Papilledema and bp
Reading File
Finding Sources
Finding Sources
Searching PubMed
papilledema hypertension intracranial pressure
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content. Here is a full, synthesized answer.
Papilledema and Blood Pressure
What is Papilledema?
Papilledema refers specifically to optic disc edema secondary to raised intracranial pressure (ICP). It is not a generic term for any disc swelling - the cause must be elevated ICP. The mechanism: raised ICP blocks axoplasmic flow in optic nerve fibers, increasing axoplasm volume at the disc. - Bradley and Daroff's Neurology in Clinical Practice
The Retinal Fundus in Papilledema
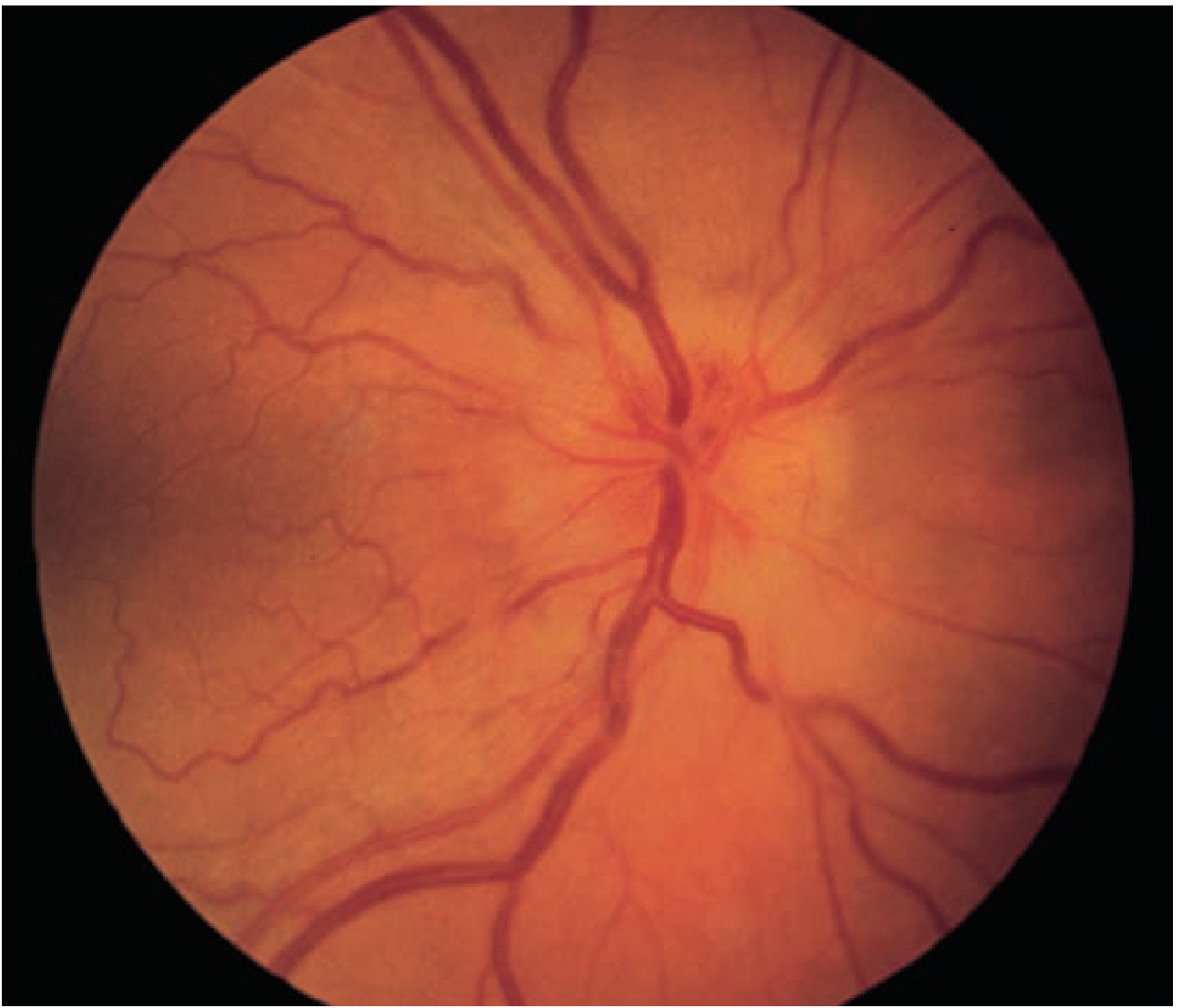
Fundus appearance showing vascular congestion, elevation of the nerve head, and blurred disc margins characteristic of papilledema - Tintinalli's Emergency Medicine
Stages of Papilledema
| Stage | Key Features |
|---|---|
| 1. Early | Minimal disc hyperemia, capillary dilation; mild nerve fiber layer opacification; absence of venous pulsations; peripapillary hemorrhage |
| 2. Fully developed | Engorged/tortuous veins; disc surface grossly elevated; cotton-wool spots; Paton lines (circumferential retinal folds); macular exudates or star |
| 3. Chronic (weeks-months) | Pale, gliotic disc; "champagne cork" appearance; pseudodrusen (extruded axoplasm); hemorrhages resolve; collateral optociliary vessels may appear |
| 4. Atrophic | Optic atrophy; severe irreversible visual loss |
- Localization in Clinical Neurology, 8e and Bradley and Daroff's Neurology
Clinical Features
- Usually bilateral (may be asymmetric due to variation in optic nerve subarachnoid septations)
- Visual acuity preserved early - a distinguishing hallmark; patients may be visually asymptomatic initially
- Transient visual obscurations (seconds-long visual loss)
- Visual field defects: enlarged blind spot (earliest), arcuate defects (typically inferonasal), concentric constriction
- No afferent pupillary defect unless disc edema is severe and asymmetric
- Absent spontaneous venous pulsations on fundoscopy (SVPs present = ICP likely normal)
- Fluorescein angiography: disc capillary dilation, dye leakage, microaneurysms
Causes - Including Hypertension
Primary causes of raised ICP (and thus papilledema):
- Idiopathic intracranial hypertension (IIH / pseudotumor cerebri)
- Mass lesions (tumor, hemorrhage, abscess, large infarction)
- Hydrocephalus
- Meningitis/encephalitis
- Subarachnoid hemorrhage
Hypertension and papilledema - two key relationships:
1. Malignant (Hypertensive Emergency) - BP causing disc edema
A marked elevation in blood pressure (typically >180/120 mmHg) can produce bilateral optic disc edema that is indistinguishable from papilledema. This is a hypertensive emergency. Associated findings include:
- Peripapillary cotton-wool spots
- Retinal hemorrhages
- Hypertensive encephalopathy / PRES (posterior reversible encephalopathy syndrome)
- Vision loss
"The changes associated with malignant hypertension can occur at lower blood pressures in patients with renal failure." - Bradley and Daroff's Neurology
The mechanism here involves both direct end-organ damage to retinal vasculature AND elevated ICP from PRES/encephalopathy.
2. Idiopathic Intracranial Hypertension (IIH) - raised ICP causing papilledema
This is a separate condition where ICP rises without a mass lesion or vascular cause. IIH is a primary cause of papilledema. Obesity and female sex are major risk factors. BP can be normal.
Papilledema vs. Pseudopapilledema
| Feature | Papilledema | Pseudopapilledema (e.g. drusen) |
|---|---|---|
| Disc color | Hyperemic | Pink/yellowish-pink |
| Disc margins | Indistinct (superior/inferior poles first) | Usually distinct, may be lumpy |
| Vessels | Normal distribution, SVPs absent | Emanate from center, anomalous pattern |
| Nerve fiber layer | Dull, edematous, obscures vessels | No edema; may glisten |
| Hemorrhages | Splinter type | Subretinal/retinal/vitreous |
Management
Treat the underlying cause:
- Hypertensive emergency: controlled reduction of BP (avoid over-rapid drop to prevent ischemia); IV agents in ICU setting
- IIH: weight loss, acetazolamide (reduces CSF production); in progressive visual loss - optic nerve sheath fenestration or CSF shunting
- Serial visual field monitoring for all cases with papilledema
Recent Evidence (2024-2026)
A 2025 meta-analysis (PMID: 40937960) found GLP-1 and dual GIP/GLP-1 receptor agonists (e.g., semaglutide) to be efficacious and safe in IIH - relevant given the obesity-IIH-hypertension overlap. A 2025 consensus statement (PMID: 38431253) from the Spanish Society of Neurology provides updated diagnostic and treatment criteria for disorders of intracranial pressure.
Key clinical pearl: In a hypertensive patient with bilateral disc edema, always consider whether the disc swelling reflects (a) direct hypertensive retinopathy/malignant hypertension, or (b) raised ICP from an underlying cause unrelated to BP. The distinction requires neuroimaging and BP measurement together.
This is a shared conversation. Sign in to Orris to start your own chat.