Tell me all details about Anesthesia Machine
Reading File
Finding Sources
Finding Sources
Searching the Web
anesthesia machine components workstation detailed overview
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Now I have all the comprehensive information I need to deliver a detailed, well-structured answer. Let me compile everything.
The Anesthesia Machine (Anesthesia Workstation)
The modern anesthesia machine - more correctly called the anesthesia workstation - is the central piece of equipment for delivery of anesthesia in the operating room. It functions primarily to deliver respiratory support and volatile anesthetics to the patient, and has evolved from a simple gas-delivery device to a complex integrated system incorporating ventilators, monitors, and safety mechanisms.
"At its heart, the anesthesia machine remains a pneumatic system. It is where breathing gases are delivered from their supply sources, measured, mixed, enriched with anesthetic vapor, and delivered to the patient's breathing circuit."
- Miller's Anesthesia, 10e
Definition
The anesthesia workstation is defined by ASTM standard F1850-00 as a system for the administration of anesthesia to patients consisting of:
- The anesthesia gas supply device (the machine proper)
- Ventilator
- Monitoring devices
- Protection devices (safety systems)
The gas delivery system includes: the anesthesia machine, anesthetic vaporizers, ventilator, breathing circuit, and waste gas scavenging system.
Overview of the Three Pressure Sections
The entire gas supply system is divided into three pressure sections:
| Section | Pressure | Components |
|---|---|---|
| High-pressure | ~2000 psig (O₂/air); ~745 psig (N₂O) | E-cylinders only |
| Intermediate-pressure | 50-55 psig (pipeline); stepped down from cylinders | Pipeline inlets, pressure regulators, fail-safe valves, O₂ flush valve |
| Low-pressure | Below 14-35 psig | Flow control valves, flowmeters, vaporizers, fresh gas outlet |
Component 1: Gas Supply System
1A. High-Pressure Section - E-Cylinders
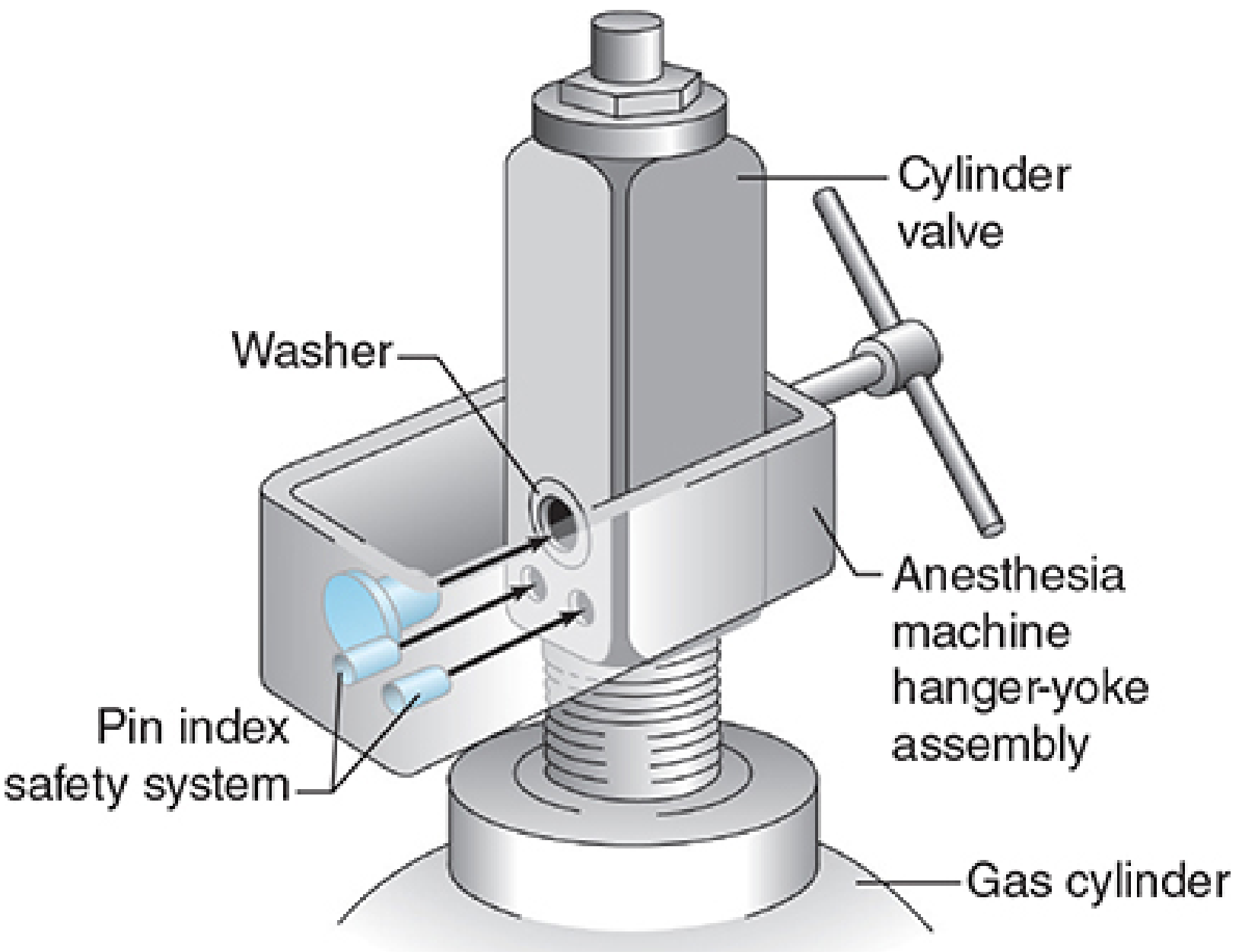
- Backup cylinders (E-cylinders) mount onto the back of the machine via the hanger yoke assembly
- Oxygen E-cylinders: ~2000 psig; Nitrous oxide: ~745 psig
- A pressure-reducing regulator steps down cylinder pressure to ~45 psig (intermediate level)
- The hanger yoke creates a gas-tight seal and ensures unidirectional gas flow into the machine
Pin Index Safety System (PISS): Two metal pins on the yoke project into specific holes on the cylinder valve head. Each gas has a unique pin arrangement, preventing wrong cylinder attachment. However, PISS is considered partial protection - label verification remains mandatory.
1B. Intermediate-Pressure Section - Pipeline Supply
- The primary gas source during normal operation is the hospital pipeline system (50-55 psig)
- Color-coded hoses (gas columns, ceiling hose drops, or articulating arms) connect to the machine via the Diameter Index Safety System (DISS) - which uses different thread sizes for each gas to prevent misconnection
- The oxygen supply failure protection device (commonly called a "fail-safe" valve) shuts off or proportionally reduces other gas flows (e.g., N₂O) when oxygen pressure drops - preventing accidental hypoxic mixtures
- Second-stage pressure regulators further reduce pressure to 14-35 psig for stable delivery to flow control valves
- The oxygen flush valve provides direct, high-flow O₂ (35-75 L/min) bypassing flowmeters and vaporizers; used in emergencies
1C. Low-Pressure Section
The most vulnerable to leaks. Contains:
- Flow control valves (needle valves)
- Flowmeters or electronic flow sensors
- Vaporizer manifold
- Anesthetic vaporizers
- Fresh gas outlet (common gas outlet, CGO)
Component 2: Flowmeters
- Classic Thorpe tubes are glass tubes containing a float (ball or bobbin) that rises in proportion to gas flow
- In modern workstations, these are replaced by electronic flowmeters - virtual displays controlled by microprocessors (e.g., Dräger Primus, GE Aisys)
- Oxygen flowmeter is always positioned downstream (closest to the patient circuit) - if an upstream flowmeter leaks, hypoxic gas cannot be preferentially delivered
- Flowmeters are agent-specific and temperature/pressure-dependent
Proportioning System: Workstations must prevent delivery of a hypoxic gas mixture. Two examples:
- Dräger SORC (Sensitive Oxygen Ratio Controller): pneumatic-mechanical interlock that maintains minimum 25% O₂ to 75% N₂O ratio
- GE Link-25 system: mechanically links O₂ and N₂O flow control chains so N₂O cannot exceed a set ratio
Component 3: Vaporizers
Vaporizers convert liquid volatile anesthetic into vapor at a clinically useful, accurately controlled concentration.
Types of Modern Vaporizers
| Type | Examples | Principle |
|---|---|---|
| Variable bypass (plenum) | Dräger Vapor 2000, GE Tec 7 | Splits gas - fraction diverted through liquid agent, remainder bypasses; mixed at outlet |
| Dual-circuit / measured flow | Desflurane vaporizer (Ohmeda Tec 6) | Special design due to desflurane's near-boiling point (22.8°C); agent is heated and pressurized separately |
| Cassette vaporizer | GE Aladin cassette | Agent-specific cassette inserted into a universal housing; electronically controlled |
| Injection vaporizer | Found in some electronic workstations | Liquid anesthetic injected directly into the gas stream |
Variable Bypass Vaporizer - Mechanism
- Fresh gas enters the inlet; the concentration control dial splits the flow between:
- Bypass chamber (no agent)
- Vaporizing chamber (contains liquid agent + wicks/baffles to maximize surface area)
- Gas passing through the vaporizing chamber becomes partially saturated with anesthetic vapor
- Both streams recombine at the outlet at the desired concentration
- A temperature-compensating device adjusts the splitting ratio as temperature changes (since vapor pressure is temperature-dependent)
- Vaporizers are agent-specific and calibrated at sea level
Vaporizer Interlock System: Prevents simultaneous use of more than one vaporizer. Each vaporizer is mounted on the manifold; activating one mechanically locks the others off.
Desflurane Vaporizer
Desflurane has a boiling point near room temperature (22.8°C), so its saturated vapor pressure approaches atmospheric pressure. A standard variable bypass vaporizer cannot be used safely. The Tec 6 heats the agent reservoir to 39°C (creating ~1500 mmHg pressure) and injects a precisely measured flow of desflurane vapor into the fresh gas stream.
Component 4: The Breathing Circuit
The breathing circuit connects the fresh gas outlet to the patient's airway, delivering the anesthetic gas mixture and allowing exhalation. The dominant circuit type is the circle system.
Circle System Components (in order of gas flow)
- Fresh gas inlet - from the machine's common gas outlet
- Inspiratory unidirectional valve - allows gas flow only toward the patient
- Inspiratory limb - corrugated tubing to the patient
- Y-piece connector - at the patient's airway (ETT/mask/LMA)
- Expiratory limb - corrugated tubing from patient
- Expiratory unidirectional valve - allows gas flow only away from patient
- CO₂ absorber - contains soda lime or Baralyme; removes exhaled CO₂ by chemical reaction (CO₂ + 2 NaOH → Na₂CO₃ + H₂O + heat)
- APL valve (Adjustable Pressure Limiting valve) - also called the pop-off valve; limits circuit pressure during spontaneous or manual ventilation; set to 0-70 cmH₂O
- Reservoir bag - acts as a buffer for variable patient demand; used for manual ventilation
Advantages of the circle system: Conservation of heat and humidity, reduced waste gas pollution, allows low fresh gas flows (less anesthetic consumption).
Fresh Gas Flow Rates
- High flow (>2 L/min): Used during induction/emergence; rapid agent changes
- Low flow (0.5-1 L/min): Used during maintenance; economical
- Minimal flow (<0.5 L/min): Rebreathing circuit; requires careful monitoring
Component 5: Ventilator
Modern anesthesia workstation ventilators are highly sophisticated and have replaced older simple bellows systems.
Bellows Types
- Ascending bellows (standing bellows): Rise during expiration. Safer - a circuit disconnect causes the bellows to fall, triggering an alarm
- Descending bellows (hanging bellows): Fall during expiration. Can continue cycling even if disconnected (entrain room air) - less preferred
Drive Mechanism
- Pneumatically driven: Pressurized gas (usually O₂ or air) compresses the bellows housing, which in turn compresses the patient gas within the bellows
- Piston ventilators: A motor-driven piston directly displaces gas; more precise, especially at low tidal volumes (useful for neonates)
- Electronic (turbine-driven): Used in many modern workstations; very precise control
Ventilation Modes Available
- Volume-controlled ventilation (VCV)
- Pressure-controlled ventilation (PCV)
- Pressure support ventilation (PSV)
- SIMV (Synchronized Intermittent Mandatory Ventilation)
- PEEP (Positive End-Expiratory Pressure) control
- Pressure-controlled ventilation with volume guarantee (PCV-VG)
Key Parameters
- Tidal volume, respiratory rate, I:E ratio, PEEP, FiO₂, pressure limits
Component 6: Waste Gas Scavenging System
Occupational exposure to anesthetic gases must be minimized. The scavenging system collects excess gas from the APL valve and ventilator relief valve and routes it away.
Components
- Gas collection assembly - tubing from APL valve and ventilator
- Transfer tubing (30 mm diameter - non-interchangeable with breathing circuit 22/15 mm)
- Interface (open or closed)
- Open interface: Open to atmosphere; no pressure relief valves needed; risk of occupational exposure
- Closed interface: Requires positive- and negative-pressure relief valves to protect patient from vacuum system pressures
- Disposal assembly - passive (vent to outside) or active (hospital vacuum system)
Active systems: Vacuum adjusted to evacuate 10-15 L/min; reservoir bag accepts overflow when vacuum capacity is exceeded.
Component 7: Safety Systems Summary
| Safety Feature | Purpose |
|---|---|
| Pin Index Safety System (PISS) | Prevents wrong cylinder connection |
| Diameter Index Safety System (DISS) | Prevents wrong pipeline connection |
| Fail-safe (O₂ supply failure protection) | Shuts off/reduces N₂O if O₂ supply fails |
| Proportioning system (SORC/Link-25) | Prevents hypoxic gas mixtures |
| O₂ analyzer / FiO₂ monitor | Continuous measurement of inspired O₂ |
| Vaporizer interlock | Prevents simultaneous use of two vaporizers |
| Ascending bellows | Alarms when circuit disconnects |
| Pressure alarms | High/low airway pressure alerts |
| APL valve | Limits excessive circuit pressure |
| Check valves in yoke assembly | Prevents backflow and cross-contamination between cylinders |
Component 8: Integrated Monitoring
Modern workstations incorporate or interface with:
| Monitor | Parameter |
|---|---|
| Pulse oximetry (SpO₂) | Oxygen saturation |
| Capnography (EtCO₂) | End-tidal CO₂; confirms ventilation and detects esophageal intubation |
| Inspired gas analysis | O₂, N₂O, volatile agent concentrations |
| Airway pressure monitor | Detects disconnection, obstruction |
| Spirometer (flow/volume) | Tidal volume, minute ventilation |
| MAC estimator | Minimum alveolar concentration of agent |
| Hemodynamic monitors | NIBP, ECG, temperature |
| Neuromuscular monitor | Train-of-four (TOF) ratio |
Pre-Use Checkout Procedure
The FDA and ASA mandate a pre-use checkout before every anesthetic. Key steps include:
- Verify backup O₂ cylinder pressure is adequate
- Check pipeline gas supplies (50-55 psig)
- Confirm all flowmeters function
- Test vaporizers (filled, no cross-filling)
- Test the O₂ analyzer (calibrate)
- Verify breathing circuit integrity and CO₂ absorber
- Perform low-pressure leak test
- Test ventilator (bellows movement, alarm function)
- Test APL valve
- Confirm waste gas scavenging connected
- Verify all monitors and alarms
- Confirm emergency ventilation equipment available
Modern machines perform automated self-tests that check circuit compliance, gas leakage, agent delivery, and ventilation systems - but manual verification remains mandatory.
Evolution: Traditional vs Modern Workstations
| Feature | Traditional | Modern (e.g., Dräger Apollo, GE Aisys) |
|---|---|---|
| Flowmeters | Glass Thorpe tubes | Virtual/electronic flowmeters on touchscreen |
| Gas mixing | Mechanical needle valves | Electronically controlled mixing |
| Vaporizer | Agent-specific, external | Cassette system or injection vaporizer |
| Ventilator | Simple bellows | Piston/turbine; multiple sophisticated modes |
| Monitoring | External, separate | Fully integrated into workstation |
| Machine check | Manual only | Automated + manual |
| CO₂ absorber | Fixed canister | Some auto-bypass for easy replacement |
Sources
- Sabiston Textbook of Surgery, 21e - Anesthesia Machine section
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapters on gas delivery, breathing circuits, scavenging
- Miller's Anesthesia, 10e - Chapter 20: Functional Anatomy of the Anesthesia Workstation
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Anesthesia equipment chapters
- NCBI StatPearls: Anesthesia Machine - Overview and function
- Anesthesia Key: The Anesthesia Workstation - Components reference
This is a shared conversation. Sign in to Orris to start your own chat.