Indications, steps and complications of distal radical gastrectomy. [3+4+3]
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have very rich content. Let me compile a thorough, well-structured answer based on the textbook material (Fischer's Mastery of Surgery and Bailey & Love).
Distal Radical Gastrectomy - Indications, Steps, and Complications
(Based on Fischer's Mastery of Surgery 8e and Bailey & Love's Short Practice of Surgery 28e)
INDICATIONS [3 marks]
Malignant (primary indication for "radical" gastrectomy):
-
Gastric adenocarcinoma of the distal third - the most common indication. Distal gastrectomy is performed when the tumor is in the distal stomach and an adequate proximal margin can be achieved.
- NCCN recommends subtotal gastrectomy for T1b-T3 tumors when microscopic-free margins plus lymphadenectomy can be achieved
- Japanese guidelines extend this to cT2-T4a tumors (with or without node positivity) when a satisfactory proximal resection margin can be obtained
- Required margins: >4 cm (NCCN) or 3 cm for Borrmann type 1/2 and 5 cm for type 3/4 (Japanese/Chinese guidelines); 2 cm for T1 tumors
-
Gastric MALT lymphoma confined to distal stomach (after failure of H. pylori eradication)
-
Gastrointestinal stromal tumor (GIST) originating from Cajal cells in the distal stomach
Benign (historical / selected cases):
-
Complicated peptic ulcer disease - surgery is now reserved for peptic stenosis (gastric outlet obstruction), penetrating or perforated ulcers, and bleeding refractory to medical and endoscopic therapy (peptic ulcer disease has largely been replaced by H. pylori eradication therapy)
-
Other benign lesions in the distal stomach: leiomyoma, gastric lipoma, adenomyoma, juvenile polyposis
Contraindications (relative): hereditary diffuse gastric cancer (requires total gastrectomy), linitis plastica extending to the proximal stomach, peritoneal metastases.
STEPS OF DISTAL RADICAL GASTRECTOMY [4 marks]
Preoperative Preparation
- Upper GI endoscopy (EGD) + CT triphasic scan for staging; FDG-PET/CT for >T2 or node-positive disease
- Correct electrolyte imbalances (CBC + CMP); pre-operative optimization
- Prophylactic antibiotics at skin incision; DVT prophylaxis (IPC devices + pharmacologic)
- Nasogastric tube for gastric decompression; 12-hour fast (longer if gastric outlet obstruction)
Positioning and Access
- Supine position; midline laparotomy (or laparoscopic/robotic ports)
- Diagnostic laparoscopy first to exclude peritoneal spread in all patients undergoing potentially curative resection
- Inspect abdomen for ascites and metastatic deposits before committing to resection
Step 1 - Greater Omentum and Greater Curvature Dissection
- The transverse colon is completely separated from the greater omentum
- The gastrocolic ligament is divided; the greater omentum is removed en bloc with the specimen
- The right gastroepiploic vessels are identified, divided, and ligated at their origin
Step 2 - Subpyloric and Infrapyloric Lymph Node Dissection
- Subpyloric (station 6) lymph nodes are dissected
- The right gastric artery is divided at its origin from the proper hepatic artery
- Suprapyloric (station 5) nodes along the hepatic artery are cleared
Step 3 - Division of the Duodenum
- The first part of the duodenum is divided just beyond the pylorus, usually with a linear surgical stapler
- The duodenal stump is secured; if necessary, the duodenum is Kocherized to allow tension-free anastomosis
Step 4 - Left Gastric Artery and D2 Lymphadenectomy
- Dissection along the lesser omentum toward the celiac axis
- D1 dissection: perigastric nodes (stations 1-6)
- D2 dissection (standard for curative intent): additionally clears nodes along the left gastric artery (station 7), common hepatic artery (station 8), celiac axis (station 9), and splenic artery (station 11)
- The left gastric artery is divided at its origin from the celiac trunk
- NCCN: goal of examining >16 lymph nodes; D2 recommended at high-volume centers
Step 5 - Proximal Gastric Transection
- The stomach is divided proximally with a linear stapler at least 4 cm (NCCN) or 3-5 cm (Japanese) from the gross tumor edge
- Frozen section analysis of the proximal margin is performed if margin clearance is in doubt
Step 6 - Reconstruction
Three main options:
| Method | Description | Notes |
|---|---|---|
| Billroth I (gastroduodenostomy) | Gastric remnant anastomosed end-to-end or end-to-side to duodenum | Most physiologic; requires tension-free anastomosis; at least 3 cm from staple line to avoid ischemia; Kocherize duodenum to reduce tension |
| Billroth II (gastrojejunostomy) | Gastric remnant anastomosed to proximal jejunum (retrocolic or antecolic); duodenum closed as blind stump | Risk of alkaline reflux gastritis; Braun enteroenterostomy reduces afferent loop problems |
| Roux-en-Y gastrojejunostomy | Divided jejunum brought up; alimentary limb ≥50 cm to prevent bile reflux | Preferred when BI not possible; prevents alkaline reflux; increasing preference in gastric cancer |
COMPLICATIONS [3 marks]
Intraoperative
- Hemorrhage - injury to right gastric, right gastroepiploic, or left gastric vessels; splenic injury during mobilization
- Pancreatic injury during lymph node dissection (D2 dissection along the superior border of the pancreas)
- Bile duct injury during hepatic hilar dissection
Early Postoperative
- Anastomotic leak - the most feared early complication; presents with fever, tachycardia, peritonitis; duodenal stump blowout (Billroth II) is particularly dangerous
- Duodenal stump leak (after Billroth II) - can cause bile peritonitis, sepsis
- Intra-abdominal abscess - subphrenic or sub-hepatic
- Postoperative hemorrhage - intraluminal (anastomotic) or intra-abdominal
- Delayed gastric emptying / gastroparesis - especially after vagotomy or in patients with pre-existing gastric outlet obstruction
- Pancreatitis - from traction or dissection trauma to the pancreas
- Pulmonary complications - pneumonia, atelectasis (common in elderly; >70% have ≥2 comorbidities)
- DVT / Pulmonary embolism - moderate-to-high risk; requires prophylaxis
Late Postoperative
- Anastomotic stricture - causing dysphagia or outlet obstruction
- Marginal (stomal) ulceration - at the gastrojejunal anastomosis (Billroth II/Roux-en-Y), especially without adequate acid reduction
- Dumping syndrome - early (vasomotor symptoms from rapid gastric emptying) or late (reactive hypoglycemia)
- Alkaline reflux gastritis - bilious reflux into gastric remnant, particularly with Billroth II; presents with postprandial epigastric pain and bilious vomiting; treated by conversion to Roux-en-Y
- Afferent loop syndrome (Billroth II) - obstruction of the afferent limb leads to pain and bilious vomiting
- Nutritional deficiencies - vitamin B12 deficiency (loss of intrinsic factor), iron deficiency anemia, calcium/vitamin D malabsorption, folate deficiency
- Remnant gastric cancer - increased risk >15-20 years post-gastrectomy; requires surveillance endoscopy
- Roux stasis syndrome - poor emptying of the Roux limb
Key references:
- Fischer's Mastery of Surgery 8e, Chapter: Distal Gastrectomy (Open and Minimally Invasive Techniques), pp. 2938-2947
- Bailey & Love's Short Practice of Surgery 28e, Chapter 67, pp. subtotal/total gastrectomy sections
Describe the surgical anatomy of the stomach and discuss the clinical features, evaluation and management of a case of bleeding duodenal ulcer. [2+2+2+4]
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative sources. Let me compile the complete answer.
Surgical Anatomy of the Stomach & Bleeding Duodenal Ulcer
(Sources: Bailey & Love's Short Practice of Surgery 28e, Schwartz's Principles of Surgery 11e, Mulholland & Greenfield's Surgery 7e, Current Surgical Therapy 14e)
1. SURGICAL ANATOMY OF THE STOMACH [2 marks]
Parts and Surfaces
The stomach lies in the left hypochondrium and epigastrium. It is divided into:
- Cardia - the junction with the oesophagus at the gastro-oesophageal junction
- Fundus - the dome-shaped part above the cardia; lies in contact with the left hemidiaphragm
- Body (corpus) - the largest part, containing parietal (acid-secreting) and chief (pepsinogen-secreting) cells in gastric crypts
- Antrum - the distal part containing G cells (gastrin-producing) and mucus-secreting pyloric glands
- Pylorus - the sphincteric junction with the duodenum
The lesser curvature runs from cardia to pylorus on the right. The greater curvature forms the left/inferior border. The angular incisure (incisura angularis) marks the junction of body and antrum on the lesser curvature.
Blood Supply (clinically critical)
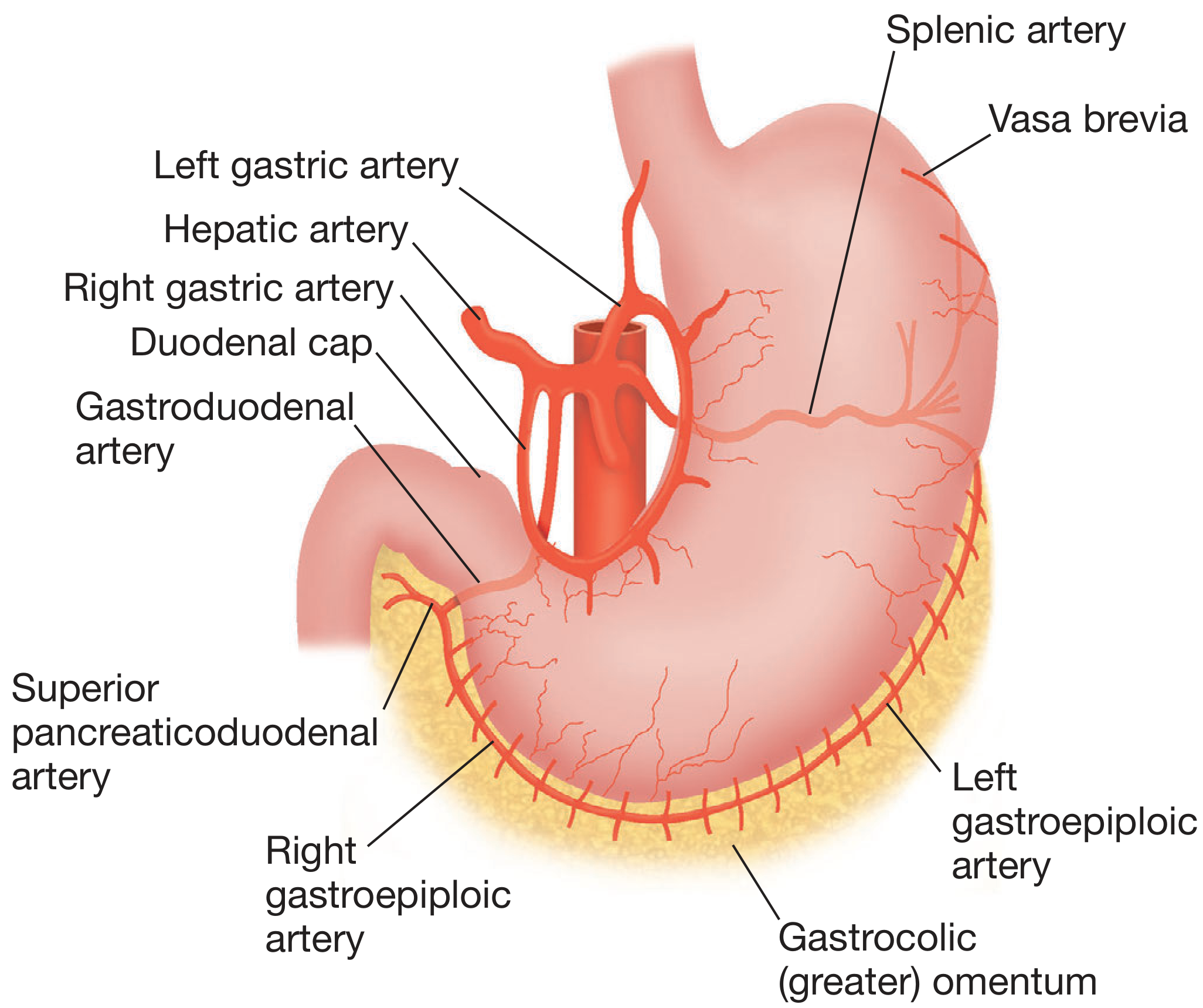
- Lesser curvature: Left gastric artery (from coeliac axis) anastomoses with right gastric artery (from common hepatic artery)
- Greater curvature: Right gastroepiploic artery (from gastroduodenal artery) anastomoses with left gastroepiploic artery (from splenic artery)
- Fundus: Vasa brevia (short gastric arteries) from the splenic artery
- Gastroduodenal artery (GDA): Passes behind the first part of the duodenum - directly clinically relevant to bleeding duodenal ulcer. It divides into the superior pancreaticoduodenal artery (anastomoses with the inferior pancreaticoduodenal from SMA) and the right gastroepiploic artery
Venous Drainage
Veins parallel the arteries; those on the lesser curvature drain into the portal vein, and those on the greater curvature drain into the splenic vein. The coronary (left gastric) vein runs along the lesser curvature toward the oesophagus, then passes left to right to join the portal vein - it becomes markedly dilated in portal hypertension.
Nerve Supply
- Intrinsic: Myenteric plexus of Auerbach (motility) and submucosal plexus of Meissner (secretion)
- Extrinsic: Vagus nerves (CN X) - anterior and posterior trunks condense from the oesophageal plexus as they pass through the oesophageal hiatus. Efferent fibres mediate receptive relaxation, gastric motility, and acid secretion. The sympathetic supply derives from the coeliac ganglia.
Microscopic Anatomy (surgical relevance)
The mucosa contains: surface mucus cells, parietal cells (body - secrete HCl via H+/K+-ATPase proton pump), chief cells (body - secrete pepsinogen), G cells (antrum - secrete gastrin), and ECL cells (secrete histamine in response to gastrin and vagal stimulation).
2. CLINICAL FEATURES OF BLEEDING DUODENAL ULCER [2 marks]
Bleeding from a posterior duodenal ulcer typically erodes the gastroduodenal artery or one of its branches - this explains the severity and potential for life-threatening haemorrhage.
Symptoms:
- Haematemesis - vomiting of bright red blood or coffee-ground material (blood altered by gastric acid)
- Melaena - passage of black, tarry, offensive stools; indicates upper GI bleeding proximal to the ligament of Treitz
- Haematochezia - fresh rectal bleeding; implies massive bleeding (>1000 mL) with rapid transit
- Previous dyspeptic history - epigastric pain, heartburn, use of NSAIDs/aspirin, prior PUD, H. pylori infection
- Syncope or presyncope - indicates significant haemodynamic compromise
Signs:
- Haemodynamic instability: Tachycardia (pulse >100/min), hypotension (SBP <100 mmHg), postural hypotension, pallor, cold clammy peripheries - indicating >20-30% blood volume loss
- Epigastric tenderness on examination
- Signs of shock in massive bleeding: altered consciousness, oliguria, metabolic acidosis
- Stigmata of chronic liver disease should be sought to exclude variceal bleeding
High-risk features (indicating likely rebleeding):
- Posteroinferior location of ulcer (erodes GDA)
- Age >60 years
- Hypovolemic shock at presentation
- Haematemesis with fresh blood
- Active bleeding at endoscopy (arterial jet)
- Ulcer size >2 cm
- Comorbid illness
3. EVALUATION (INVESTIGATION) [2 marks]
Initial Assessment and Resuscitation (concurrent)
- Two large-bore IV cannulae; aggressive fluid resuscitation with crystalloids/colloids
- Blood for: FBC, U&E, LFTs, coagulation screen, group & crossmatch (at least 4-6 units)
- ABG if haemodynamically compromised
- Urinary catheterisation - monitor urine output as marker of renal perfusion
- Nasogastric tube - to confirm blood in stomach, decompress, and monitor further bleeding
Risk Stratification Scores
Rockall Score (pre- and post-endoscopy) - predicts rebleeding and mortality:
| Variable | Score |
|---|---|
| Age <60 yrs = 0; 60-79 = 1; ≥80 = 2 | |
| Shock: No shock = 0; tachycardia = 1; hypotension = 2 | |
| Comorbidity: None = 0; cardiac/other major = 2; renal/liver failure, disseminated malignancy = 3 | |
| Endoscopic diagnosis: Mallory-Weiss/no lesion = 0; all other = 1; upper GI malignancy = 2 | |
| Stigmata: None/dark spot = 0; blood in upper GI tract, adherent clot, visible vessel, active bleeding = 2 |
- Clinical Rockall score (pre-endoscopy) of 0 = low risk; complete score ≤2 = low risk for rebleeding/death
- Glasgow-Blatchford Score (GBS): uses BUN, Hb, SBP, pulse, melaena, syncope, hepatic disease, cardiac failure; score 0 = safe for outpatient management
Endoscopy (EGD) - the key investigation
- Should be performed within 24 hours of presentation (within 12 hours if haemodynamically unstable after resuscitation)
- Confirms the source of bleeding (rules out varices, Mallory-Weiss tear)
- Forrest Classification guides endoscopic management:
| Forrest | Appearance | Rebleeding risk |
|---|---|---|
| Ia | Active arterial spurting | ~90% |
| Ib | Active oozing | ~30-50% |
| IIa | Non-bleeding visible vessel | ~50% |
| IIb | Adherent clot | ~25-30% |
| IIc | Haematin-covered flat spot | ~7-10% |
| III | Clean base | <5% |
Other Investigations
- CT angiography - if endoscopy fails to identify source or control bleeding; detects active bleeding at rates >0.5 mL/min
- Formal angiography - if CT angiography positive; allows therapeutic embolisation
- ECG and chest X-ray - baseline cardiac/pulmonary assessment
4. MANAGEMENT [4 marks]
A. Initial Resuscitation
- Airway protection (consider intubation if active haematemesis and altered consciousness)
- Restore circulating volume: IV crystalloids initially, then blood products (target Hb ≥7-8 g/dL; ≥9-10 g/dL in cardiac disease)
- Correct coagulopathy: FFP, platelet transfusions if required
- IV Proton Pump Inhibitor: Omeprazole/pantoprazole 80 mg IV bolus then 8 mg/hr infusion - reduces rebleeding by maintaining intragastric pH >6 and stabilising clot
- Withhold anticoagulants/antiplatelet agents where possible; reverse if life-threatening bleeding
- Surgical consultation is mandatory from the outset
B. Endoscopic Therapy (first-line haemostatic treatment)
Performed for Forrest Ia, Ib, IIa, and IIb lesions:
- Injection therapy: Dilute adrenaline (epinephrine 1:10,000) injected around the vessel - causes tamponade and vasoconstriction; used as adjunct, not alone
- Thermal coagulation: Bipolar electrocoagulation (BICAP) or heater probe - achieves coaptive coagulation; reduces rebleeding rates
- Mechanical clips: Haemoclips applied across the bleeding vessel; Over-the-scope clips (OTSC) are superior for recurrent/refractory bleeding
- Dual therapy (injection + thermal/clip) is superior to monotherapy
- A second attempt at endoscopic haemostasis for rebleeding is as effective as surgery with fewer complications and is recommended
C. Medical Management post-endoscopy
- Continue high-dose IV PPI for 72 hours, then oral PPI
- H. pylori eradication (triple therapy): rebleeding reduced from 20% to 3% after successful eradication
- Stop NSAIDs; if unavoidable, use COX-2 inhibitor + long-term PPI
- Long-term PPI if chronic aspirin/anticoagulants required
D. Interventional Radiology
- Transcatheter arterial embolisation (TAE) - salvage option when endoscopic control fails; embolises the gastroduodenal artery or its branches; avoids surgical risk in high-risk patients
E. Surgical Management
Indicated when:
- Massive haemorrhage unresponsive to initial endoscopic control
- Recurrent haemorrhage after two attempts at endoscopic therapy
- Ongoing bleeding requiring >4 units blood in 24 hours or >8 units in 48 hours
- Haemodynamic instability/shock unresponsive to resuscitation
- Concomitant perforation or obstruction
Surgical options:
-
Oversewing (suture ligation) of the bleeding vessel - the most commonly performed emergency procedure:
- Longitudinal pyloroduodenotomy or duodenotomy for exposure
- Kocher maneuver first - reduces tension and allows manual haemorrhage control with the left hand (fingers behind pancreatic head, thumb anterior)
- U-stitch or figure-of-eight sutures placed in the ulcer base using heavy material - controls the GDA, its superior pancreaticoduodenal branch, and the transverse pancreatic branch (important to include all three)
- Closure of pylorotomy as a pyloroplasty (Heineke-Mikulicz)
- Higher rebleeding rate but lower operative mortality than resection; 30-day mortality ~27%
-
Oversewing + Vagotomy and Drainage (V+D) - preferred definitive operation if patient is haemodynamically stable and surgeon experienced:
- Truncal vagotomy + pyloroplasty
- 30-day postoperative mortality ~12% (NSQIP data)
- Reduces acid secretion and rebleeding risk
-
Vagotomy and Antrectomy (V+A) - lowest rebleeding rate but highest operative morbidity:
- Reserved for haemodynamically stable, low-risk patients
- Billroth II gastrojejunostomy for reconstruction
- Large posterior duodenal ulcers may need to be left in the duodenal stump with suture haemostasis and secure stump closure + omental buttress + duodenostomy decompression
- 30-day mortality ~23%; rarely performed today
F. Postoperative Management
- High-dose PPI in early postoperative period (reduces rebleeding)
- Early rebleeding evaluated with EGD + CT/formal angiography
- H. pylori eradication if not yet treated
- Long-term smoking cessation; avoid NSAIDs
- If NSAIDs medically necessary: COX-2 inhibitor + PPI
Key references:
- Bailey & Love's Short Practice of Surgery 28e, Ch. 67, pp. 1170-1172
- Schwartz's Principles of Surgery 11e, Ch. 26, pp. 1154-1161
- Mulholland & Greenfield's Surgery 7e, Ch. 45, pp. 2262-2263
- Current Surgical Therapy 14e, Ch: Surgery for Bleeding Duodenal Ulcer, pp. 132-133
Describe the surgical anatomy of the stomach and discuss the clinical features, evaluation and management of a case of bleeding duodenal ulcer. [2+2+2+4]
This is the same question I just answered in detail. Here is the complete answer again for your reference:
Surgical Anatomy of the Stomach & Bleeding Duodenal Ulcer
(Sources: Bailey & Love's Short Practice of Surgery 28e, Schwartz's Principles of Surgery 11e, Mulholland & Greenfield's Surgery 7e, Current Surgical Therapy 14e)
1. SURGICAL ANATOMY OF THE STOMACH [2 marks]
Parts and Curvatures
The stomach occupies the left hypochondrium and epigastrium. It has five parts:
- Cardia - oesophagogastric junction
- Fundus - dome above the cardia, in contact with the left hemidiaphragm
- Body (corpus) - largest part; contains parietal cells (HCl via H+/K+-ATPase) and chief cells (pepsinogen)
- Antrum - distal part; contains G cells (gastrin) and mucus-secreting pyloric glands
- Pylorus - sphincteric junction with the duodenum
The lesser curvature runs from cardia to pylorus on the right; the greater curvature forms the left/inferior border. The angular incisure (incisura angularis) on the lesser curvature marks the body-antrum junction.
Blood Supply (surgically critical)
| Vessel | Origin | Territory |
|---|---|---|
| Left gastric artery | Coeliac axis | Lesser curvature (upper) |
| Right gastric artery | Common hepatic artery | Lesser curvature (lower), anastomoses with left gastric |
| Gastroduodenal artery (GDA) | Common hepatic artery | Passes behind D1; divides into right gastroepiploic + superior pancreaticoduodenal |
| Right gastroepiploic artery | GDA | Greater curvature (right) |
| Left gastroepiploic artery | Splenic artery | Greater curvature (left) |
| Vasa brevia (short gastric arteries) | Splenic artery (terminal branches) | Fundus |
The GDA lying posterior to the first part of the duodenum is directly responsible for life-threatening haemorrhage when a posterior duodenal ulcer erodes into it.
Venous Drainage
Veins parallel the arteries. Lesser curvature veins drain into the portal vein; greater curvature veins drain into the splenic vein. The coronary (left gastric) vein runs along the lesser curvature toward the oesophagus, then passes left-to-right to join the portal vein - it becomes markedly dilated in portal hypertension (oesophageal varices).
Nerve Supply
- Intrinsic: Myenteric plexus of Auerbach (motility) and submucosal plexus of Meissner (secretion)
- Extrinsic: Vagus nerves (CN X) - the oesophageal plexus condenses into anterior and posterior trunks passing through the oesophageal hiatus. Efferent fibres mediate receptive relaxation, gastric motility, and acid secretion (cephalic phase). Sympathetic supply from the coeliac ganglia.
Microscopic Anatomy
Surface mucous cells protect the lining. Gastric crypts contain: parietal cells (body - HCl secretion), chief cells (body - pepsinogen), G cells (antrum - gastrin), and ECL cells (histamine, paracrine stimulator of parietal cells). The gastric mucous layer is essential to mucosal integrity.
2. CLINICAL FEATURES OF BLEEDING DUODENAL ULCER [2 marks]
A posterior duodenal ulcer bleeds by erosion into the gastroduodenal artery - the most dangerous form of peptic ulcer haemorrhage.
Symptoms:
- Haematemesis - vomiting of fresh red blood (brisk bleeding) or coffee-ground material (blood altered by gastric acid, slower bleed)
- Melaena - black, tarry, foul-smelling stools; characteristic of upper GI bleeding proximal to the ligament of Treitz
- Haematochezia - fresh rectal bleeding; indicates massive haemorrhage (>1000 mL) with rapid transit
- Prior dyspeptic history, NSAID/aspirin use, known H. pylori infection, smoking
- Syncope or presyncope - indicates significant haemodynamic compromise
Signs:
- Haemodynamic instability: Tachycardia (>100/min), hypotension (SBP <100 mmHg), postural hypotension, pallor, cold clammy peripheries - indicating >20-30% blood volume loss
- Epigastric tenderness
- Signs of shock in massive bleeding: altered consciousness, oliguria
- Stigmata of chronic liver disease should be sought to exclude variceal bleeding as the source
High-risk features predicting rebleeding:
- Posterior duodenal location (erodes GDA)
- Age >60 years
- Haemodynamic shock at presentation
- Active arterial bleeding at endoscopy
- Ulcer size >2 cm
- Significant comorbidity
3. EVALUATION [2 marks]
Resuscitation (simultaneous with evaluation)
- Two large-bore IV cannulae; aggressive IV fluid resuscitation
- Blood: FBC, U&E, LFTs, coagulation screen, group & crossmatch (4-6 units)
- Urinary catheter to monitor urine output
- Nasogastric tube to confirm blood in stomach, decompress, and monitor ongoing bleeding
Risk Stratification
Rockall Score (pre- and post-endoscopy) - predicts rebleeding and mortality (total 0-11):
| Variable | Points |
|---|---|
| Age: <60 = 0; 60-79 = 1; ≥80 = 2 | |
| Shock: none = 0; tachycardia = 1; hypotension = 2 | |
| Comorbidity: none = 0; cardiac/major = 2; renal/liver failure or malignancy = 3 | |
| Endoscopic diagnosis: Mallory-Weiss/no lesion = 0; other = 1; upper GI malignancy = 2 | |
| Stigmata of recent haemorrhage: none/dark spot = 0; blood, adherent clot, visible vessel, active bleeding = 2 |
- Clinical (pre-endoscopy) Rockall score = 0 → low risk; complete score ≤2 → low risk for rebleeding/death
- Glasgow-Blatchford Score (GBS): incorporates BUN, Hb, SBP, pulse, melaena, syncope, hepatic/cardiac disease; GBS = 0 is safe for outpatient management
Endoscopy (OGD) - the key investigation
- Performed within 24 hours of presentation (within 12 hours if haemodynamically unstable after resuscitation)
- Confirms bleeding source, excludes varices
- Forrest Classification guides endoscopic treatment decision:
| Class | Appearance | Rebleeding risk |
|---|---|---|
| Ia | Active arterial spurting | ~90% |
| Ib | Active oozing | ~30-50% |
| IIa | Non-bleeding visible vessel | ~50% |
| IIb | Adherent clot | ~25-30% |
| IIc | Haematin-covered flat spot | ~7-10% |
| III | Clean base | <5% |
Further Investigations
- CT angiography - detects active bleeding >0.5 mL/min; used when endoscopy fails or is non-diagnostic
- Formal angiography - if CT positive; allows therapeutic embolisation
- ECG and chest X-ray for baseline cardiopulmonary assessment
4. MANAGEMENT [4 marks]
A. Resuscitation
- Airway protection (consider intubation if active haematemesis + altered consciousness)
- Restore circulating volume: IV crystalloids initially, then blood (target Hb ≥7 g/dL; ≥9-10 g/dL in cardiac disease)
- Correct coagulopathy: FFP, platelets as needed
- IV PPI: Omeprazole/pantoprazole 80 mg IV bolus then 8 mg/hr infusion - maintains intragastric pH >6, stabilises clot, reduces rebleeding
- Withhold/reverse anticoagulants and antiplatelet agents in life-threatening bleeding
- Mandatory early surgical consultation
B. Endoscopic Haemostasis (first-line treatment for Forrest Ia, Ib, IIa, IIb)
- Injection therapy: Dilute adrenaline (1:10,000) injected around the vessel - tamponade + vasoconstriction; used as adjunct only (not monotherapy)
- Thermal coagulation: Bipolar electrocoagulation (BICAP) or heater probe - coaptive coagulation of vessel
- Mechanical clips: Haemoclips or over-the-scope clips (OTSC) - superior for recurrent/refractory bleeding; OTSC shown to be more effective than standard haemoclipping in randomised trials
- Dual therapy (injection + thermal or clip) is superior to monotherapy
- A second attempt at endoscopic haemostasis for rebleeding is recommended before surgery - equally effective with fewer complications
C. Medical Management (post-endoscopy)
- High-dose IV PPI for 72 hours, then oral PPI
- H. pylori eradication (triple therapy - PPI + amoxicillin + clarithromycin): reduces rebleeding from 20% to 3%
- Discontinue NSAIDs; if unavoidable, use COX-2 inhibitor + long-term PPI
- Long-term PPI if chronic aspirin or anticoagulants required; smoking cessation
D. Interventional Radiology (salvage after failed endoscopy)
- Transcatheter arterial embolisation (TAE) of the GDA or its branches
- Avoids surgical risk in high-risk/elderly patients; preferred in centres with 24-hour IR availability
E. Surgical Management
Indications for surgery:
- Massive haemorrhage unresponsive to initial endoscopic control
- Recurrent haemorrhage after two attempts at endoscopic therapy
- Ongoing bleeding requiring >4 units blood in 24 hours or >8 units in 48 hours
- Haemodynamic shock unresponsive to resuscitation
- Concurrent perforation or obstruction
Surgical options:
1. Oversewing (suture ligation) alone - most commonly performed emergency procedure:
- Longitudinal pyloroduodenotomy or duodenotomy for exposure
- Kocher manoeuvre first - reduces tension and allows manual haemorrhage control (left hand: long fingers behind pancreatic head, thumb anterior)
- U-stitch or figure-of-eight sutures with heavy material in the ulcer base, securing the GDA proximally, distally, and the transverse pancreatic branch (3-point ligation)
- Abrade ulcer bed with sucker tip to confirm secure haemostasis
- Close pylorotomy as a Heineke-Mikulicz pyloroplasty
- Operative mortality ~27% (NSQIP); higher rebleeding rate but lowest operative morbidity
2. Oversewing + Truncal Vagotomy and Drainage (V+D) - preferred definitive option if patient is stable:
- Truncal vagotomy + pyloroplasty
- Reduces acid secretion and rebleeding risk
- 30-day operative mortality ~12% (NSQIP data) - significantly lower than oversewing alone
3. Vagotomy and Antrectomy (V+A) - lowest ulcer recurrence/rebleeding:
- Reserved for haemodynamically stable, low-risk patients where exposure is straightforward
- Billroth II gastrojejunostomy for reconstruction
- Large posterior ulcers may need to be left in duodenal stump with suture haemostasis + secure stump closure + omental buttress + duodenostomy decompression tube
- 30-day mortality ~23%; rarely performed today given availability of PPIs and H. pylori treatment
F. Postoperative Management
- High-dose PPI in early postoperative period
- H. pylori eradication if not yet completed
- Early rebleeding: evaluate with OGD + CT/formal angiography
- Long-term smoking cessation; avoid NSAIDs
Key references:
- Bailey & Love's Short Practice of Surgery 28e, Ch. 67, pp. 1170-1172
- Schwartz's Principles of Surgery 11e, Ch. 26, pp. 1154-1161
- Mulholland & Greenfield's Surgery 7e, Ch. 45, pp. 2262-2263
- Current Surgical Therapy 14e, Surgery for Bleeding Duodenal Ulcer, pp. 132-133
Differentiate between a gastric and duodenal ulcer. [5]
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have excellent content. Let me compile the comprehensive differentiation table and narrative.
Differentiation Between Gastric Ulcer and Duodenal Ulcer
(Sources: Sabiston Textbook of Surgery 21e, Bailey & Love's Short Practice of Surgery 28e, S. Das Manual on Clinical Surgery 13e)
| Feature | Gastric Ulcer (GU) | Duodenal Ulcer (DU) |
|---|---|---|
| Incidence | Less common (GU : DU ≈ 1 : 4) | More common; commonest peptic ulcer |
| Age of onset | Peak 55-65 years; rarely before age 40 | Peak 30-55 years; younger onset |
| Sex | Slight female predominance (or equal) | Male predominance (M : F ≈ 3-4 : 1) |
| Site | Lesser curvature at incisura angularis (type I, ~50-60%); also near GEJ (type IV), prepyloric (type III); body with duodenal ulcer (type II) | Anterior or posterior wall of the first part of the duodenum (D1 bulb); posterior wall ulcers erode the gastroduodenal artery |
| Acid secretion | Normal or low (type I GU); hypersecretion in types II, III (prepyloric) | Increased; BAO and MAO both elevated; increased parietal cell mass (~2× normal) |
| Pathogenesis | Defective mucosal defence - impaired mucus/bicarbonate secretion, mucosal ischaemia, bile reflux, weakened tight junctions; H. pylori disrupts protective mucosa; NSAIDs strongly associated | Aggressive factors dominant - excess acid/pepsin overwhelms normal mucosa; H. pylori (>90% of cases) causes antral gastritis, raises gastrin, reduces somatostatin, increasing acid; gastric emptying is accelerated, delivering more acid to duodenum |
| H. pylori association | ~70-80% | >90%; almost universal |
| NSAID association | Strongly associated (NSAID-induced ulcers preferentially in stomach) | Less strongly associated than GU |
| Blood group | No association | Group O more commonly affected (historical observation) |
| Pain character | Epigastric pain related to meals - food may worsen or give no relief; burning/gnawing | Epigastric pain relieved by food (food buffers acid); burning/gnawing |
| Pain timing | Pain occurs during or soon after eating | Classic night pain (wakes patient 1-2 AM); pain 2-3 hours after meals (hunger pain); relieved by food/antacids |
| Tender spot | Midepigastrium, below the xiphoid process | ~1½ inches to the right of the midline on the transpyloric plane (L1) |
| Vomiting | More common - food may trigger vomiting | Less common unless gastric outlet obstruction develops |
| Weight | Weight loss common (fear of eating/reduced intake) | Weight gain may occur (eating relieves pain, so patient eats more) |
| Appetite | Reduced (sitophobia - fear of food) | Normal or increased |
| Periodicity | Less marked periodicity | Classic periodicity - periods of weeks of pain separated by weeks/months of relief |
| Malignant potential | Present - a gastric ulcer may be or may become malignant; all gastric ulcers require biopsy and follow-up endoscopy to confirm healing | Absent - duodenal ulcers are virtually never malignant |
| Complications | Perforation (often into lesser sac), haemorrhage (left gastric or short gastric artery), gastric outlet obstruction (pyloric/antral ulcers), malignant transformation | Perforation (anterior wall - into peritoneal cavity), haemorrhage (posterior wall - gastroduodenal artery), gastric outlet obstruction (scarring), pancreatitis (posterior penetration) |
| Most common vessel eroded in bleeding | Left gastric artery (lesser curvature), right gastroepiploic (greater curvature) | Gastroduodenal artery (posterior DU) |
| Surgical treatment | Distal gastrectomy (to include ulcer) + Billroth I/Roux-en-Y; biopsy mandatory if not resected | Oversewing (emergency) ± truncal vagotomy + pyloroplasty; vagotomy and antrectomy in stable patients |
| Indication for surgery | Malignancy must be excluded; perforation, haemorrhage, GOO | Perforation, haemorrhage refractory to endoscopy, GOO; intractability (rare now) |
| Recurrence after H. pylori eradication | 20% if not eradicated; markedly reduced after eradication | 20% if not eradicated; reduces to ~3% after eradication |
| Endoscopic appearance | Typically punched-out ulcer with overhanging edges (benign); rolled, heaped-up edges suggest malignancy; multiple biopsies (≥8) from edge and base mandatory | Punched-out ulcer in D1 bulb; biopsies not routinely required as malignancy not a concern; biopsy antral mucosa for H. pylori |
| Radiological (barium meal) | Ulcer crater projects outside the stomach lumen (in profile); Hampton's line (thin radiolucent line across ulcer neck); Carman's meniscus sign in malignant ulcer | Ulcer crater in D1; "cloverleaf" or "trefoil" deformity from scarring of the bulb; giant duodenal ulcer may fill entire bulb |
Johnson Classification of Gastric Ulcers (surgical relevance)
| Type | Location | Acid Secretion | Association |
|---|---|---|---|
| I | Lesser curvature at incisura (50-60%) | Low/normal | Most common |
| II | Body + concurrent duodenal ulcer (15-20%) | High | Behaves like DU |
| III | Prepyloric (20%) | High | Behaves like DU |
| IV | Near GEJ on lesser curvature (<10%) | Normal | Technically demanding surgery |
| V | Anywhere | Any | NSAID-associated |
Key Points for Exam
- "No acid, no ulcer" - both require acid but the mechanism differs: GU has defective defence; DU has excess acid
- Duodenal ulcers are more common, occur in younger patients, cause night pain relieved by food, and are never malignant
- Gastric ulcers occur in older patients, cause food-related pain, are associated with NSAIDs, and must always be biopsied to exclude malignancy
- Both are principally caused by H. pylori, and eradication is the cornerstone of treatment
- A perforated anterior DU spills into the peritoneal cavity (surgical emergency); a perforated posterior DU penetrates into the pancreas
Key references:
- Sabiston Textbook of Surgery 21e, Ch. 86, pp. 1771-1800
- Bailey & Love's Short Practice of Surgery 28e, Ch. 67, pp. 1173-1177
- S. Das Manual on Clinical Surgery 13e, Ch. 34, pp. 491-495
Enumerate the causes of gastric outlet obstruction
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have a comprehensive, textbook-sourced answer. Here it is:
Causes of Gastric Outlet Obstruction (GOO)
(Sources: Yamada's Textbook of Gastroenterology 7e - Table 49.8; Bailey & Love's Short Practice of Surgery 28e; Current Surgical Therapy 14e)
GOO is defined as mechanical or functional obstruction at the level of the gastric antrum, pylorus, or proximal duodenum preventing normal gastric emptying. Causes are classified as benign or malignant.
A. MALIGNANT CAUSES (50-80% of GOO in developed countries - now the commonest overall)
- Carcinoma of the stomach (antral/pyloric carcinoma) - commonest single malignant cause
- Carcinoma of the pancreas - local extension into the duodenum/pyloric region
- Gastric lymphoma (primary)
- Proximal duodenal carcinoma (D1/D2)
- Ampullary carcinoma (carcinoma of the ampulla of Vater)
- Gallbladder/biliary tree carcinoma - local extension
- Gastric carcinoid tumour
- Metastatic disease to the gastric antrum or duodenum (e.g., from breast, lung, melanoma)
B. BENIGN CAUSES
1. Peptic Ulcer Disease (~5% in developed countries; still 50-60% in low/middle-income countries)
- Chronic duodenal ulcer with fibrosis and scarring of D1 (the classical cause)
- Pyloric channel ulcer with oedema + fibrosis
- Gastric ulcer of the antrum/prepyloric region
2. Inflammatory and Infiltrative Conditions
- Crohn's disease involving the stomach or duodenum (~5% of GOO)
- Chronic pancreatitis with fibrosis compressing the duodenum (1-5%)
- Large pancreatic pseudocyst - external compression of the duodenum
- Acute severe pancreatitis - oedema and inflammation
- Cholecystitis - adjacent inflammation (rare)
- Eosinophilic gastroenteritis - submucosal infiltration
- Gastric tuberculosis - granulomatous inflammation and stricture
- Sarcoidosis / amyloid infiltration of the gastric wall
- Strongyloides infection (in endemic areas)
3. Congenital Causes
- Infantile hypertrophic pyloric stenosis (IHPS) - hypertrophy of the pyloric musculature; commonest surgical emergency in infancy
- Adult hypertrophic pyloric stenosis - rare adult form
- Annular pancreas - encircles the second part of the duodenum, may present in adulthood
- Duodenal webs / membranes - congenital obstruction
- Duodenal atresia - complete obstruction (neonatal)
- Ectopic pancreas in the pyloric/duodenal wall
4. Vascular
- Superior mesenteric artery (SMA) syndrome (Wilkie's syndrome) - compression of D3 by the SMA
5. Mechanical / Miscellaneous
- Bouveret syndrome - impaction of a gallstone in the pyloric channel or duodenum following migration through a cholecystoduodenal/cholecystogastric fistula
- Gastric bezoars - phytobezoar, trichobezoar causing pyloric/antral obstruction
- Large pedunculated gastric polyp prolapsing into the pylorus
- Gastric volvulus - organoaxial or mesenteroaxial rotation causing obstruction
- Caustic ingestion - stricture formation after acid/alkali ingestion
- Migration of a PEG tube (buried bumper syndrome) causing intraluminal obstruction
- Post-surgical complications - anastomotic stricture, stomal stenosis, afferent loop obstruction after Billroth II
- Duodenal haematoma - after blunt abdominal trauma (especially in children)
- Radiation stricture - after radiotherapy to the upper abdomen
Summary by Mechanism
| Mechanism | Examples |
|---|---|
| Intraluminal | Bezoar, gallstone (Bouveret), pedunculated polyp, PEG tube migration |
| Intramural | Carcinoma, pyloric stenosis (PUD/IHPS), Crohn's, TB, caustic stricture, lymphoma, hypertrophic pyloric stenosis |
| Extramural | Pancreatic cancer/pseudocyst, SMA syndrome, annular pancreas, cholecystitis |
Key Clinical Points
- In the current era, malignancy (especially pancreatic and gastric carcinoma) is the commonest cause of GOO in developed countries and must be assumed until excluded by endoscopic biopsy
- Benign pyloric stenosis from chronic PUD should be a diagnosis of exclusion
- The characteristic metabolic abnormality of benign GOO (repeated vomiting of HCl-rich fluid) is hypochloraemic, hypokalaemic metabolic alkalosis with paradoxical aciduria
- Zollinger-Ellison syndrome is associated with GOO in ~10% of cases (severe acid hypersecretion causing multiple, refractory duodenal ulcers)
Key references:
- Yamada's Textbook of Gastroenterology 7e, Table 49.8, p. 1042
- Bailey & Love's Short Practice of Surgery 28e, Ch. 67, p. 1190
- Current Surgical Therapy 14e, Gastric Outlet Obstruction, p. 132
Enlist the investigations required to diagnose i
It looks like your message got cut off — it ends with "to diagnose i". Could you complete the question?
GOO
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have comprehensive textbook content. Here is the complete answer:
Investigations to Diagnose Gastric Outlet Obstruction (GOO)
(Sources: Yamada's Textbook of Gastroenterology 7e; Bailey & Love's Short Practice of Surgery 28e; Current Surgical Therapy 14e)
I. LABORATORY INVESTIGATIONS
These establish the metabolic consequences of GOO and help assess the patient's overall status:
- Serum electrolytes (Na+, K+, Cl-) - the hallmark is hypochloraemic, hypokalaemic metabolic alkalosis due to repeated vomiting of HCl-rich gastric contents; low chloride and low potassium
- Arterial blood gas (ABG) - confirms metabolic alkalosis (raised pH, raised HCO3-, raised base excess); paradoxical aciduria in late stages as kidneys excrete H+ to conserve Na+
- Serum urea and creatinine - elevated if pre-renal acute kidney injury from dehydration
- Serum calcium - may be low (alkalosis reduces ionised calcium → tetany)
- Full blood count (FBC) - anaemia from chronic blood loss or malnutrition; raised WCC if infective cause
- Liver function tests + serum albumin - hypoalbuminaemia reflects chronic malnutrition; LFTs relevant if biliary/hepatic malignancy suspected
- Serum amylase/lipase - if pancreatitis is a suspected cause
- Tumour markers - CA 19-9 (pancreatic cancer), CEA, CA 72-4 (gastric cancer) - useful when malignancy is suspected, though not diagnostic alone
- H. pylori testing (when stable) - urea breath test or stool antigen; serology for prevalence assessment
II. BEDSIDE / CLINICAL TESTS
- Succussion splash (clinical) - auscultate over the epigastrium while rocking the patient side-to-side; audible splash >3 hours after last oral intake confirms large volume gastric residue
- Saline load test (historical/occasionally used) - 750 mL of normal saline instilled via NGT; aspiration of >400 mL at 30 minutes suggests mechanical obstruction; aspiration <200 mL suggests resolution after treatment
III. IMAGING INVESTIGATIONS
A. Plain X-rays
- Erect chest X-ray - may show a massively dilated stomach; also rules out pneumoperitoneum (perforation) and pulmonary pathology
- Plain abdominal X-ray (erect + supine) - shows a large gastric shadow with a fluid level in the left upper quadrant; distended stomach; absence of gas in small bowel distal to obstruction
B. Contrast Studies
- Barium meal (upper GI series) / water-soluble contrast study (Gastrografin) - demonstrates:
- Dilated, atonic stomach with large gastric residue
- Narrowing at the pylorus or D1
- "Rat-tail" or "apple-core" deformity suggests malignant stricture
- Mucosal pattern of duodenal scarring (cloverleaf deformity) in benign PUD
- Delayed gastric emptying
- Note: Water-soluble contrast preferred if perforation is suspected
C. Ultrasound
- Abdominal ultrasound - useful initial investigation; shows a distended fluid-filled stomach; can identify pancreatic mass, pseudocyst, gallstones (Bouveret syndrome), hepatic metastases, lymphadenopathy; limited by bowel gas
D. Cross-sectional Imaging (most important for staging and cause)
- CT scan of abdomen and pelvis (with IV + oral contrast) - the investigation of choice for determining the cause of GOO:
- Identifies the site and level of obstruction
- Shows pancreatic carcinoma, gastric carcinoma, lymphoma
- Demonstrates lymphadenopathy, liver metastases, peritoneal disease (staging)
- Identifies pancreatic pseudocysts, annular pancreas, aortic/SMA compression
- Guides decision between curative and palliative management
-
CT angiography / MRI - if SMA syndrome suspected; demonstrates reduced aortomesenteric angle
-
PET-CT - for staging of malignancy if surgery is being considered
IV. ENDOSCOPIC INVESTIGATIONS (most important for definitive diagnosis)
- Upper GI endoscopy (OGD) - the key investigation; performed after gastric decompression with NGT:
- Directly visualises the antrum, pylorus, and duodenum
- Identifies the cause: ulcer disease, malignant mass, web, Crohn's stricture
- Biopsy is mandatory - multiple biopsies from the stricture edge to exclude malignancy (gastric cancer can mimic benign pyloric stenosis)
- Can be therapeutic (balloon dilatation, stent insertion)
- Endoscopic ultrasound (EUS) - when CT and OGD biopsies are inconclusive:
- Gives detailed imaging of the gastric wall layers and peri-gastric/peripancreatic structures
- Enables EUS-guided fine needle aspiration (FNA/FNB) of a mass for histology
- Particularly useful for submucosal lesions, GIST, and lymphoma
- Gastric emptying scintigraphy (radionuclide study) - useful to distinguish mechanical GOO from functional gastroparesis (diabetic, postsurgical); not required if mechanical cause is obvious on imaging/endoscopy
Summary: Stepwise Approach
| Priority | Investigation | Purpose |
|---|---|---|
| Immediate | Serum electrolytes, ABG, urea/creatinine, FBC, albumin | Assess metabolic derangement, severity |
| Early | Plain X-ray, NGT drainage + saline load test | Confirm GOO, decompress stomach |
| Definitive cause | CT abdomen/pelvis | Identify malignancy, staging |
| Tissue diagnosis | OGD + biopsy | Confirm cause, exclude malignancy |
| Problem solving | EUS + FNA, barium meal, scintigraphy | Inconclusive cases, functional vs. mechanical |
Key references:
- Yamada's Textbook of Gastroenterology 7e, Ch. 49, p. 1041-1042
- Bailey & Love's Short Practice of Surgery 28e, Ch. 67, p. 1190
- Current Surgical Therapy 14e, Gastric Outlet Obstruction, p. 132
Describe the management of pyloric stenosis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent content from both paediatric and adult perspectives. Here is the comprehensive answer:
Management of Pyloric Stenosis
(Sources: Schwartz's Principles of Surgery 11e; Current Surgical Therapy 14e; Bailey & Love's Short Practice of Surgery 28e)
Pyloric stenosis has two distinct clinical entities requiring separate management approaches: infantile hypertrophic pyloric stenosis (IHPS) and adult pyloric stenosis (from benign peptic ulcer disease or malignancy). Both are managed along the same general principles: correct metabolic derangement first, then definitive treatment of the obstruction.
PART A: INFANTILE HYPERTROPHIC PYLORIC STENOSIS (IHPS)
Background
- Incidence: ~1 in 300 live births; presents at 3-6 weeks of age
- Male predominance: M:F = 5:1
- Caused by progressive hypertrophy of the pyloric musculature → complete GOO
- Presents with projectile, non-bilious vomiting, hunger, dehydration, weight loss
Step 1: Resuscitation and Metabolic Correction (ALWAYS before surgery)
IHPS is NEVER a surgical emergency - surgery must be deferred until metabolic abnormalities are fully corrected, as the risk of anaesthetic complications (apnoea, laryngospasm) is unacceptably high with uncorrected alkalosis.
The metabolic derangement is hypochloraemic, hypokalaemic metabolic alkalosis (from repeated vomiting of HCl-rich gastric contents) with paradoxical aciduria in severe cases.
- IV fluid resuscitation: 5% dextrose + 0.45% normal saline + KCl (2-4 mEq/kg over 24 hours) at ~150-175 mL/kg/24 hours
- Monitoring: Urine output >2 mL/kg/hour confirms adequate rehydration
- Criteria for safe anaesthesia:
- Serum chloride >100 mEq/L
- Serum bicarbonate <30 mEq/L
- Serum potassium >3.5 mEq/L
- Normal urine output
- NGT for gastric decompression during resuscitation period
Step 2: Definitive Surgery - Fredet-Ramstedt Pyloromyotomy
This is the gold-standard and only definitive treatment for IHPS. Medical treatment with IV atropine (reduces pyloric spasm) has been described but is not standard practice and has a high relapse rate.
Principle: The hypertrophied pyloric muscle is split longitudinally down to (but not through) the submucosa, allowing the mucosa to bulge through and relieve the obstruction. The pyloric musculature is NOT excised.
Approaches:
| Approach | Incision | Notes |
|---|---|---|
| Open (classical) | Right upper quadrant transverse / umbilical incision | Umbilical is cosmetically superior; transverse gives easier access |
| Laparoscopic | 3 ports (umbilical camera + 2 working) | Increasingly preferred; equal safety, superior cosmesis; 2 RCTs confirm equivalence |
Operative steps:
- Deliver the pylorus into the wound (or into the laparoscopic field)
- Make a longitudinal seromuscular incision from just proximal to the pyloric vein of Mayo (marks the pyloroduodenal junction - critical landmark to avoid duodenal perforation) extending proximally 1-2 cm onto the gastric antrum
- Spread the incised muscle down to the submucosal plane using a spreader/haemostat until the mucosa bulges freely through the entire length of the incision
- Check for mucosal perforation - insufflate air via NGT and look for bubbles; perform duodenal milking test
- If perforation occurs: repair mucosa with absorbable suture; reapproximate serosa; leave NGT 24 hours; rotate the pyloromyotomy 180° and repeat if needed (or close and allow healing)
Postoperative feeding:
- IV fluids for several hours post-op
- Start oral Pedialyte/electrolyte solution, then escalate to formula/breast milk
- Target 60 mL every 3 hours; most infants tolerate ad lib feeds
- Discharge: 24-48 hours post-operatively
Complications of pyloromyotomy:
- Mucosal perforation (1-3%) - commonest; usually at duodenal end
- Inadequate myotomy → recurrent symptoms
- Wound infection
- Bleeding
- Incomplete division → persistent GOO requiring re-operation
PART B: ADULT PYLORIC STENOSIS (Benign - Peptic Ulcer Disease)
The most common cause of adult pyloric stenosis is chronic duodenal or pyloric channel ulceration causing oedema, fibrosis, and scarring.
Step 1: Initial Assessment and Resuscitation
Metabolic correction (same principle as IHPS - surgery only after correction):
- Hypochloraemic, hypokalaemic metabolic alkalosis - correct with IV isotonic (0.9%) saline + KCl
- Replacing NaCl and water allows the kidney to auto-correct the acid-base abnormality
- Monitor electrolytes, urine output, renal function
- Correct nutritional deficits: enteral (nasojejunal tube) or parenteral nutrition in severely malnourished patients
Gastric decompression:
- Large-bore nasogastric or orogastric tube with lavage until stomach is completely emptied (may require repeated washes - the stomach can hold litres of stagnant food)
- This allows subsequent endoscopy and contrast imaging
H. pylori testing and treatment:
- Test (urea breath test or antral biopsy at endoscopy)
- Eradicate if positive: triple therapy (PPI + amoxicillin + clarithromycin × 14 days)
- IV/high-dose oral PPI to reduce acid secretion and allow oedema to resolve
Step 2: Medical Trial
In early/acute GOO (where oedema is the predominant component rather than fibrosis), aggressive medical management alone - NGT decompression + IV PPI + H. pylori eradication - may lead to complete resolution in up to 50% of cases and avoid surgery.
- Duration of medical trial: typically 5-7 days of NGT decompression + PPI
- Serial saline load tests can monitor improvement (<200 mL residual at 30 min = resolution)
Step 3: Endoscopic Management
Endoscopic balloon dilatation (EBD):
- Performed via OGD using through-the-scope (TTS) balloon catheters
- Serial dilatations (typically to 12-15 mm) may be required
- Effective in ~50% of patients with benign pyloric stenosis; may delay surgery for 1-2 years
- Best suited to early, predominantly oedematous stenosis; less effective in fibrotic strictures
- Must be combined with anti-ulcer therapy and H. pylori eradication
Duodenal stent:
- Self-expanding metallic stent (SEMS)
- Reserved for malignant GOO as palliation (unresectable pancreatic/gastric cancer) or as bridge to surgery
- Not appropriate for benign stenosis long-term (stent migration, overgrowth)
Step 4: Surgical Management
Indicated when:
- Medical therapy and EBD fail or are inappropriate
- Fibrotic/organic obstruction on imaging or endoscopy
- Malignancy cannot be excluded
- Recurrent obstruction after dilatation
Surgical options for benign pyloric stenosis:
1. Vagotomy and Antrectomy (V+A) - Gold Standard:
- Removes the obstructing antrum/pylorus + eliminates acid drive
- Reconstruction: Billroth II gastrojejunostomy (antecolic, isoperistaltic)
- Advantages: lowest ulcer recurrence, confirms benign pathology by specimen histology
- Disadvantage: higher operative mortality (~2%), technically demanding with difficult duodenal stump
- Chronically obstructed stomach has thick walls - use larger staple cartridges
- If duodenal stump closure is difficult: lateral duodenostomy, nasogastric/retrograde jejunostomy for decompression; omental buttress
2. Vagotomy and Gastrojejunostomy (V+GJ) - preferred in high-risk patients:
- Truncal vagotomy + posterior gastrojejunostomy (drainage procedure without resection)
- Advantages: lower operative mortality, reversible if severe dumping, readily laparoscopic
- Disadvantages: obstructing cancer may be missed; risk of marginal ulceration
- Suitable when duodenal dissection is hazardous (densely adherent, inflamed)
3. Highly Selective Vagotomy (HSV) + Gastrojejunostomy:
- Preserves antral innervation; lower dumping/diarrhoea rates
- Reserved for elective, fit patients with minimal operative risk
4. Pyloroplasty (Heineke-Mikulicz):
- For functional/early stenosis with minimal scarring; rarely used in true fibrotic stenosis
- Often combined with truncal vagotomy
PART C: MALIGNANT PYLORIC STENOSIS
When GOO is caused by gastric or pancreatic carcinoma:
- Resectable disease: Curative resection - distal gastrectomy (gastric cancer) or Whipple's procedure (pancreatic/duodenal cancer)
- Unresectable/metastatic disease - Palliation:
- Endoscopic duodenal stent (SEMS): Quicker symptom relief; preferred in patients with poor performance status or short expected survival
- Surgical gastrojejunostomy (palliative bypass): More durable; preferred in patients with better performance status and longer expected survival; can be done laparoscopically
- Chemotherapy ± radiotherapy per oncology protocol
Summary Algorithm
PYLORIC STENOSIS
├── INFANT (IHPS)
│ ├── Correct metabolic alkalosis (IV saline + KCl)
│ └── Fredet-Ramstedt pyloromyotomy (open/laparoscopic)
│
└── ADULT
├── Correct alkalosis + NGT decompression + IV PPI + H. pylori Rx
├── Medical trial (5-7 days) → resolve? → long-term PPI
├── Not resolved → Endoscopic balloon dilatation (serial)
└── Failed/fibrotic/malignant → SURGERY
├── Benign: V+A (gold standard) or V+GJ (high-risk)
└── Malignant: Resection OR palliation (stent/GJ bypass)
Key references:
- Schwartz's Principles of Surgery 11e, Ch. 39, pp. 1749-1750 (IHPS)
- Current Surgical Therapy 14e, Surgery for Obstructing Duodenal Ulcer, pp. 132-134
- Bailey & Love's Short Practice of Surgery 28e, Ch. 67, p. 1190
Clinical presentation, investigations and management of stage II carcinoma of stomach.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer:
Stage II Carcinoma of the Stomach: Clinical Presentation, Investigations, and Management
(Sources: Bailey & Love's Short Practice of Surgery 28e; Schwartz's Principles of Surgery 11e; Sabiston Textbook of Surgery 21e)
TNM STAGING - WHAT IS STAGE II?
Using the UICC/AJCC 8th Edition TNM system:
T staging:
- T1a: Invades lamina propria or muscularis mucosae
- T1b: Invades submucosa
- T2: Invades muscularis propria
- T3: Involves subserosa (without serosa breach)
- T4a: Perforates serosa (visceral peritoneum)
- T4b: Invades adjacent structures
N staging:
- N0: No nodal metastasis
- N1: 1-2 regional nodes
- N2: 3-6 regional nodes
- N3a: 7-15 nodes; N3b: ≥16 nodes
Stage II (locoregionally advanced, no distant metastasis, M0):
| Stage | T | N | M |
|---|---|---|---|
| IIA | T1 | N2 | M0 |
| IIA | T2 | N1 | M0 |
| IIA | T3 | N0 | M0 |
| IIB | T1 | N3a | M0 |
| IIB | T2 | N2 | M0 |
| IIB | T3 | N1 | M0 |
| IIB | T4a | N0 | M0 |
Key: Stage II = tumour beyond the submucosa OR limited nodal involvement, but no distant metastasis (M0). It is potentially curable disease.
5-year survival for stage II: approximately 40-65% (stage IIA better than IIB).
1. CLINICAL PRESENTATION
Stage II gastric cancer sits between "early" (T1, high curability) and "advanced" (T3-T4 with N+). Most patients at this stage have non-specific symptoms that overlap with benign dyspepsia - a high index of suspicion is essential.
Symptoms (in order of frequency):
Upper GI symptoms:
- Epigastric pain or discomfort - persistent, often dull, not relieved by antacids or food
- Dyspepsia / indigestion - may be indistinguishable from peptic ulcer disease early on
- Early satiety - due to loss of gastric compliance (diffuse infiltration) or tumour bulk reducing reservoir capacity
- Anorexia - common; often precedes significant weight loss
- Nausea and vomiting - especially with antral/pyloric tumours causing partial GOO
- Dysphagia - if tumour is at or near the gastro-oesophageal junction (GOJ)
- Haematemesis / melaena - from tumour ulceration and bleeding; may present as iron deficiency anaemia
Systemic symptoms:
- Weight loss - significant, often >10% body weight; due to anorexia, malabsorption, cancer cachexia
- Fatigue - from anaemia (chronic blood loss) or systemic effects of malignancy
Signs (may be absent in early stage II):
Local signs:
- Epigastric mass - may be palpable in thin patients with larger tumours
- Epigastric tenderness on palpation
- Succussion splash - if pyloric involvement causing partial GOO
Signs of lymph node spread (rare at Stage II but possible):
- Troisier's sign / Virchow's node - palpable left supraclavicular lymph node (Troisier's sign); indicates involvement of the thoracic duct → technically N+ but distant nodal spread is M1
- Sister Mary Joseph's nodule - umbilical nodule from peritoneal spread (more advanced)
Paraneoplastic / systemic signs:
- Trousseau's sign - migratory thrombophlebitis (hypercoagulable state from malignancy)
- Pallor (anaemia), cachexia
- Acanthosis nigricans - black velvety skin in flexures (rare paraneoplastic)
Note: Stage II by definition has M0 disease, so hepatomegaly (liver metastases), ascites, Krukenberg tumours (ovarian metastases), and Sister Joseph's nodule suggest more advanced (stage IV) disease.
2. INVESTIGATIONS
A. To Confirm Diagnosis
-
Upper GI endoscopy (OGD) - key investigation
- Visualises tumour: ulcerating, polypoid, infiltrating (linitis plastica)
- Multiple biopsies (≥8) from the edge and floor of the lesion - mandatory for histological confirmation
- Biopsies of adjacent antral mucosa for H. pylori
- Endoscopic classification: Borrmann types I-IV (macroscopic); Japanese early gastric cancer types
-
Biopsy and histopathology - confirms adenocarcinoma; Lauren classification:
- Intestinal type (well-differentiated, glandular; H. pylori-related; better prognosis)
- Diffuse type (poorly differentiated, signet ring cells; worse prognosis; CDH1 mutation in hereditary diffuse GC)
B. Staging Investigations
-
CT scan of chest, abdomen and pelvis (with IV contrast - triphasic) - primary staging tool:
- Assesses T stage (wall invasion depth), N stage (lymphadenopathy), M stage (liver metastases, lung, peritoneal disease)
- Distinguishes resectable from metastatic disease
-
PET-CT (FDG-PET) - recommended for T2 or above:
- Detects occult distant metastases not seen on CT
- Assesses response to neoadjuvant chemotherapy
- Note: FDG-PET has limited sensitivity for diffuse/signet ring cell type (low FDG uptake)
-
Endoscopic ultrasound (EUS) - most accurate for local T and N staging:
- Assesses depth of wall invasion (T stage) and perigastric node involvement
- EUS-FNA of suspicious nodes for cytological confirmation
- Particularly important when surgical planning depends on precise T stage
-
Diagnostic laparoscopy (with peritoneal washings):
- Recommended for all patients with locoregional (potentially resectable) disease (T1b or above) before curative surgery
- Detects peritoneal metastases not visible on CT (~20-30% of "stage II/III" patients on CT have peritoneal disease at laparoscopy)
- Positive peritoneal cytology = M1 disease (stage IV)
C. Haematological and Biochemical Investigations
- FBC - microcytic anaemia (chronic blood loss); baseline
- Serum albumin and total protein - nutritional assessment; hypoalbuminaemia indicates poor nutritional status
- LFTs + bilirubin - baseline; may indicate liver involvement
- Urea and electrolytes, creatinine - baseline renal function; important pre-chemotherapy
- Coagulation studies - pre-operative
- Blood group and crossmatch - pre-operatively
D. Tumour Markers
- CEA (carcinoembryonic antigen) - elevated in ~30-40%; useful for monitoring response and recurrence, not diagnostic
- CA 19-9 - may be elevated; useful in combination with CEA
- CA 72-4 - more specific for gastric cancer than CEA; useful in monitoring
- HER2 testing (IHC/FISH) on biopsy - mandatory: ~15-20% of gastric adenocarcinomas overexpress HER2; determines eligibility for trastuzumab (ToGA regimen)
- PD-L1 (CPS score) - important for immunotherapy eligibility (pembrolizumab)
- Microsatellite instability (MSI) testing - MSI-H tumours respond to checkpoint inhibitors
E. Cardiopulmonary Assessment (pre-operative)
- ECG, chest X-ray - baseline
- Echocardiogram / pulmonary function tests - if cardiac/respiratory comorbidity; particularly if using anthracycline-based chemotherapy (epirubicin)
3. MANAGEMENT
Stage II gastric cancer is treated with curative intent using a multimodal approach combining surgery, perioperative chemotherapy, and (in selected cases) radiotherapy.
A. Perioperative (Neoadjuvant + Adjuvant) Chemotherapy
Level 1 evidence supports perioperative chemotherapy for all operable (stage II-III) gastric cancers. Most operable patients should receive chemotherapy before and after surgery.
Regimen of choice - FLOT (current standard):
- Fluorouracil + Leucovorin + Oxaliplatin + Docetaxel (FLOT)
- 4 pre-operative cycles + 4 post-operative cycles
- Based on the FLOT4 trial: FLOT showed median OS of 50 months vs 35 months for the older ECF (epirubicin + cisplatin + 5-FU) regimen; significantly improved R0 resection rates and pathological response
Older regimen (still used when FLOT not tolerated):
- ECF/ECX (epirubicin + cisplatin + 5-FU or capecitabine) - based on MAGIC trial
- 3 pre-op + 3 post-op cycles; improved 5-year survival from 23% to 36%
Rationale for neoadjuvant chemotherapy:
- Downstages tumour (reduces T and N stage)
- Eliminates occult micrometastases
- Tests chemo-sensitivity
- Improves R0 resection rates
- Practical issue: <50% of patients in trials received the full post-operative component; hence emphasis on completing pre-operative cycles
B. Surgical Resection - the only curative treatment
Principle: Complete (R0) resection with adequate margins and adequate lymph node dissection (D2).
Type of resection depends on tumour location:
| Tumour Location | Operation |
|---|---|
| Distal third (antrum/pylorus) | Distal (subtotal) gastrectomy - preferred for T2-T3 distal tumours |
| Middle third (body) | Distal or total gastrectomy depending on margins |
| Proximal third / GOJ | Total gastrectomy ± oesophagectomy |
| Diffuse/linitis plastica | Total gastrectomy (mandatory) |
Resection margins:
- Proximal margin: ≥5 cm for diffuse type; ≥3 cm for intestinal type (or 2 cm for T1)
- Frozen section of margins performed intraoperatively if margin status uncertain
Lymph node dissection:
- D2 lymphadenectomy is the standard of care in curative-intent surgery (Japan, Korea, Europe)
- Removes perigastric nodes (stations 1-6) + nodes along the coeliac axis, left gastric, common hepatic, and splenic arteries (stations 7-11)
- Goal: ≥16 lymph nodes examined (NCCN) to ensure adequate staging
- Spleen-preserving D2 is standard; splenectomy added only if direct splenic or splenic hilar (station 10) involvement
Reconstruction after gastrectomy:
- After subtotal gastrectomy: Billroth I (gastroduodenostomy) or Roux-en-Y gastrojejunostomy
- After total gastrectomy: Roux-en-Y oesophagojejunostomy (alimentary limb ≥50 cm to prevent bile reflux)
Minimally invasive approach:
- Laparoscopic or robotic gastrectomy: equivalent oncological outcomes to open surgery for early and locally advanced disease; less blood loss, shorter hospital stay; increasing use globally
C. Adjuvant Therapy (post-operative)
-
Adjuvant chemotherapy (after surgery-first approach if neoadjuvant not given):
- Capecitabine + oxaliplatin (CAPOX) for 6 months - CLASSIC trial (Asia)
- S-1 (oral fluoropyrimidine) for 1 year - ACTS-GC trial (Japan)
-
Chemoradiotherapy (if R1 resection or D0/D1 surgery):
- Macdonald protocol (US INT-0116 trial): 5-FU/leucovorin + 45 Gy radiotherapy post-operatively
- Currently used mainly when D2 dissection not achieved or positive margins
-
Targeted therapy:
- Trastuzumab (anti-HER2): added to chemotherapy in HER2+ tumours (ToGA trial); applicable if metastatic disease develops
- Pembrolizumab (anti-PD-1): for MSI-H tumours or high PD-L1 CPS; increasingly used in first-line and adjuvant settings
D. Summary of Management Plan for Stage II Gastric Cancer
Stage II Gastric Cancer (M0, potentially resectable)
│
├── Pre-treatment staging: CT chest/abdomen/pelvis + EUS + diagnostic laparoscopy
│
├── Peritoneal cytology negative → PROCEED WITH CURATIVE INTENT
│
├── NEOADJUVANT CHEMOTHERAPY: FLOT × 4 cycles (3 months)
│
├── Re-staging CT ± EUS after neoadjuvant
│
├── SURGERY: R0 resection + D2 lymphadenectomy
│ ├── Distal: subtotal gastrectomy
│ └── Proximal/diffuse: total gastrectomy + Roux-en-Y
│
├── ADJUVANT CHEMOTHERAPY: FLOT × 4 cycles (complete perioperative protocol)
│
└── SURVEILLANCE: CT every 6-12 months; OGD at 1 year; nutritional support
Key Points for Exam
- Stage II = locoregional disease (T1-T4a, N0-N3a, M0); potentially curable
- The FLOT4 trial established FLOT as the preferred perioperative regimen (50 vs 35 months median OS vs ECF)
- Diagnostic laparoscopy is mandatory before curative surgery; positive peritoneal cytology = M1 (stage IV) → palliative intent
- D2 lymphadenectomy with ≥16 nodes examined is the surgical standard
- HER2 testing and MSI testing are mandatory at diagnosis for targeted/immunotherapy planning
- 5-year survival for stage II: ~40-65% (varies by substage)
Key references:
- Bailey & Love's Short Practice of Surgery 28e, Ch. 67, pp. 1191-1197 (Table 67.6, UICC 8th edition TNM)
- Schwartz's Principles of Surgery 11e, Ch. 26, pp. 1145-1160
- Sabiston Textbook of Surgery 21e, Ch. 49 (Gastric Cancer)
This is a shared conversation. Sign in to Orris to start your own chat.