. PRE-OPERATIVE PHASE
3a. Clinical Assessment
- Directed history: duration and type of symptoms; response to compression stockings
- Physical examination: document skin changes (hyperpigmentation, ulceration, edema) with photography
- CEAP classification and VCSS (Venous Clinical Severity Score) baseline
- Medications: note anticoagulants, NSAIDs; consider stopping 5-7 days pre-op if needed
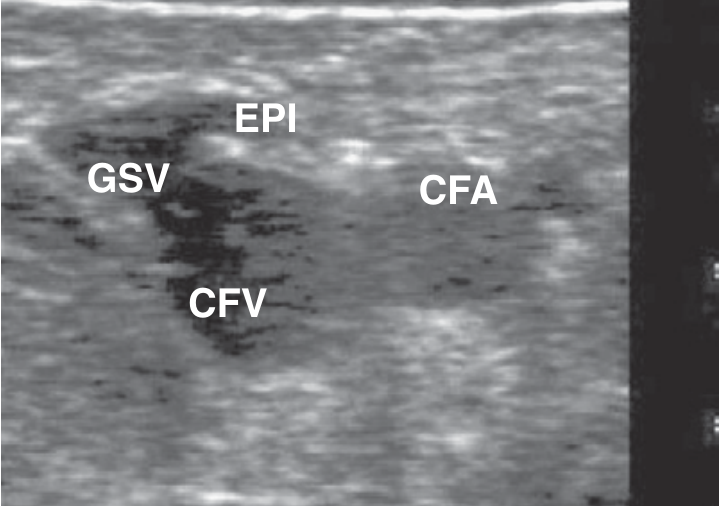
3b. Pre-procedure Duplex Ultrasound Mapping
- Start at the groin (SFJ) and map caudally along medial thigh for GSV
- For SSV: start at popliteal fossa (SPJ) - identify where the vein dives deep (at minimum 3 cm from SPJ)
- For Giacomini: trace thigh extension of SSV connecting to GSV
- Mark the vein course on skin with a marking pen
- Measure vein diameter at multiple levels
- Document reflux duration by Doppler (manual calf compression/release)
- Identify perforators, tributaries, and any anatomical variants
Key safety point for SSV: Identify the sural nerve (adjacent to SSV in lower calf). The catheter tip must not go below the point where the SSV dives deep to form the SPJ. The SPJ location is variable (L3 to L5) - always verify with ultrasound.

3c. Pre-medication
- Alprazolam 0.5 mg orally, 30 min before procedure (anxiolytic)
- NSAIDs (ibuprofen 600 mg) pre-emptively if desired
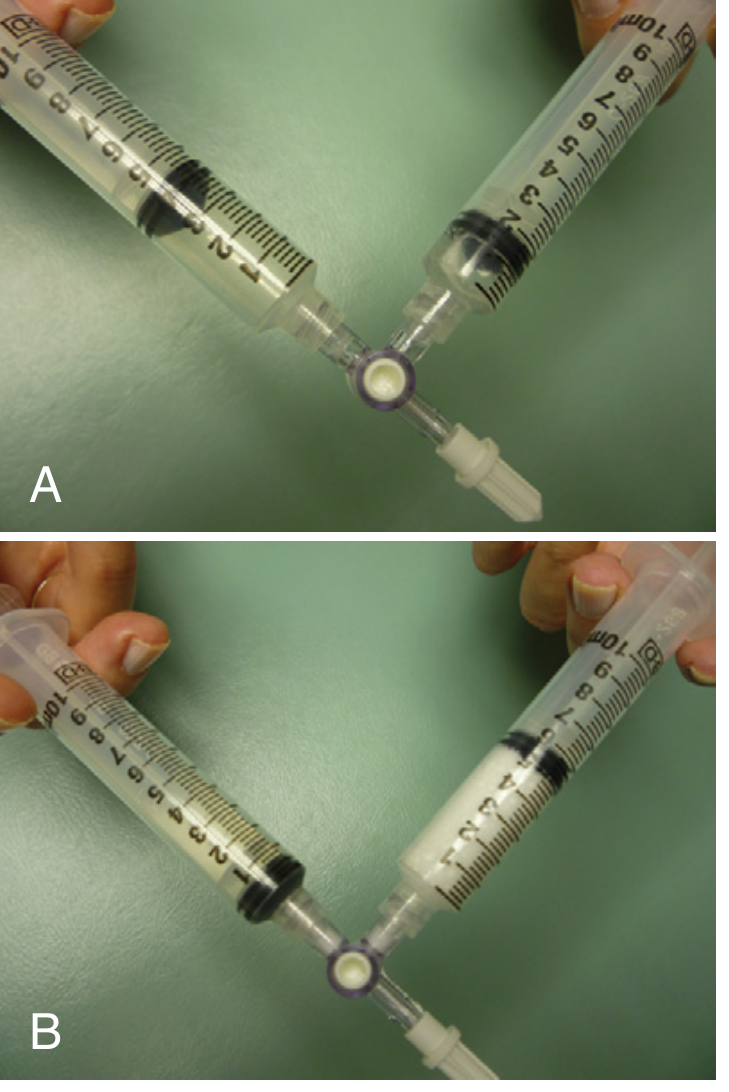
3d. Tumescent Anesthesia Preparation
4. INTRAOPERATIVE PHASE - Step-by-Step Procedure
- Protective laser eyewear for ALL staff and patient
- Sterile field: povidone-iodine prep, sterile drapes, ultrasound probe cover
- Trendelenburg position (head down) to collapse the target vein
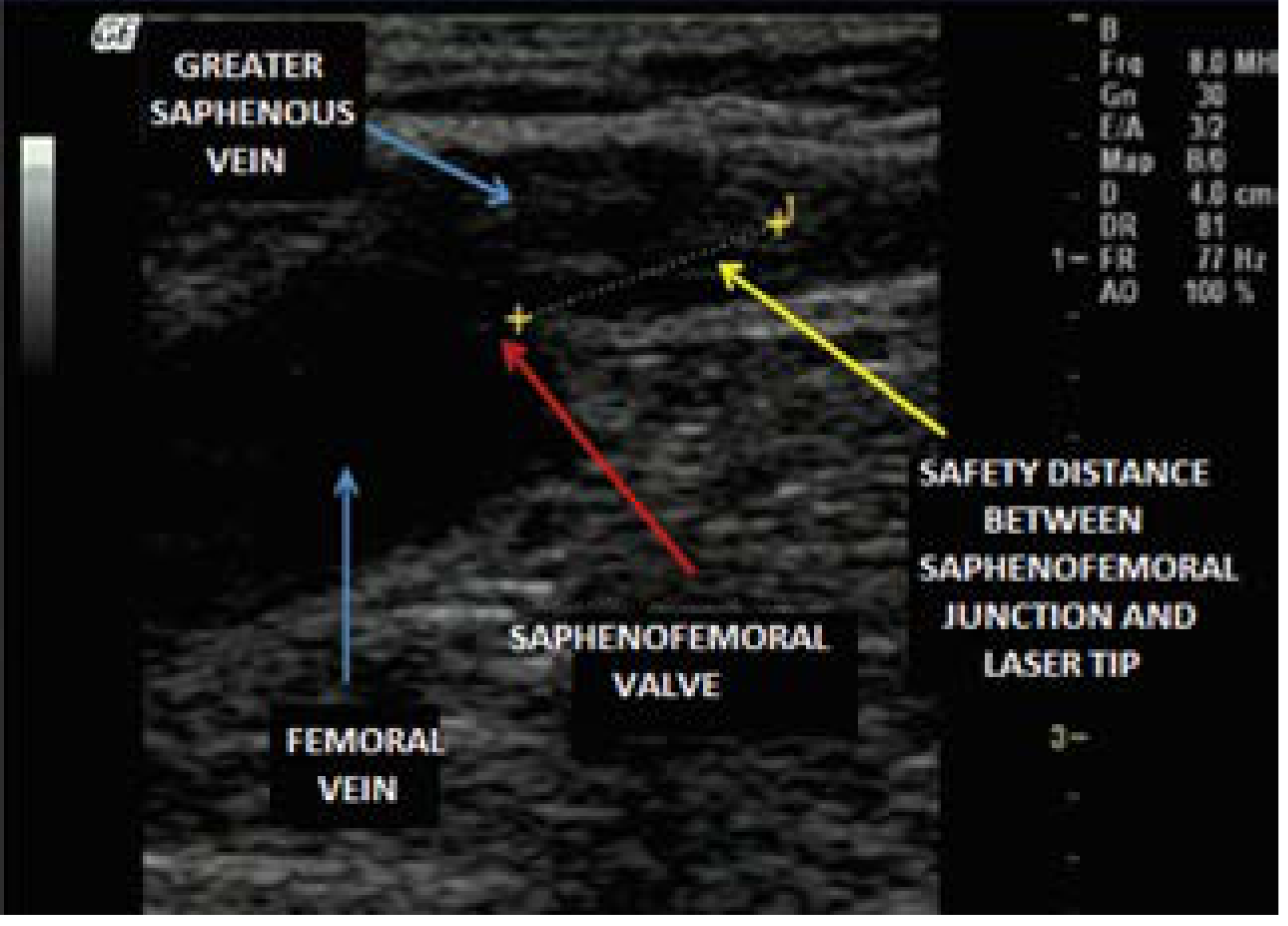
- GSV: tip must be at least 2 cm distal to the SFJ (distal to superficial epigastric vein origin)
- SSV: tip must be at least 3 cm from the SPJ, in the superficial portion of the SSV
- Compresses the vein diameter around the fiber
- Creates a heat sink protecting surrounding tissues
- Provides analgesia
- 1470 nm laser: 40 J/cm linear endovenous energy density (LEED)
- 810 nm laser: 80 J/cm LEED
- General rule: minimum 70 J/cm needed for reliable occlusion
- Practical setting: 14 W power + withdrawal rate of 2 mm/sec = 70 J/cm
- Vein spasm on attempted access: apply 2% nitroprusside topically, have patient ambulate 10 min, retry; ensure warm room temperature
- Patient too anxious: vocal reassurance ("vocal anesthesia"), lorazepam 0.5-1 mg
- Inadequate tumescence: reassess if >10 mm distance not achieved
- Wrong position: must be Trendelenburg (NOT reverse Trendelenburg)
5. POSTOPERATIVE CARE
- Immediate ambulation - do not rest post-procedure
- Class II compression stockings (30-40 mmHg), thigh-high, open toe, applied in operating suite
- Wear compression stockings overnight, then for 6 more days while ambulatory (remove at bedtime and for showering)
- Ibuprofen 600 mg TDS x 3 days, then PRN every 6 hours
- Duplex ultrasound at 3-7 days post-procedure:
- Confirm vein closure (thickened, fibrotic wall, no flow)
- Check deep venous system for adequate flow (no EHIT/DVT)
- Document femoral/popliteal vein patency
- Symptom improvement often within 1 month
- Residual varices usually need adjunct sclerotherapy or ambulatory phlebectomy (some operators do these simultaneously; others wait 1 month to assess)
- Telangiectases require separate treatment (foam sclerotherapy, transcutaneous laser)
6. LASER FIBER TYPES - PROS & CONS
A. Bare-Tip (Straight) Fiber - 810 nm / 980 nm
| Aspect | Detail |
|---|---|
| Wavelength | 810 nm, 940 nm, 980 nm |
| Target chromophore | Hemoglobin |
| Mechanism | Heats blood -> steam bubbles -> vessel wall damage indirectly |
| Pros | Lower equipment cost; simpler; widely available; well-studied long-term data |
| Cons | Higher bruising (57% in studies); higher post-op pain; forward-directed energy risks vein perforation; less uniform wall heating; higher LEED needed (80 J/cm) |
| Occlusion rate | 95-98% at 1 year |
B. Radial (Ring) Fiber - 1470 nm
| Aspect | Detail |
|---|---|
| Wavelength | 1470 nm (water-absorbing) |
| Target chromophore | Water in vein wall |
| Mechanism | Directly heats vein wall without relying on blood; 360-degree energy distribution |
| Pros | Significantly less pain (0% vs 25% in RCT); significantly less bruising (7% vs 57%); superior occlusion rates at all time points (OR 2.54 for GSV at early follow-up); 100% occlusion at 12 weeks; lower LEED required (40 J/cm); less risk of perforation; better paresthesia profile |
| Cons | Higher device cost (~2x the bare-tip); requires compatible generator; slightly more technique-sensitive for SSV (must not go too deep); disposable fibers are expensive (single-use) |
| Occlusion rate | Superior to 980 nm at early, 1-year, and medium/long-term (meta-analysis: OR 2.54 at 12-month GSV) |
C. Emerging: >1900 nm Lasers (Thulium, Water-Vapour)
- Targets water even more specifically
- A 2022 systematic review (Setia et al., PMID 35819662) showed promising early results but data are limited
- Not yet widely available or cost-effective
7. INSTRUMENT REQUIREMENTS
Standard EVLA Setup (Complete List)
| Category | Equipment |
|---|---|
| Imaging | Duplex ultrasound machine (portable or stationary, 7-10 MHz linear probe); sterile probe cover |
| Vascular access | 18-gauge 2-inch angiocatheter; 0.035-inch J-wire; No. 11 blade; 5-Fr introducer sheath with dilator; micropuncture kit (for veins <3 mm) |
| Laser system | Diode laser generator (1470 nm preferred); single-use radial laser fiber; laser-protective eyewear for all personnel; aiming beam laser |
| Tumescent anesthesia | 250 mL 0.9% saline bags; 1% lidocaine; 7% sodium bicarbonate; Luer-Lok syringes; Klein pump (mechanical infiltration pump - optional but preferred for even delivery) |
| Analgesia/sedation | Alprazolam 0.5 mg oral (pre-med); ibuprofen 600 mg (post-op); lorazepam 0.5-1 mg PRN |
| Wound/compression | Sterile drapes; povidone-iodine; sterile gloves; Class II (30-40 mmHg) thigh-high graduated compression stockings; skin marking pen |
Cost-Effective Alternatives with Similar Outcomes
| EVLA Standard | Lower-Cost Alternative | Evidence |
|---|---|---|
| 1470 nm radial fiber system (~$50,000-$120,000 capital) | 980 nm bare-tip system (~$15,000-$30,000) - similar occlusion rates (95-98%), slightly more bruising | Widely used; comparable 5-year outcomes |
| Radial disposable fibers (~$150-300 each) | Bare-tip fibers (~$30-60 each) - reuse protocols exist in some settings | 4-5x cost saving per case |
| Klein pump for tumescent | Manual syringe infiltration - equally effective, slower | Standard in most Indian centres |
| Portable high-end ultrasound ($30,000+) | Budget-range portable ultrasound (SonoSite, Mindray, Butterfly iQ; ~$5,000-$15,000) | Adequate for 2D guidance at 7-10 MHz |
| RFA (ClosureFast, Medtronic; high recurring catheter costs) | EVLA 980 nm bare-tip - EVLA is the more cost-effective thermal ablation option with equivalent outcomes; [Cochrane 2021, PMID 34378180] | |
| Mechanochemical ablation (MOCA, ClariVein) | EVLA 980 nm - MOCA at 5-year follow-up (LAMA trial 2025, PMID 40288564) showed no difference in outcomes; MOCA disposables also expensive | |
| Lowest cost approach with good results: | EVLA 980 nm bare-tip + manual tumescent + portable duplex + foam sclerotherapy for tributaries | Occlusion 94-98%, returnable to work same day |
8. COMPLICATIONS - PREVENTION & TREATMENT
Minor Complications (Common)
| Complication | Incidence | Prevention | Treatment |
|---|---|---|---|
| Bruising/ecchymosis | 7-57% (higher with 980 nm bare-tip) | Use 1470 nm radial fiber; adequate tumescence; Trendelenburg | Reassurance; NSAIDs; spontaneous resolution 2-4 weeks |
| Post-procedural pain along vein | Variable; lower with 1470 nm | 1470 nm radial fiber; adequate LEED; tumescent heat sink | NSAIDs; ibuprofen 600 mg TDS; spontaneous resolution |
| Superficial thrombophlebitis | 3-5% | Adequate energy delivery (avoid under-treatment); compression | NSAIDs; compression; warm compresses |
| Hyperpigmentation | Up to 10% | Minimize perivenous heating; do not treat too superficially | Mostly resolves; topical bleaching agents if persistent |
| Paresthesia (nerve injury - sensory) | 1.6-11% (mean ~4% for SSV; <5% for GSV) | Float vein ≥10 mm below skin; adequate tumescence around nerve; for SSV keep fiber >3 cm from SPJ | Reassurance; usually resolves within 2-3 months; never motor nerve damage |
| Induration along vein | Common | Expected part of fibrosis; adequate compression | Resolves over weeks to months |
Major Complications (Rare)
| Complication | Incidence | Prevention | Treatment |
|---|---|---|---|
| EHIT (Endothermal Heat-Induced Thrombosis) | Up to 9% any grade; Grade III 0.8% | Position tip ≥2 cm (GSV) / ≥3 cm (SSV) from deep junction; Trendelenburg; avoid high LEED near junction | AVF-EHIT Classification guides treatment: Class IA/IB (at junction only): no treatment or monitoring only. Class II (<5 mm into deep vein, <50%): weekly duplex; antiplatelet or prophylactic anticoagulation in high-risk patients. Class III (>50% of deep vein): therapeutic anticoagulation + weekly duplex until resolution. Class IV (total DVT): treat as provoked DVT per CHEST guidelines |
| DVT | <1-2% | Immediate ambulation; compression; short treatment times; avoid Trendelenburg prolonged; screen for thrombophilia pre-op | Therapeutic anticoagulation (LMWH/DOAC) per DVT protocol |
| Skin burn (full thickness) | 0.1-1.3% | Do not treat veins <10 mm below skin; adequate tumescent; avoid high energy near skin | Wound care; possible skin graft if severe; burns are preventable with adequate technique |
| Arteriovenous fistula | Very rare | Careful ultrasound identification of adjacent arteries (especially SSV artery) before injection/ablation | Observation (small) or surgical/endovascular closure |
| Pulmonary embolism | Very rare (<0.1%) | EHIT prevention; early ambulation | LMWH/DOAC; haematology involvement |
9. VEIN COMPARISON: GSV vs SSV vs Reticular/Giacomini Vein
Anatomy Recap
- GSV (Great Saphenous Vein): Medial leg/thigh; joins CFV at SFJ in groin; longest vein in body; causes medial varicose veins; most commonly treated
- SSV (Short/Small Saphenous Vein): Posterior calf; joins popliteal vein at SPJ (variable level); associated with posterior/lateral calf varices; close to sural nerve in distal calf
- Giacomini Vein: Thigh extension of SSV connecting to GSV; from SSV at popliteal fossa, runs posterolaterally in thigh. About 4% of patients have an incompetent Giacomini
- Reticular Veins: Intradermal/subdermal small (<3 mm), bluish-green veins; usually treated with sclerotherapy or transcutaneous laser; generally not suitable for EVLA (too small)
EVLA Outcomes Comparison
| Parameter | GSV | SSV | Giacomini Vein |
|---|---|---|---|
| EVLA suitability | Gold standard indication | Well-established (growing evidence) | Feasible; limited studies; usually combined with SSV treatment |
| Technical difficulty | Low-moderate | Moderate-high | High (variable anatomy) |
| Anatomic occlusion rate (EVLA) | 94-100% (1470 nm); 94-98% at 5 years | 94.3% mid-term; 94.3% long-term (PMID 40449724) | ~89-96% (small series; Korean series 100% at 980 nm EVLA PMID found) |
| Competing treatment occlusion | RFA 97-98%; MOCA 80-85%; UGFS 80-88% | RFA 98.4% short-term (best); EVLA 96.1% mid/long-term (best) | Foam sclerotherapy (UGFS) commonly used as alternative |
| Special safety concern | EHIT (position ≥2 cm from SFJ); preserve epigastric vein | Nerve injury (sural nerve; fibular/common peroneal nerve); SPJ identification; popliteal artery proximity | SSV artery companion; variable anatomy requires meticulous duplex mapping |
| Symptom relief | Excellent; most evidence; QoL scores best documented | Good; comparable to GSV after adequate treatment | Limited QoL data; symptomatic improvement reported |
| Recurrence | 5-year recurrence higher for EVLA vs RFA in one RCT (OR 2.77, 95% CI 1.52-5.06 favoring RFA at 5 years) | Long-term data limited; 33 studies in SSV review (PMID 37779391) | Insufficient long-term data |
| Key difference | SPJ is fixed at groin (predictable anatomy) | SPJ is variable (L3-L5); harder to locate; risk of treating wrong vein | Requires tracing from SSV; often dual-access needed |
| Nerve risk | Low (saphenous nerve, distal 1/3 leg) | Moderate-high (sural nerve average 4% paresthesia) | Posterior femoral cutaneous nerve; sensory only |
Which Vein is Most Important for Symptom Relief?
- EVLA vs RFA for GSV: technically equivalent success up to 5 years (OR 0.98); RFA may have slight benefit at 5 years
- EVLA vs UGFS for GSV: EVLA significantly superior technical success (OR 6.47 at >5 years)
- No direct RCT comparing GSV-EVLA vs SSV-EVLA for symptom relief (a genuine research gap)
10. STEPS THAT CAN BE MODIFIED BASED ON OUTCOME
| Step | Standard | Evidence-Based Modification |
|---|---|---|
| Wavelength selection | 980 nm (cheaper) | Upgrade to 1470 nm if post-op pain and bruising are major concerns (proven by multiple RCTs) |
| Fiber tip position (GSV) | 2 cm from SFJ | If EHIT occurs repeatedly, increase to 3 cm from SFJ |
| Energy delivery (LEED) | 40 J/cm (1470 nm) | If recanalization occurs at 3-month duplex, increase to 60-70 J/cm |
| Adjunct procedures | Wait 1 month after EVLA | If patient convenience is priority, do ambulatory phlebectomy/sclerotherapy same session (no inferior outcomes) |
| Compression duration | 7 days | Extended to 2 weeks if phlebitis develops; can reduce to 48 hours in select patients (2023 RCT evidence emerging) |
| SSV fiber tip position | 3 cm from SPJ | Increase to 5 cm if paresthesia occurs (sural nerve protection zone) |
| Post-op duplex follow-up | Day 3-7 | If EHIT Grade II found, weekly surveillance ultrasound until resolution |
| Power setting | 5-7 W | Reduce to 3-4 W for thin-walled SSV or small caliber veins to prevent perforation |
11. SCOPE OF RESEARCH IN EVLA - HOW TO IMPROVE IN INDIA
Current Research Gaps (Globally)
- No high-quality RCT comparing GSV vs SSV EVLA for symptom relief - most studies report technical occlusion, not patient-reported outcomes
- SSV studies are predominantly retrospective with low GRADE quality (confirmed PMID 40449724)
- Giacomini vein EVLA - only case series; no prospective comparative data
- Reticular vein EVLA - under-studied; mostly foam sclerotherapy used
- Optimal LEED for SSV in Indian population (different body habitus, BMI)
- Long-term data (>5 years) for 1470 nm radial fiber
- EVLA in CEAP C5-C6 disease (venous ulcer) - limited India-specific data
- Hybrid EVLA (trunk ablation + simultaneous phlebectomy/sclerotherapy) vs staged approach
- EHIT risk prediction models specific to Asian populations
How to Improve EVLA Practice in India
| Research Idea | Feasibility | Impact |
|---|---|---|
| Registry study: Multi-centre Indian EVLA outcomes registry (CEAP classification, VCSS, AVVQ QoL, 1/3/5-year follow-up) | High - needs institutional collaboration | Creates India-specific baseline data; publishable in JVS or Phlebology |
| RCT: 980 nm bare-tip vs 1470 nm radial fiber in Indian patients (powered for QoL endpoints, not just occlusion) | Moderate - needs two-arm setup | Directly answers cost vs benefit for Indian healthcare |
| SSV EVLA registry with sural nerve injury documentation | High - SSV treated far less than GSV in India | Fills a major evidence gap |
| Giacomini vein EVLA case series - prospective with 1-year duplex follow-up | High - feasible single-centre | First Indian prospective data on Giacomini |
| Cost-effectiveness study: EVLA 980 nm vs surgical stripping in Indian public hospitals | High | Policy-changing for national health programs (Ayushman Bharat) |
| Training study: EVLA learning curve in Indian trainees | Medium | Important for skill dissemination to tier-2/3 cities |
- Chinese-manufactured 980/1470 nm diode laser systems (e.g., Biolitec India distributor, WonTech, Eufoton) cost 60-70% less than US/European equivalents with similar specifications - proper evaluation needed
- Mindray/Sonosite portable duplex systems at ₹3-8 lakh are adequate for EVLA guidance (vs ₹20-40 lakh for high-end systems)
- Reusable fiber protocols (cleaned, re-sterilized bare-tip fibers) used in some Indian centres - needs formal safety evaluation
- Ultrasound-guided foam sclerotherapy (UGFS) for reticular and smaller tributaries: equipment cost near-zero; can be combined with EVLA for complete treatment in one session
- Training in high-volume government hospitals (AIIMS, PGI, teaching hospitals) to bring EVLA within reach of non-private sector patients
- India has an estimated 20-30% prevalence of varicose veins in working-age adults, making this a large public health opportunity - suitable for ICMR-funded multicentre trial
- Register studies at CTRI (Clinical Trials Registry India) before enrollment
- Target journals: Phlebology, Journal of Vascular Surgery: Venous and Lymphatic Disorders, Indian Journal of Surgery, Indian Journal of Vascular and Endovascular Surgery
- Partner with European societies (EVF - European Venous Forum) for collaborative data pooling
- Use validated Indian QoL tools alongside AVVQ/VCSS
REFERENCES
- Current Surgical Therapy 14e, Endovenous Laser Ablation of Truncal Veins, p.1238
- Pfenninger & Fowler's Procedures for Primary Care 3e, Endovenous Radiofrequency and Laser Ablation, p.573-576
- Whing J et al. Cochrane Database Syst Rev 2021 - Interventions for GSV incompetence (PMID 34378180)
- Tan J et al. Vasa 2023 - Systematic review: endovenous ablation for SSV (PMID 37779391)
- Oud S et al. Eur J Vasc Endovasc Surg 2026 - Network meta-analysis: SSV treatment modalities (PMID 40449724) - EVLA ranked superior at short-term; RFA at mid-term
- Bontinis V et al. J Vasc Surg Venous Lymphat Disord 2023 - Network meta-analysis: thermal vs non-thermal ablation (PMID 37030442)
- Lasers in Medical Science 2024 - 980 nm vs 1470 nm meta-analysis (3,193 truncal veins; 1470 nm superior occlusion + less paresthesia)
- Lim AJM et al. Eur J Vasc Endovasc Surg 2025 - LAMA trial 5-year follow-up EVLA vs MOCA (PMID 40288564)