Gastritis morphology, gross, types, etiology, clinical Symptoms, treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have all the information needed for a comprehensive response. Let me compile everything.
Gastritis: Complete Overview
Definition
Gastritis is a mucosal inflammatory process of the stomach. When inflammatory cells are absent or rare despite mucosal damage, the preferred term is gastropathy.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 720
Classification (Sydney System)
The most widely used classification (Updated Sydney System) categorizes chronic gastritis by topography, morphology, and etiology:
| Type | Etiology | Synonyms |
|---|---|---|
| Nonatrophic chronic gastritis | H. pylori, other factors | Chronic superficial gastritis, Type B gastritis, Diffuse antral gastritis |
| Atrophic - Autoimmune | Autoimmunity (± H. pylori) | Type A gastritis, Diffuse corporal gastritis, Pernicious anemia-associated |
| Atrophic - Multifocal | H. pylori + environmental | Type AB gastritis, Atrophic pangastritis |
| Reactive gastropathy | NSAIDs, bile reflux, alcohol | Chemical gastropathy |
| Lymphocytic gastritis | ? H. pylori, celiac disease | Varioliform gastritis |
| Granulomatous gastritis | Crohn disease, sarcoidosis, TB | - |
| Eosinophilic gastritis | Allergic, idiopathic | - |
- Yamada's Textbook of Gastroenterology, Table 51.1, p. 1081
A staging system called OLGA (Operative Link for Gastritis Assessment) adds detailed grading of glandular atrophy to predict gastric cancer risk.
Types of Gastritis
1. Acute Gastritis
A dense neutrophilic infiltration of the gastric mucosa. True acute neutrophilic gastritis is rare; most "active" gastritis is chronic inflammation with superimposed neutrophils (as in H. pylori infection).
Special severe forms:
-
Phlegmonous (suppurative) gastritis: infection of the gastric submucosa and muscularis propria; may spare mucosa. Organisms: gram-negative bacilli, anaerobes, group A streptococci, fungi (mucormycosis). Presents as a septic abdomen with peritonitis. Associated with alcohol binge, respiratory infections, AIDS, liver transplantation.
-
Emphysematous gastritis: caused by gas-producing organisms (Clostridium perfringens, E. coli, S. aureus); gas seen in stomach wall and portal venous system on CT. Risk factors include recent gastroduodenal surgery and ingestion of corrosives. May progress to gastric gas gangrene.
-
Sleisenger and Fordtran's GI and Liver Disease, p. 909
2. Chronic Gastritis - H. pylori (most common)
- Produces diffuse antral gastritis initially (nonatrophic pattern)
- With time can progress to multifocal atrophic gastritis (corpus + antrum)
- Associated with 70-80% of peptic ulcer disease and risk of gastric adenocarcinoma and MALToma
3. Chronic Gastritis - Autoimmune (Type A)
- Spares antrum; involves body and fundus
- Causes pernicious anemia; less than 10% of chronic gastritis; prevalence ~2% in patients >60 years
4. Environmental Metaplastic Atrophic Gastritis (EMAG)
- H. pylori + dietary/environmental factors (high-salt diet, smoking, carcinogens)
- Patchy involvement beginning at incisura, spreading to antrum and corpus
5. Special/Distinctive Forms
- Lymphocytic gastritis, Collagenous gastritis, Eosinophilic gastritis, Granulomatous gastritis (Crohn, sarcoid, TB), Infectious gastritis (CMV, fungal, parasitic)
Etiology
| Category | Agents |
|---|---|
| Bacterial | H. pylori (most common), H. heilmannii, streptococcal (phlegmonous), Clostridium (emphysematous), TB, syphilis |
| Viral | CMV (especially immunocompromised), HSV, EBV |
| Fungal | Mucormycosis, Aspergillus, Cryptococcus (immunocompromised) |
| Parasitic | Strongyloides, Anisakis, Giardia, Cryptosporidiosis |
| Drugs/Chemicals | NSAIDs (most common after H. pylori), aspirin, alcohol, bile reflux |
| Autoimmune | Anti-parietal cell antibodies (anti-H+/K+-ATPase), anti-intrinsic factor antibodies |
| Systemic diseases | Crohn disease, sarcoidosis, amyloidosis, graft-versus-host disease |
| Physical | Radiation injury, nasogastric tube trauma, stress |
| Iatrogenic | Immune checkpoint inhibitors (nivolumab can cause autoimmune hemorrhagic gastritis) |
- Robbins, Cotran & Kumar, p. 714-720; Sleisenger & Fordtran, p. 908-910
Gross Morphology
Acute Gastritis / Stress Ulcers
- Mucosal hyperemia, edema, and congestion
- Erosions (superficial) to frank ulcers; ulcers typically < 1 cm, rounded, base stained brown-black by acid digestion of blood
- Lesions are multiple and distributed throughout the stomach (unlike peptic ulcers which are usually solitary/antral)
- Phlegmonous gastritis: thick, edematous gastric wall, multiple perforations, granular/purulent mucosa, mucosal hemorrhage and necrosis
H. pylori Chronic Gastritis
- Antral mucosa appears erythematous, coarse, or nodular (endoscopic "chicken-skin" appearance = nodular gastritis)
- In dense colonization, rugal folds can appear thickened
Autoimmune Atrophic Gastritis
- Fundus/body mucosa appears markedly thinned
- Rugal folds are lost (flattening)
- Residual islands of oxyntic mucosa may appear as small polyps or nodules endoscopically
Multifocal Atrophic Gastritis
-
Patchy mucosal atrophy beginning at incisura, extending to antrum and corpus
-
Grayish-white or pale mucosa where normal reddish glandular epithelium has been replaced by intestinal metaplasia
-
Sleisenger & Fordtran, pp. 908-914; Robbins, pp. 715-716
Microscopic Morphology (Histology)
H. pylori Gastritis
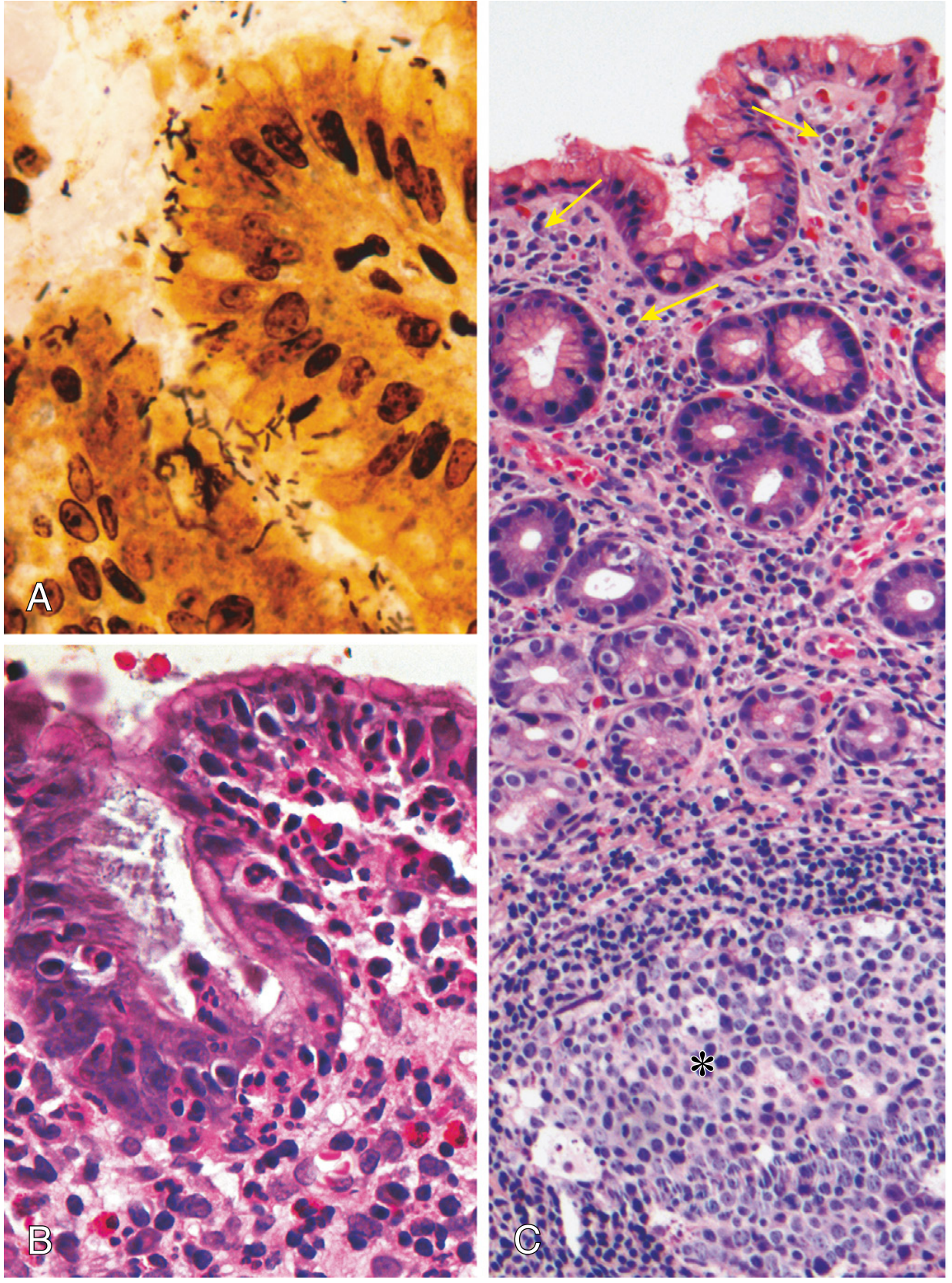
Fig. A: Warthin-Starry silver stain showing spiral H. pylori organisms in surface mucus. B: Intraepithelial and lamina propria neutrophils forming pit abscesses. C: Lymphoid aggregates with germinal centers (asterisk) and subepithelial plasma cells (arrows). - Robbins Pathology
Key features:
- Neutrophils infiltrate gastric pits - "pit abscesses"
- Plasma cells in clusters within superficial lamina propria
- Lymphoid aggregates with germinal centers (MALT induction)
- H. pylori organisms visible in superficial mucus on H&E; best seen with Warthin-Starry silver stain or immunostains
- "Active" chronic gastritis: both neutrophils and chronic cells (lymphocytes, plasma cells) coexist
Autoimmune Atrophic Gastritis
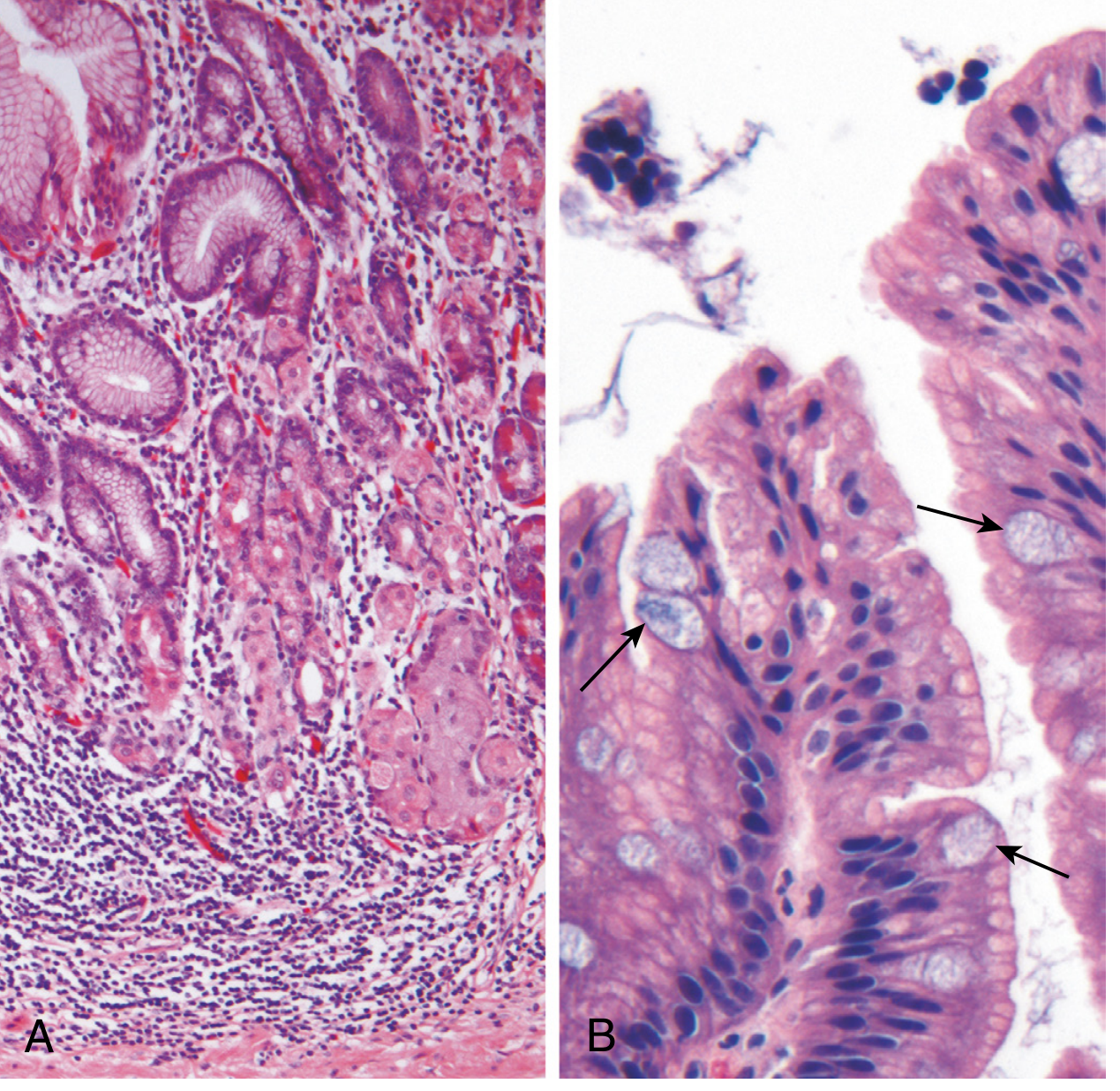
Fig. A: Deep inflammatory infiltrate centered on gastric glands with atrophy. B: Intestinal metaplasia - goblet cells (arrows) within gastric foveolar epithelium. - Robbins Pathology
Key features:
- Deep inflammation centered on gastric glands (not superficial lamina propria as in H. pylori)
- Infiltrate: lymphocytes, macrophages, plasma cells - no prominent neutrophils
- Loss of parietal and chief cells in body/fundus
- Intestinal metaplasia: goblet cells, absorptive cells, Paneth cells
- Enterochromaffin-like (ECL) cell hyperplasia and neuroendocrine hyperplasia
- May progress to multicentric low-grade neuroendocrine tumors (gastric carcinoids)
Common to All Chronic Forms
-
Intestinal metaplasia (goblet cells in gastric epithelium) - risk factor for gastric adenocarcinoma
-
Dysplasia may develop as precancerous change
-
Robbins, pp. 715-717; Yamada's, pp. 1874-1887
Comparison: H. pylori vs. Autoimmune Gastritis
| Feature | H. pylori-Associated | Autoimmune |
|---|---|---|
| Location | Antrum (initially) | Body/Fundus |
| Inflammatory infiltrate | Neutrophils + plasma cells | Lymphocytes, macrophages |
| Acid production | Increased to slightly decreased | Decreased (achlorhydria) |
| Gastrin secretion | Normal to increased | Markedly increased |
| Other lesions | Hyperplastic/inflammatory polyps | Neuroendocrine (ECL) hyperplasia |
| Serology | Anti-H. pylori antibodies | Anti-parietal cell (H+/K+-ATPase), anti-intrinsic factor antibodies |
| Sequelae | Peptic ulcer, adenocarcinoma, MALToma | Pernicious anemia, adenocarcinoma, gastric carcinoid |
| Associations | Low socioeconomic status, poverty, rural areas | Hashimoto thyroiditis, Type 1 DM, Addison disease, Graves disease |
- Robbins, Table 17.2, p. 716
Pathogenesis of H. pylori Gastritis
H. pylori is a gram-negative, helical/spiral-shaped, flagellated bacterium infecting >50% of the world's population (70-80% in developing nations).
Key virulence factors:
- Urease - hydrolyzes urea to NH3, neutralizing local acid; essential for colonization
- Adhesins - facilitate mucosal adherence
- CagA pathogenicity island - injected into epithelial cells; activates signaling, structural remodeling; present in 90% of isolates in high-gastric-cancer-risk populations; associated with body colonization, atrophy, and intestinal metaplasia
- VacA (vacuolating cytotoxin A) - causes epithelial vacuolization and barrier disruption
- HP-NAP (neutrophil activating protein)
- LPS, Oip A, peptidoglycan - inflammatory mediators
Outcomes depend on interplay of:
-
Host genetic polymorphisms (IL-1, TNF, IL-10)
-
Bacterial virulence (CagA+, VacA s1m1 strains)
-
Environmental factors (smoking, high-salt diet, refrigeration access)
-
Robbins, p. 715; Sleisenger & Fordtran, p. 914
Clinical Symptoms
Acute Gastritis
- Often asymptomatic
- Epigastric pain or burning
- Nausea and vomiting
- Hematemesis (if erosions/stress ulcers)
- Severe forms (phlegmonous/emphysematous): acute abdomen, sepsis, fever, hypotension, peritonitis, purulent ascitic fluid
Chronic Gastritis (General)
- Typically less severe but more persistent than acute
- Nausea and upper abdominal discomfort/pain (most common)
- Vomiting (less frequent)
- Hematemesis - uncommon
- Bloating and belching
- Significant weight loss (particularly if atrophic)
H. pylori Gastritis Specifically
- Many patients are asymptomatic
- May present only when complications arise (peptic ulcer, GI bleeding)
Autoimmune Atrophic Gastritis Specifically
-
Symptoms develop slowly over 2-3 decades
-
Pernicious anemia: fatigue, pallor, glossitis, neurological symptoms (subacute combined degeneration of the cord - due to B12 deficiency)
-
Achlorhydria symptoms: poor digestion
-
Increased risk of gastric carcinoid tumors
-
Robbins, pp. 715-720; Sleisenger & Fordtran, p. 909
Diagnosis
| Test | Type | Notes |
|---|---|---|
| Urea breath test | Non-invasive, indirect | Detects urease activity; sensitive and specific |
| Stool antigen test | Non-invasive, direct | Good for post-treatment confirmation |
| Serology (IgG anti-H. pylori) | Non-invasive | Cannot distinguish active from past infection |
| Biopsy urease test (CLO test) | Endoscopic | Fast, inexpensive |
| Histology (H&E ± Warthin-Starry) | Endoscopic | Gold standard; shows morphology + organisms |
| Culture | Endoscopic | Allows sensitivity testing; low sensitivity |
| PCR | Endoscopic | High sensitivity; detects resistance genes |
For autoimmune gastritis: serum anti-parietal cell antibodies (anti-H+/K+-ATPase), anti-intrinsic factor antibodies (present in up to 80%), reduced serum pepsinogen I.
- Sleisenger & Fordtran, p. 913-914
Treatment
Acute Gastritis / Stress Ulcers
- Remove/treat the underlying cause (most effective approach)
- Proton pump inhibitors (PPIs) - prophylactic in critically ill ICU patients
- Healing with complete re-epithelialization occurs within days to weeks after treatment
- Supportive care: IV fluids, antiemetics
H. pylori Eradication (Chronic Gastritis / Peptic Ulcer Disease)
First-line regimens:
- Triple therapy: PPI + Clarithromycin + Amoxicillin (or Metronidazole) for 14 days
- Bismuth quadruple therapy: PPI + Bismuth + Tetracycline + Metronidazole (used in areas of high clarithromycin resistance)
Goals: eradication, mucosal healing, prevention of complications. After successful H. pylori eradication, peptic ulcer recurrence rate is less than 20%.
Autoimmune Atrophic Gastritis
- No curative treatment (autoimmune process)
- Vitamin B12 replacement (intramuscular injections monthly, or high-dose oral supplementation)
- Iron supplementation as needed
- Endoscopic surveillance for gastric carcinoid and adenocarcinoma
- Treat any coexisting autoimmune conditions
NSAIDs / Reactive Gastropathy
- Discontinue the offending NSAID (including selective COX-2 inhibitors)
- PPI therapy for mucosal healing
- If NSAIDs must continue: use lowest effective dose + PPI co-therapy
Granulomatous Gastritis (Sarcoidosis)
- Glucocorticoid therapy (cornerstone)
- Subtotal gastric resection reserved for obstruction or severe hemorrhage
Phlegmonous/Emphysematous Gastritis
-
Broad-spectrum IV antibiotics (covers gram-negative bacilli, anaerobes, gram-positive cocci)
-
Surgical resection/drainage may be necessary
-
Mucormycosis: resection of affected necrotic stomach; anti-fungal therapy (amphotericin B)
-
Robbins, p. 715, 720; Sleisenger & Fordtran, pp. 905-912; Harrison's Principles of Internal Medicine 22E
Complications of Chronic Gastritis
- Peptic Ulcer Disease - usually H. pylori-induced hyperchlorhydria
- Gastric Adenocarcinoma - via intestinal metaplasia → dysplasia → cancer (Correa cascade); risk greatest in autoimmune metaplastic atrophic gastritis
- MALToma (MALT Lymphoma) - B-cell lymphoma arising from H. pylori-induced MALT; can regress with H. pylori eradication
- Pernicious Anemia - autoimmune atrophic gastritis; megaloblastic anemia from B12 deficiency
- Gastric Neuroendocrine Tumors (Carcinoids) - ECL cell hyperplasia driven by hypergastrinemia in autoimmune gastritis
- Dysplasia - intermediate precancerous lesion
- Robbins, pp. 720-722
Key Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (pp. 713-722) | Sleisenger and Fordtran's GI and Liver Disease (pp. 908-920) | Yamada's Textbook of Gastroenterology (pp. 1080-1087) | Harrison's Principles of Internal Medicine 22E
Give me the details about gastritis
The detailed overview I just provided covers all the key aspects of gastritis. Here is a structured summary of everything covered:
Gastritis - Complete Details
1. Definition
Gastritis is a mucosal inflammatory process of the stomach. When mucosal damage occurs without significant inflammation, the preferred term is gastropathy.
2. Classification (Updated Sydney System)
Based on topography, morphology, and etiology:
| Type | Etiology | Old Name |
|---|---|---|
| Nonatrophic chronic gastritis | H. pylori | Type B gastritis |
| Autoimmune atrophic gastritis | Autoimmunity | Type A gastritis |
| Multifocal atrophic gastritis | H. pylori + environment | Type AB gastritis |
| Reactive gastropathy | NSAIDs, bile reflux | Chemical gastropathy |
| Lymphocytic gastritis | H. pylori, celiac | Varioliform gastritis |
| Granulomatous gastritis | Crohn, sarcoidosis, TB | - |
| Eosinophilic gastritis | Allergic, idiopathic | - |
The OLGA staging system adds detailed atrophy grading to estimate gastric cancer risk.
3. Types
A. Acute Gastritis
- Dense neutrophilic infiltration of mucosa
- True acute gastritis is rare; "active" gastritis = neutrophils superimposed on chronic inflammation
Severe subtypes:
| Subtype | Features |
|---|---|
| Phlegmonous gastritis | Infection of submucosa/muscularis propria; organisms: gram-negative bacilli, streptococci, anaerobes, fungi |
| Emphysematous gastritis | Gas-producing organisms (C. perfringens, E. coli, S. aureus); gas in stomach wall + portal venous gas on CT; may progress to gastric gangrene |
B. Chronic Gastritis - H. pylori (Most Common)
- Starts as diffuse antral gastritis
- Progresses to multifocal atrophic gastritis
- Risk of peptic ulcer, adenocarcinoma, MALToma
C. Autoimmune Atrophic Gastritis (Type A)
- Body and fundus only (antrum spared)
- Anti-parietal cell + anti-intrinsic factor antibodies
- Leads to pernicious anemia, gastric carcinoids
D. Multifocal Atrophic Gastritis (EMAG)
- H. pylori + environmental cofactors (salt, smoking)
- Begins at incisura, spreads to antrum and corpus
E. Special/Distinctive Forms
- Lymphocytic gastritis - thick folds, varioliform erosions; associated with celiac, H. pylori
- Collagenous gastritis - subepithelial collagen band > 20 µm
- Eosinophilic gastritis - eosinophil-dominant infiltrate; allergic or idiopathic
- Granulomatous gastritis - non-caseating granulomas; Crohn, sarcoidosis, TB
- CMV gastritis - immunocompromised patients; intranuclear "owl-eye" inclusions
4. Etiology
| Category | Agents |
|---|---|
| Bacterial | H. pylori (#1), TB, syphilis, streptococcal, Clostridium |
| Viral | CMV, HSV, EBV |
| Fungal | Mucormycosis, Aspergillus, Cryptococcus |
| Parasitic | Strongyloides, Anisakis, Giardia |
| Drugs | NSAIDs, aspirin, alcohol, corticosteroids |
| Autoimmune | Anti-H+/K+-ATPase, anti-intrinsic factor Ab |
| Physical | Radiation, NG tube trauma, stress (Curling/Cushing ulcers) |
| Systemic | Crohn disease, sarcoidosis, amyloidosis, GVHD |
| Iatrogenic | Immune checkpoint inhibitors (nivolumab) |
| Bile reflux | Post-gastrectomy, pyloric dysfunction |
5. Gross Morphology
Acute Gastritis
- Mucosal hyperemia, edema, congestion
- Superficial erosions to frank ulcers
- Ulcers < 1 cm, rounded, base stained brown-black by acid digestion of blood
- Multiple throughout stomach (vs. peptic ulcers - usually solitary/antral)
- Phlegmonous: thick, edematous wall with granular/purulent mucosa and necrosis
H. pylori Chronic Gastritis
- Antrum appears erythematous, coarse, or nodular endoscopically
- "Chicken-skin" (nodular gastritis) - visible on endoscopy
Autoimmune Atrophic Gastritis
- Fundus/body mucosa thinned, rugal folds lost
- Residual oxyntic islands may look like small polyps/nodules endoscopically
- Pale, atrophic appearance
Multifocal Atrophic Gastritis
- Patchy pale/white mucosa at incisura spreading outward
- Areas of intestinal metaplasia appear grayish-white
6. Microscopic Morphology (Histology)
H. pylori Gastritis
| Feature | Detail |
|---|---|
| H. pylori location | Superficial mucus layer, gastric pit lumens |
| Best stain | Warthin-Starry silver stain or immunostain |
| Neutrophils | Infiltrate gastric pits - "pit abscesses" |
| Lamina propria | Plasma cells in clusters, lymphocytes, macrophages |
| Lymphoid tissue | Lymphoid aggregates with germinal centers = MALT |
| Active gastritis | Neutrophils + chronic cells simultaneously |
Autoimmune Atrophic Gastritis
| Feature | Detail |
|---|---|
| Inflammation location | Deep - centered on gastric glands (not superficial) |
| Cell types | Lymphocytes, macrophages, plasma cells - no neutrophils |
| Glandular changes | Loss of parietal and chief cells |
| Metaplasia | Intestinal metaplasia - goblet cells, absorptive cells, Paneth cells |
| Endocrine changes | ECL cell hyperplasia; may form multicentric carcinoid tumors |
| Megaloblastic change | Nuclear enlargement in epithelial cells if severe B12 deficiency |
Common to All Chronic Gastritis
- Intestinal metaplasia - goblet cells in gastric epithelium; risk factor for adenocarcinoma
- Dysplasia - nuclear pleomorphism, loss of polarity; precancerous
7. H. pylori vs. Autoimmune Gastritis - Comparison
| Feature | H. pylori | Autoimmune |
|---|---|---|
| Location | Antrum (initially) | Body/Fundus |
| Inflammatory cells | Neutrophils + plasma cells | Lymphocytes + macrophages |
| Acid production | Increased to slightly decreased | Decreased (achlorhydria) |
| Gastrin | Normal to increased | Markedly increased (hypergastrinemia) |
| Serology | Anti-H. pylori Ab | Anti-H+/K+-ATPase, anti-IF Ab |
| Other lesions | Hyperplastic polyps | ECL hyperplasia, carcinoids |
| Complications | Peptic ulcer, adenocarcinoma, MALToma | Pernicious anemia, adenocarcinoma, carcinoid |
| Associations | Low socioeconomic status, poverty, rural | Hashimoto thyroiditis, Type 1 DM, Addison, Graves |
8. Pathogenesis of H. pylori
H. pylori is a gram-negative, helical, flagellated bacterium infecting >50% of the world's population.
Key virulence factors:
| Factor | Function |
|---|---|
| Urease | Splits urea → NH3; neutralizes local acid; essential for survival |
| Adhesins | Mucosal attachment |
| CagA (pathogenicity island) | Injected into epithelial cells; activates oncogenic signaling; present in 90% of isolates in high-cancer-risk populations |
| VacA | Epithelial vacuolization, barrier disruption |
| HP-NAP | Neutrophil activation, oxidative burst |
| LPS | Weak immunostimulant; Lewis Ag mimicry causes molecular mimicry with gastric epithelium |
Host factors: IL-1, TNF-α polymorphisms → increased pro-inflammatory cytokines → pangastritis, atrophy, cancer progression
Environmental modifiers: High-salt diet, smoking, lack of refrigeration accelerate progression
9. Clinical Symptoms
Acute Gastritis
- Often asymptomatic
- Epigastric burning or pain
- Nausea and vomiting
- Hematemesis (with erosions/ulcers)
- Severe forms: acute abdomen, sepsis, fever, hypotension, peritonitis
Chronic Gastritis
- Symptoms less severe but persistent
- Nausea, upper abdominal discomfort/pain
- Vomiting (less common)
- Bloating, belching
- Significant weight loss in atrophic forms
- Hematemesis - uncommon
Autoimmune Gastritis Specifically
- Slow progression over decades
- Pernicious anemia: fatigue, pallor, glossitis, neurological deficits (subacute combined degeneration due to B12 deficiency)
- Achlorhydria: impaired digestion
- Signs of associated autoimmune diseases
10. Diagnosis
| Test | Method | Notes |
|---|---|---|
| Urea breath test | Non-invasive | Detects active urease; gold standard non-invasive test |
| Stool antigen test | Non-invasive | Best for post-treatment confirmation |
| Serology (IgG) | Non-invasive | Cannot confirm active vs. past infection |
| Biopsy urease (CLO test) | Endoscopic | Fast, inexpensive, accurate |
| Histology (H&E + Warthin-Starry) | Endoscopic | Definitive; shows organisms + morphology |
| Culture + sensitivity | Endoscopic | Guides antibiotic choice in resistant cases |
| PCR | Endoscopic | High sensitivity; detects antibiotic resistance genes |
| Anti-parietal cell Ab | Blood test | For autoimmune gastritis; positive in up to 80% |
| Serum pepsinogen I | Blood test | Reduced in atrophic gastritis |
Sydney system requires 5-site biopsy protocol: antrum (greater + lesser curvature), corpus (greater + lesser curvature), and incisura.
11. Treatment
Acute Gastritis / Stress Ulcers
- Treat the underlying cause (most effective)
- PPI prophylaxis in critically ill ICU patients
- IV fluids, antiemetics, supportive care
- Healing in days to weeks after removing offending agent
H. pylori Eradication
| Regimen | Drugs | Duration |
|---|---|---|
| Triple therapy (1st line) | PPI + Clarithromycin + Amoxicillin | 14 days |
| Alternative triple | PPI + Clarithromycin + Metronidazole | 14 days |
| Bismuth quadruple (resistance areas) | PPI + Bismuth + Tetracycline + Metronidazole | 10-14 days |
After successful eradication: peptic ulcer recurrence < 20% (previously notoriously difficult)
Autoimmune Atrophic Gastritis
- No cure (autoimmune)
- Vitamin B12 replacement - IM injections monthly or high-dose oral (1000 µg/day)
- Iron supplementation
- Endoscopic surveillance for carcinoid tumors and adenocarcinoma
NSAIDs/Chemical Gastropathy
- Discontinue NSAIDs (including COX-2 inhibitors)
- PPI for healing
- If NSAIDs unavoidable: lowest dose + PPI co-therapy
Granulomatous Gastritis (Sarcoidosis)
- Glucocorticoids (cornerstone)
- Surgery only for obstruction or severe hemorrhage
Phlegmonous/Emphysematous Gastritis
- Broad-spectrum IV antibiotics (gram-negative, anaerobic, gram-positive coverage)
- Surgical resection/drainage for severe cases
- Mucormycosis: resection + amphotericin B
12. Complications
| Complication | Mechanism | Notes |
|---|---|---|
| Peptic Ulcer Disease | H. pylori-induced hyperchlorhydria | Stomach or duodenum |
| Gastric Adenocarcinoma | Intestinal metaplasia → dysplasia → cancer (Correa cascade) | Risk greatest in AMAG |
| MALToma | H. pylori-induced MALT → B-cell lymphoma | Can regress with H. pylori eradication alone |
| Pernicious Anemia | Autoimmune loss of intrinsic factor → B12 deficiency → megaloblastic anemia | AMAG-specific |
| Gastric Carcinoid Tumors | ECL hyperplasia from hypergastrinemia | AMAG-specific; usually low-grade |
| Dysplasia | Inflammation-driven genetic alterations | Precancerous; requires surveillance |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Sleisenger and Fordtran's GI and Liver Disease | Yamada's Textbook of Gastroenterology, 7th Ed. | Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.