A person came in my OPD with elevated blood sugar level 126 and elevated LDL level with 155 with a family history of past heart diseases. What should I do?
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
diabetes AND dyslipidemia AND cardiovascular risk reduction statin
I now have comprehensive information to provide a thorough clinical response. Here is a structured management plan:
Clinical Assessment & Management Plan
This patient presents with three simultaneous cardiovascular risk issues that must be addressed together:
| Parameter | Patient's Value | Threshold | Interpretation |
|---|---|---|---|
| Fasting Plasma Glucose | 126 mg/dL | ≥126 mg/dL | Diabetes Mellitus (ADA criteria) |
| LDL-C | 155 mg/dL | See risk stratification | Elevated — requires treatment |
| Family history of heart disease | Present | — | ASCVD Risk Enhancer |
Step 1 — Confirm the Diagnosis
Before starting treatment, confirm the diabetes diagnosis:
- Repeat fasting plasma glucose on a separate day (required unless the patient has overt hyperglycemia symptoms like polyuria, polydipsia, polyphagia).
- Order HbA1c — a value ≥6.5% confirms diabetes and gives a 3-month average glucose picture.
- Order a full lipid panel if not already done (Total cholesterol, HDL, TG, LDL).
"A fasting plasma glucose of ≥126 mg/dL (7.0 mmol/L)... is consistent with a diagnosis of diabetes... if the patient does not have overt signs of hyperglycemia, repeat testing should be performed as soon as possible to confirm." — Lippincott Illustrated Reviews: Pharmacology
Step 2 — Cardiovascular Risk Stratification (ASCVD)
This patient has multiple risk enhancers:
- Family history of premature ASCVD (a major risk enhancer per 2018 ACC/AHA guidelines)
- Diabetes mellitus (newly diagnosed)
- Elevated LDL-C 155 mg/dL
Calculate the 10-year ASCVD risk score (Pooled Cohort Equations). Given the combination of diabetes + family history + elevated LDL, this patient likely falls into intermediate-to-high risk, warranting statin therapy.
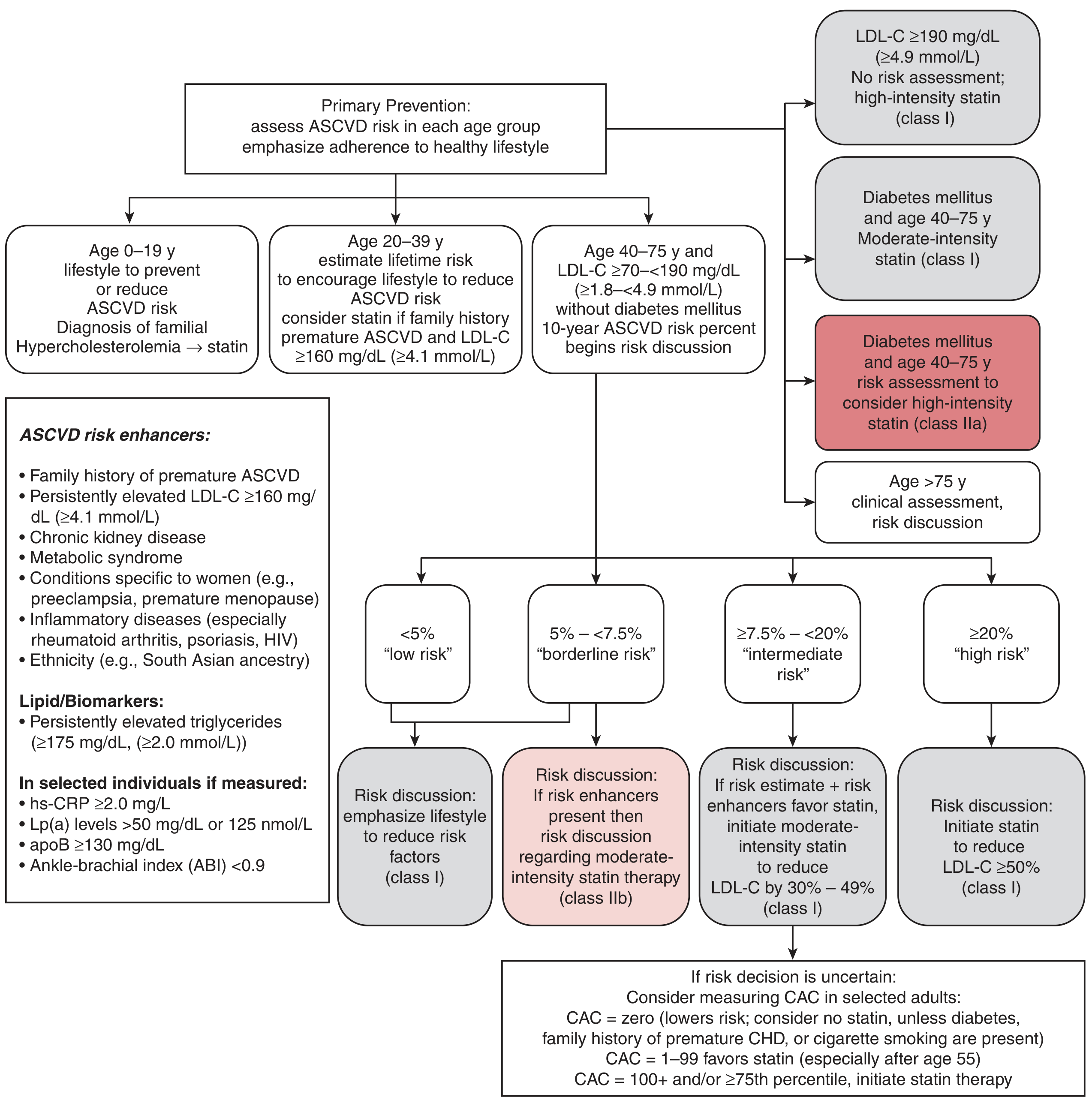
Primary ASCVD Prevention Strategy (2018 ACC/AHA):
Step 3 — Diabetes Management
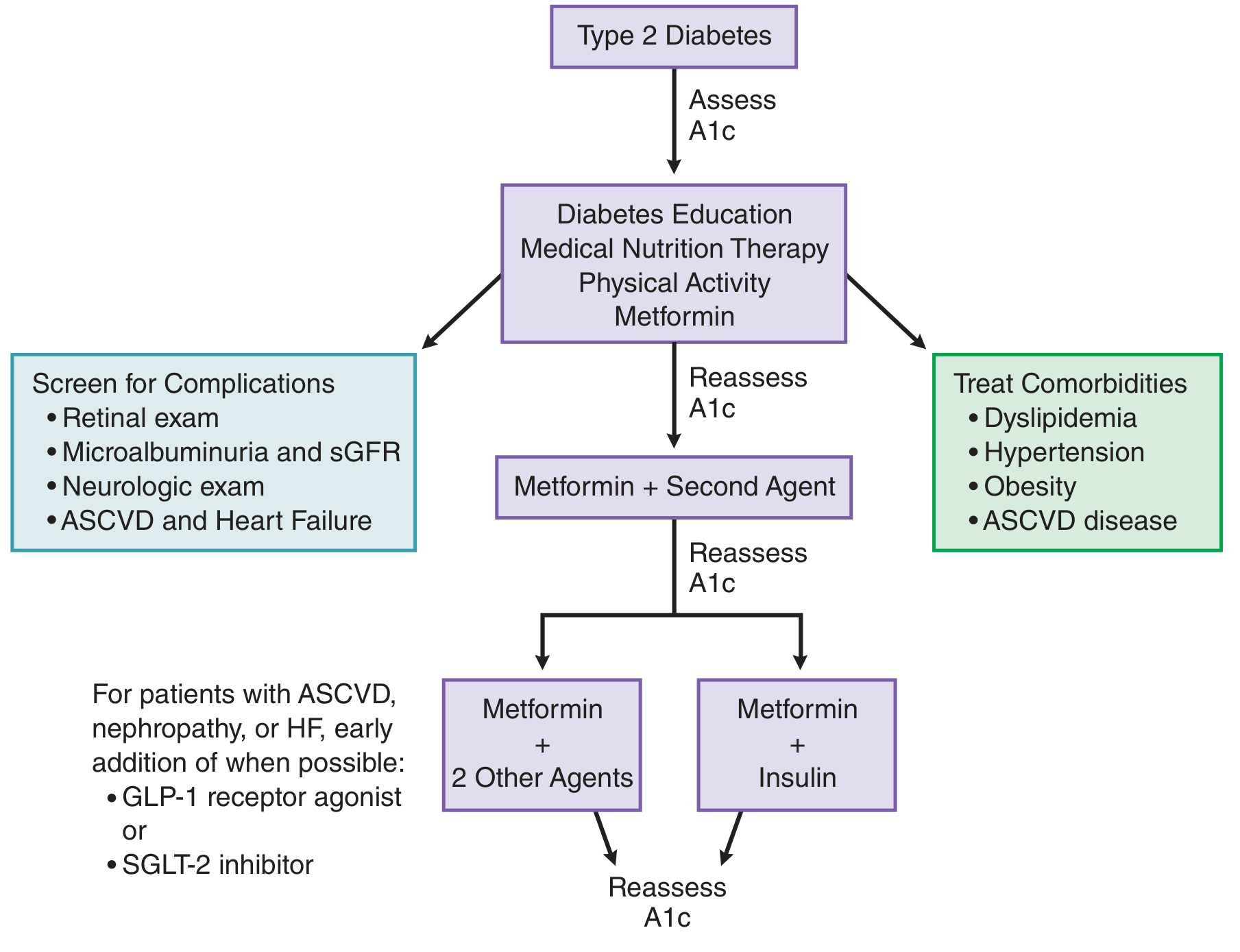
Treatment Algorithm for Type 2 Diabetes:
First-Line Pharmacotherapy:
- Metformin — first-line consensus drug for Type 2 DM; improves insulin sensitivity; preferred in overweight patients; start at diagnosis alongside lifestyle changes.
- Typical starting dose: 500 mg BD with meals, titrate to 1000 mg BD over 4–8 weeks.
- Check renal function (eGFR) before starting — contraindicated if eGFR <30.
Lifestyle Interventions (start simultaneously):
- Medical nutrition therapy: low glycemic index diet, reduced saturated fat and cholesterol
- Physical activity: ≥150 min/week of moderate aerobic exercise
- Weight management if overweight
Glycemic Target:
- HbA1c goal: ≤7% for most patients (reassess every 3 months initially)
Additional agents to consider given ASCVD risk:
Given the cardiovascular risk profile (family history of heart disease + new diabetes), consider early addition of:
- GLP-1 receptor agonist (e.g., semaglutide, liraglutide) — proven cardiovascular benefit in diabetics with high ASCVD risk
- SGLT-2 inhibitor (e.g., empagliflozin, dapagliflozin) — preferred if heart failure or diabetic nephropathy develops
Step 4 — Dyslipidemia (LDL = 155 mg/dL) Management
Per the ACC/AHA 2018 guidelines:
- Patient age 40–75 + Diabetes + LDL 70–189 mg/dL → Moderate-intensity statin (Class I recommendation)
- With family history of premature ASCVD as a risk enhancer → Upgrade to High-intensity statin (Class IIa)
Statin options:
| Intensity | Drug | Dose | Expected LDL Reduction |
|---|---|---|---|
| Moderate | Atorvastatin | 10–20 mg/day | 30–49% |
| Moderate | Rosuvastatin | 5–10 mg/day | 30–49% |
| High | Atorvastatin | 40–80 mg/day | ≥50% |
| High | Rosuvastatin | 20–40 mg/day | ≥50% |
LDL target in this patient (primary prevention with diabetes + risk enhancers): LDL-C <70 mg/dL is a reasonable goal (per ESC/EAS); US guidelines target ≥50% reduction from baseline.
If LDL remains above goal after maximally tolerated statin:
- Add ezetimibe 10 mg/day (additive LDL reduction ~18–20%)
- Consider PCSK9 inhibitors if LDL goal still not reached
"Low/moderate-intensity statin + ezetimibe combination therapy demonstrated comparable efficacy to high-intensity statin monotherapy with fewer adverse effects." — [BMC Cardiovascular Disorders 2024, PMID: 39567875]
Step 5 — Investigations to Order Now
| Investigation | Purpose |
|---|---|
| HbA1c | Confirm diabetes, baseline glycemic control |
| Fasting lipid panel (repeat) | Full ASCVD risk assessment |
| eGFR / Serum creatinine | Before starting metformin |
| Urine microalbumin/creatinine ratio | Screen for early diabetic nephropathy |
| Fasting insulin / HOMA-IR | Assess insulin resistance |
| Liver function tests | Before statin initiation |
| Blood pressure | Essential ASCVD risk factor |
| Resting ECG | Baseline cardiac assessment given family history |
| Uric acid, TSH | Exclude secondary causes of dyslipidemia |
Step 6 — Follow-Up Plan
- 4–8 weeks: Review HbA1c response, fasting glucose, metformin tolerability, LFTs post-statin
- 3 months: HbA1c reassessment — if not at goal (≤7%), add second agent
- 6 months: Repeat fasting lipid panel; assess LDL target achievement
- Annual: Retinal exam, foot exam, microalbuminuria, eGFR, ECG
Summary of Immediate Actions
- Confirm diabetes — repeat FBS or check HbA1c
- Start Metformin + intensive lifestyle counseling
- Calculate 10-year ASCVD risk score
- Initiate statin — moderate- to high-intensity given diabetes + family history; aim LDL <70 mg/dL
- Order baseline labs (HbA1c, lipid panel, eGFR, LFTs, urine microalbumin, ECG)
- Counsel patient on diet, physical activity, smoking cessation, BP monitoring
- Consider early GLP-1 agonist or SGLT-2 inhibitor given elevated ASCVD risk profile
Sources: Lippincott Illustrated Reviews Pharmacology; Goodman & Gilman's Pharmacological Basis of Therapeutics; Tietz Textbook of Laboratory Medicine 7th Ed.; Braunwald's Heart Disease
Hba1c is 6
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
This is an important clarification. Here is the updated assessment:
Updated Assessment: HbA1c = 6.0% — This is Prediabetes, NOT Diabetes
| Test | Patient Value | Diabetes Threshold | Prediabetes Range | Your Patient |
|---|---|---|---|---|
| Fasting Glucose | 126 mg/dL | ≥126 mg/dL | 100–125 mg/dL | Borderline — meets glucose threshold |
| HbA1c | 6.0% | ≥6.5% | 5.7–6.4% | Prediabetes |
How to Interpret This Discordance
The fasting glucose of 126 mg/dL meets the numeric threshold for diabetes, but the HbA1c of 6.0% falls squarely in the prediabetes range (5.7–6.4%). These two tests can give discordant results. Per ADA guidelines (Standards of Care 2024):
- Diagnosis requires confirmation by repeat testing — either a second fasting glucose ≥126 on a separate day, OR a second test (OGTT or repeat HbA1c) that confirms diabetes.
- Since the HbA1c does not confirm diabetes (it confirms prediabetes), this patient does not yet meet diagnostic criteria for diabetes based on dual-test confirmation.
"Patients with borderline elevated fasting glucose (100–125 mg/dL), postprandial glucose (140–199 mg/dL), or A1C 5.7% to 6.4% are considered to have prediabetes." — Lippincott Illustrated Reviews: Pharmacology
Revised Management Plan
1. Confirm or Exclude Diabetes
- Order OGTT (75g oral glucose tolerance test) — the gold standard when fasting glucose and HbA1c are discordant.
- 2-hour post-load glucose ≥200 mg/dL → confirms diabetes
- 2-hour post-load glucose 140–199 mg/dL → confirms prediabetes (IGT)
- <140 mg/dL → normal glucose tolerance
- Repeat fasting plasma glucose on a separate day to verify the 126 mg/dL value
2. Current Status: Treat as High-Risk Prediabetes
This patient has a very high-risk prediabetes profile:
- HbA1c 6.0% (upper end of prediabetes — close to diabetes threshold)
- Fasting glucose at the diabetes boundary
- Elevated LDL 155 mg/dL
- Family history of heart disease
3. Diabetes Prevention — Lifestyle Intervention (Priority #1)
This is the most powerful intervention at the prediabetes stage:
| Intervention | Target | Evidence |
|---|---|---|
| Weight loss | ≥5–7% body weight if overweight | Diabetes Prevention Program: 58% reduction in progression to T2DM |
| Physical activity | ≥150 min/week moderate aerobic exercise | Reduces insulin resistance directly |
| Dietary modification | Low glycemic index, reduced saturated fat, high fiber | Reduces postprandial glucose spikes |
| Smoking cessation | If applicable | Independent CV risk factor |
4. Consider Metformin for Prediabetes Prevention
Per ADA guidance, Metformin is appropriate for prediabetes when:
- HbA1c is in the 5.7–6.4% range (especially closer to 6.4%)
- Age 25–59 with BMI ≥35
- History of gestational diabetes, or
- Fasting glucose persistently ≥110 mg/dL
At HbA1c 6.0% with a borderline fasting glucose and a high cardiovascular risk profile, a strong case can be made to start Metformin (500 mg once daily, titrating to 500 mg BD) alongside lifestyle changes. Discuss this with the patient.
5. Dyslipidemia & ASCVD Risk — Statin Therapy (Unchanged)
The cardiovascular risk management does not change based on HbA1c reclassification. This patient still has:
- LDL 155 mg/dL
- Family history of premature heart disease (major ASCVD risk enhancer)
- Prediabetes / metabolic syndrome features
Recommendation: Initiate a moderate-intensity statin (e.g., Atorvastatin 10–20 mg/day or Rosuvastatin 5–10 mg/day). Family history of premature ASCVD alone is sufficient justification per ACC/AHA guidelines regardless of diabetes status. Target LDL reduction ≥30–50%.
Summary of Immediate Actions
| Priority | Action |
|---|---|
| 1 | Order OGTT to resolve the glucose/HbA1c discordance |
| 2 | Intensive lifestyle counseling — diet, exercise, weight loss |
| 3 | Consider Metformin for prediabetes prevention (shared decision-making) |
| 4 | Start moderate-to-high intensity statin for elevated LDL + family history |
| 5 | Reassess HbA1c in 3–6 months to track progression |
| 6 | Annual screening — repeat FPG, HbA1c, lipid panel, BP |
The critical message: at HbA1c 6.0%, this patient is at the highest-risk window for prevention — aggressive lifestyle intervention now can realistically halt progression to overt diabetes. The cardiovascular risk from LDL + family history needs pharmacological management now.
This is a shared conversation. Sign in to Orris to start your own chat.