Aub /dub
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough breakdown of the "lub dub" (S1/S2) heart sounds, drawn from Guyton & Hall and Harrison's:
The Heart Sounds: "Lub Dub"
S1 - "Lub" (First Heart Sound)
S1 marks the start of ventricular systole. It is produced by closure of the mitral (bicuspid) and tricuspid valves (the atrioventricular valves). The mechanism is:
- Ventricular contraction causes a sudden backflow of blood against the AV valves.
- The valves close and bulge toward the atria until the chordae tendineae stop the backward movement.
- The elastic recoil bounces blood forward into the ventricles, creating vibrations in the blood, valve leaflets, and ventricular walls - these travel to the chest wall as sound.
S1 is lower pitched and slightly longer (~0.14 sec) than S2, because the AV valves are less taut and the ventricles are less elastic vibrating chambers.
Auscultation: Best heard at the cardiac apex (mitral area) and lower left sternal border (tricuspid area).
S2 - "Dub" (Second Heart Sound)
S2 marks the end of ventricular systole. It is produced by closure of the aortic and pulmonic valves (the semilunar valves). The mechanism is:
- At the end of systole, blood flows back from the aorta/pulmonary artery toward the ventricles.
- This closes the semilunar valves, which bulge back toward the ventricles.
- Blood rebounds back and forth between the arterial walls and the valves, creating vibrations that radiate along the arteries to the chest wall.
S2 is shorter (~0.11 sec) and higher pitched than S1, because the semilunar valves are tauter and the arterial walls are stiffer, producing briefer, higher-frequency vibrations.
S2 has two components:
- A2 - aortic valve closure (normally first)
- P2 - pulmonic valve closure (normally slightly after A2)
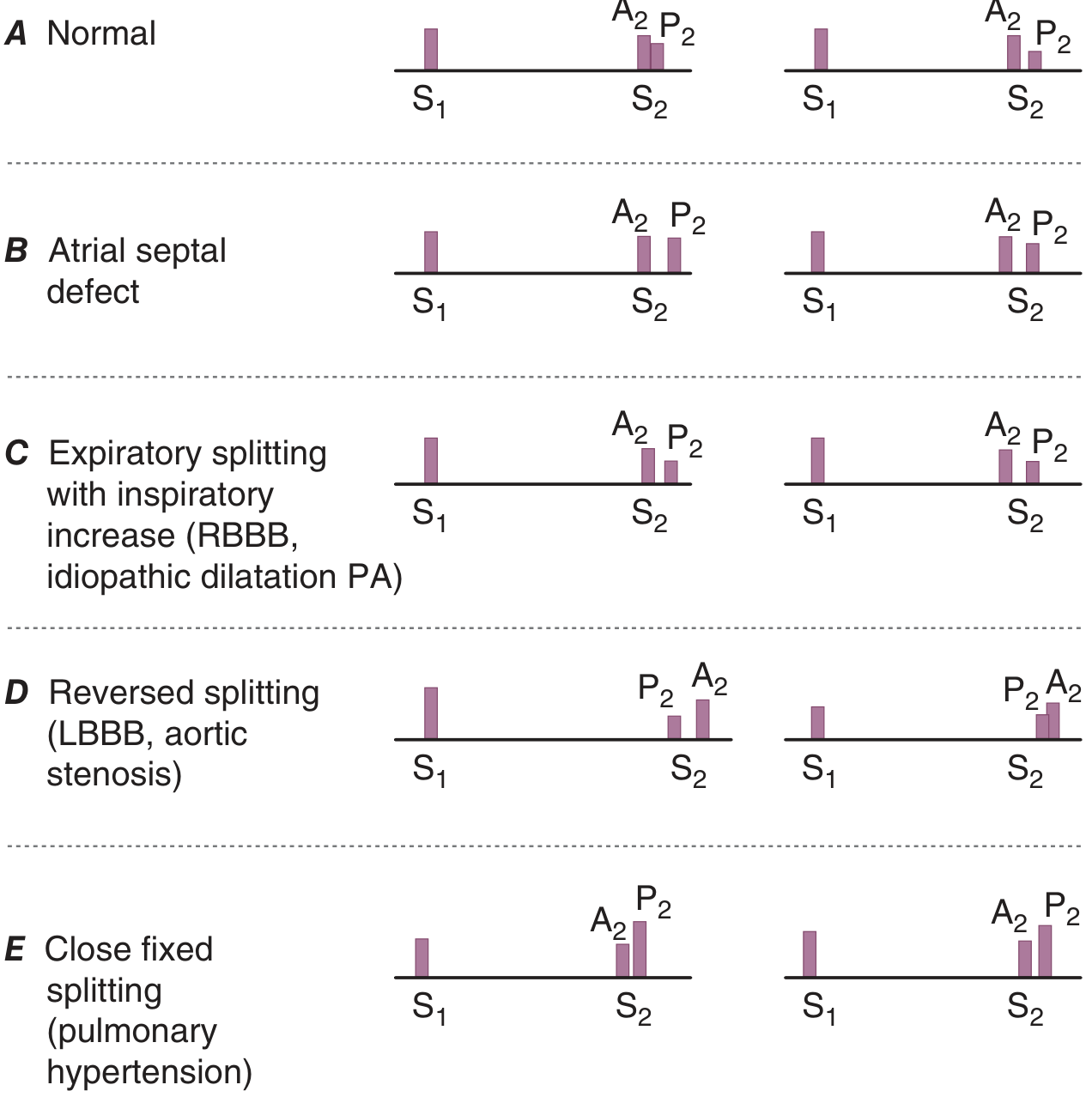
Splitting of S2
Under normal conditions, A2 precedes P2. Their gap widens on inspiration (increased venous return to the right heart delays P2) and narrows on expiration - this is called physiologic splitting.
| Pattern | Condition |
|---|---|
| Normal (physiologic) splitting | A2 before P2, increases with inspiration |
| Wide fixed splitting | Atrial septal defect (ASD) |
| Wide splitting (RBBB pattern) | Right bundle branch block, idiopathic PA dilatation |
| Reversed / paradoxical splitting | Left bundle branch block, aortic stenosis, HOCM |
| Narrow / single S2 | Pulmonary hypertension |
The Third and Fourth Heart Sounds (S3, S4)
- S3 ("ventricular gallop"): Heard in early diastole, caused by rapid ventricular filling. Physiologic in children and young adults. Pathologic in heart failure (suggests elevated filling pressures / dilated, non-compliant ventricle).
- S4 ("atrial gallop"): Heard just before S1, caused by a forceful atrial contraction pushing blood into a stiff ventricle (e.g., LVH, hypertensive heart disease, aortic stenosis). Always pathologic.
Quick Clinical Summary
| Sound | Timing | Cause | Pitch/Duration |
|---|---|---|---|
| S1 ("lub") | Start of systole | Mitral + tricuspid closure | Low, ~0.14 sec |
| S2 ("dub") | End of systole | Aortic + pulmonic closure | Higher, ~0.11 sec |
| S3 | Early diastole | Rapid ventricular filling | Low |
| S4 | Late diastole (pre-S1) | Atrial kick into stiff ventricle | Low |
- Guyton and Hall Textbook of Medical Physiology, Normal Heart Sounds section
- Harrison's Principles of Internal Medicine 22E, Cardiac Auscultation
This is a shared conversation. Sign in to Orris to start your own chat.