Describe rabies
Reading File
Finding Sources
Searching PubMed
rabies virus pathogenesis clinical features
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Here is the full answer:
Rabies
Overview
Rabies is a near-universally fatal viral encephalitis caused by a neurotropic RNA virus (genus Lyssavirus, family Rhabdoviridae). It causes approximately 55,000 deaths per year worldwide, with the vast majority occurring in Asia and Africa. Once clinical disease appears, mortality approaches 100%.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1675
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1169
Etiology and Transmission
The rabies virus is transmitted primarily through the bite or scratch of an infected animal. Key reservoir species include:
- Dogs - the most common source globally
- Wild carnivores - skunks, foxes, raccoons, coyotes, wolves
- Bats - the dominant source in the United States; exposure without a recognized bite can still transmit infection due to the ability of bat rabies variants to infect epithelial cells and fibroblasts
Rare routes of transmission include aerosol exposure (documented in bat-inhabited caves and laboratory accidents) and organ transplantation - in 2004, four recipients of kidneys, a liver, and an arterial segment from a single donor died of rabies within a month of surgery, with the donor retrospectively found to have had a possible bat bite.
Pathogenesis and Incubation
After inoculation at the wound site, the virus travels centripetally along peripheral nerves to the CNS. Because the distance between the wound and the brain determines how long this journey takes, the incubation period depends on wound location:
- Typical range: 1 to 3 months
- Possible range: 1 week to several years
- Bites to the face or head carry shorter incubation periods than distal extremity wounds
Once in the CNS, the infection is most severe in the brainstem and limbic system, with secondary involvement of basal ganglia, spinal cord, and dorsal root ganglia.
Pathology (Morphology)
Gross brain examination shows intense edema and vascular congestion. Microscopically:
- Widespread neuronal degeneration with inflammatory infiltration, worst in the brainstem
- Negri bodies - the pathognomonic finding: cytoplasmic, round-to-oval, eosinophilic inclusion bodies found in:
- Pyramidal neurons of the hippocampus
- Purkinje cells of the cerebellum
- These sites are characteristically devoid of inflammation despite containing inclusions
- Rabies virus can be detected within Negri bodies by ultrastructural and immunohistochemical methods
Below is a histological image of rabies encephalitis showing a Negri body (arrow) in a Purkinje cell:
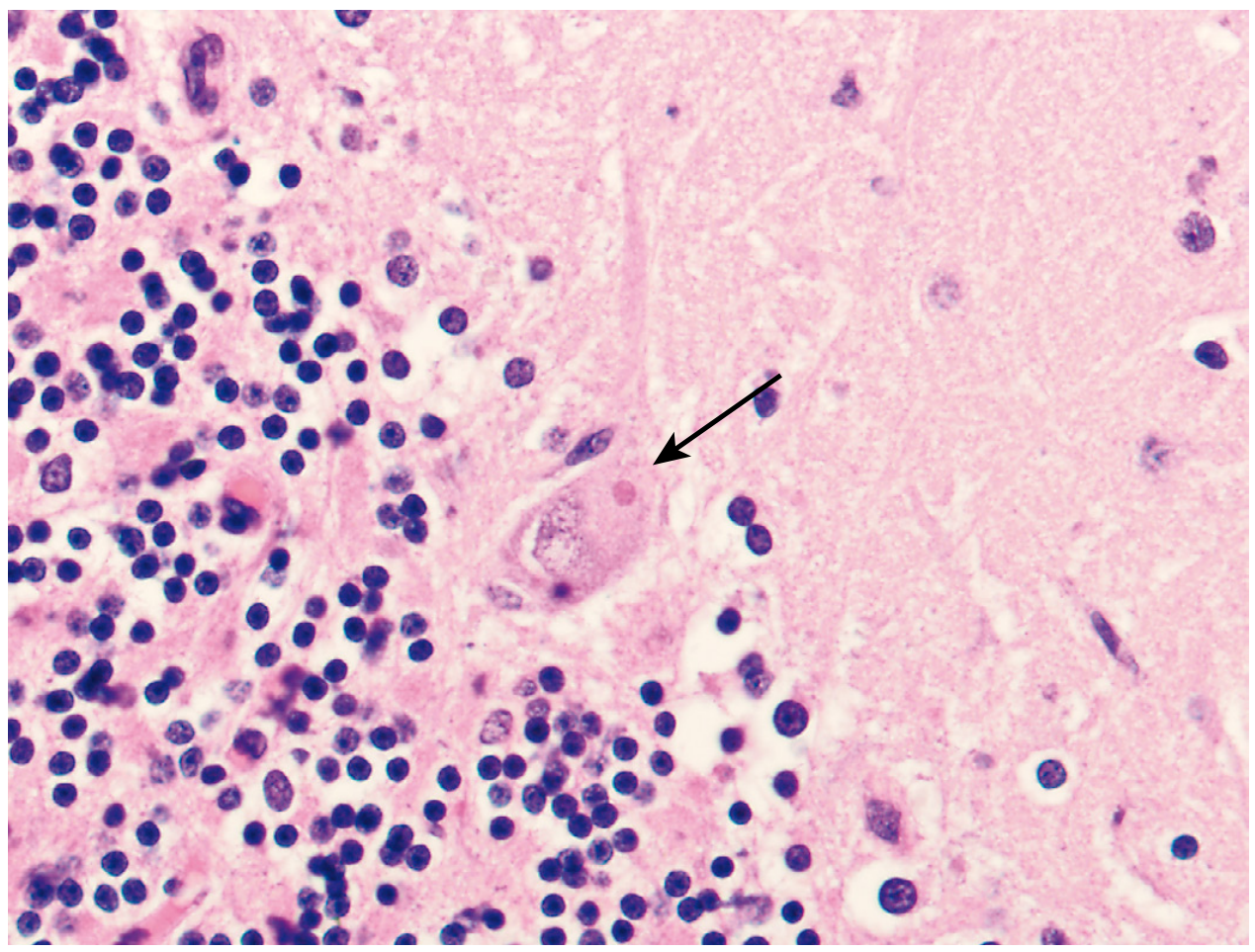
Robbins Pathology, Fig. 28.27 - Eosinophilic Negri body visible in a Purkinje cell (arrow)
Clinical Features
Prodrome
- Malaise, headache, fever
- Local paresthesias and pain at the inoculation site - highly suggestive when combined with the above
Acute Neurological Phase
Two main clinical forms:
| Feature | Furious (Encephalitic) Rabies | Paralytic ("Dumb") Rabies |
|---|---|---|
| Frequency | ~80% | ~20% |
| Hallmark | Hyperexcitability, agitation | Flaccid paralysis |
| Progression | Spasms → seizures → coma | Ascending paralysis → quadriplegia |
Key features of furious rabies:
- Hydrophobia - spasm of pharyngeal and nuchal muscles triggered by swallowing; present in up to 80% of patients
- Aerophobia - similar spasms triggered by air currents
- Spasms last 1-5 minutes and are triggered by touch, sound, light, or smell
- Hyperthermia (body temperature may reach 105-107°F)
- Autonomic hyperactivity, hallucinations, seizures
- Agitated delirium progressing to coma
Paralytic rabies is characterized by paresthesias, weakness, and flaccid paralysis beginning in the bitten extremity and progressing to quadriplegia - it can mimic Guillain-Barré syndrome.
MRI findings (FLAIR/T2): gray matter involvement of basal ganglia, thalamus, midbrain, and pontine nuclei.
CSF: Mononuclear pleocytosis in >50% during the first week, rising to 87% beyond the first week.
Diagnosis
Rabies should be considered in any patient with rapidly progressive encephalitis progressing to coma, especially after travel to endemic regions, even without a known bite history.
Antemortem tests:
- Nuchal (posterior neck) skin biopsy - immunofluorescence for rabies antigen in nerve fibers around hair follicles; fastest and most reliable
- Saliva RT-PCR - sensitive for detecting viral RNA
- Neutralizing antibodies in serum and CSF of an unimmunized patient - diagnostic, but appear late
- Corneal smears - low sensitivity, rarely used
Differential diagnosis includes:
- Tetanus (shorter incubation <2 weeks, normal CSF, no encephalitis)
- Other viral encephalitides
- Intoxications
- Postvaccinal encephalitis
- Rabies phobia (hysterical response to animal bite)
Post-Exposure Prophylaxis (PEP)
PEP is the cornerstone of preventing death after exposure. It is nearly 100% effective when initiated promptly.
Step 1 - Wound care:
- Thorough washing with soap and water
- Application of povidone-iodine
Step 2 - Active immunization (vaccine):
- Human diploid cell vaccine (HDCV) or purified chick-embryo cell vaccine (PCEC)
- Given IM into deltoid or anterolateral thigh on days 0, 3, 7, and 14 (4-dose regimen for unvaccinated)
- Previously immunized: booster on days 0 and 3 only
Step 3 - Passive immunization (for unvaccinated individuals):
- Human rabies immunoglobulin (HRIG) at 20 IU/kg, given once as soon as possible after exposure (up to 7 days after the first vaccine dose)
- Infiltrate as much as possible into and around the wound; remaining dose given IM at a site distant from the vaccine
- Do not exceed the recommended dose (suppresses active antibody production)
Animal observation: A dog, cat, or ferret with a current rabies vaccination can be observed for 10 days rather than euthanized.
Pre-Exposure Prophylaxis (PreP)
Indicated for travelers to endemic regions (Latin America, Asia, Africa) where post-exposure resources are limited, and for high-risk occupational groups (veterinarians, spelunkers, laboratory workers).
- The WHO endorses a 2-dose schedule for pre-exposure prophylaxis
- A 3rd dose or antibody titer check is recommended at 1-3 years to assure long-term boostability
Prognosis
Once clinical signs develop, rabies is almost invariably fatal. A handful of survivorship cases exist (most famously the "Milwaukee Protocol"), but these remain exceptional and no reliable treatment for established rabies encephalitis exists.
Sources: Bradley and Daroff's Neurology in Clinical Practice | Robbins, Cotran & Kumar Pathologic Basis of Disease | Goldman-Cecil Medicine | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.