Explain 10 common medical conditions and ECGs
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
ECG atrial fibrillation no P waves irregular rhythm
Searching Images
STEMI ST elevation myocardial infarction ECG
Searching Images
ventricular fibrillation ECG chaotic rhythm
Searching Images
complete heart block third degree AV block ECG P waves QRS dissociation
Searching Images
Wolff-Parkinson-White WPW ECG delta wave short PR interval
Searching Images
hyperkalemia ECG peaked T waves sine wave pattern
Searching Images
ventricular tachycardia wide complex tachycardia ECG
Searching Images
long QT syndrome ECG prolonged QT interval torsades de pointes
Searching Images
atrial flutter sawtooth waves ECG flutter waves 2:1 block
Searching Images
pulmonary embolism right heart strain ECG S1Q3T3 pattern
I now have comprehensive information from textbooks and medical images. Let me compile the full response.
10 Common Medical Conditions & Their ECG Findings
1. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized depolarization waves spread through both atria simultaneously. Because many waves are of opposite polarity at any given time, they electrically neutralize one another. The dilated atrial walls (from valve disease or ventricular failure) provide the ideal substrate — long conductive pathways and slow conduction. Blood stagnates in the left atrial appendage, creating thrombus and stroke risk. — Guyton & Hall Medical Physiology
Clinical features: Palpitations, dyspnea, fatigue, reduced cardiac output (~20–30% from loss of atrial kick). Most dangerous complication: embolic stroke.
ECG hallmarks:
- No organized P waves — replaced by fine fibrillatory (f) waves, best seen in V1
- Irregularly irregular R-R intervals (pathognomonic)
- Narrow QRS complexes (unless bundle branch block present)
- Ventricular rate varies (controlled: 60–100 bpm; rapid: >100 bpm)

Management: Rate control (beta-blockers, diltiazem), rhythm control (cardioversion, antiarrhythmics), anticoagulation (DOACs) to prevent stroke.
2. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Acute total occlusion of a coronary artery causes transmural myocardial ischemia. The territory distal to the occlusion progresses through injury → necrosis if not reperfused within 90–120 minutes.
Clinical features: Crushing chest pain, diaphoresis, nausea, radiation to jaw/arm. Troponin elevation follows ECG changes by 3–6 hours.
ECG hallmarks (evolving sequence):
- Hyperacute T waves (earliest — tall, peaked, broad-based)
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in ≥2 precordial leads — convex ("tombstone") morphology
- Pathological Q waves develop (>40 ms wide, >25% of R-wave height) — indicate necrosis
- Reciprocal ST depression in opposite leads
- T-wave inversion in the subacute phase
Localization by leads:
| Territory | Leads elevated | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | ST depression V1–V3 | RCA/LCx |

Management: Urgent PCI (door-to-balloon <90 min), antiplatelet therapy, anticoagulation, beta-blockers, statins.
3. Ventricular Fibrillation (VF)
Pathophysiology: Completely disorganized ventricular electrical activity — up to 30–50 small patches of myocardium contract asynchronously. No effective ventricular contraction occurs; cardiac output drops to zero. Without defibrillation, death within minutes. — Guyton & Hall Medical Physiology
Clinical features: Sudden collapse, pulselessness, loss of consciousness. Most common cause of sudden cardiac death. Precipitated by STEMI, cardiomyopathy, electrolyte imbalances, or preceding VT.
ECG hallmarks:
- Completely chaotic, irregular waveforms — no identifiable P waves, QRS, or T waves
- Rapid, undulating oscillations of varying amplitude and frequency
- Coarse VF (early): larger amplitude waves — more amenable to defibrillation
- Fine VF (late): low-amplitude waves decaying over minutes

Management: Immediate defibrillation (200 J biphasic), CPR, epinephrine, amiodarone per ACLS protocol.
4. Third-Degree (Complete) Heart Block
Pathophysiology: Total failure of conduction through the AV node — atrial impulses never reach the ventricles. The ventricles are driven by a slow escape pacemaker from the AV junction (narrow QRS, ~40–60 bpm) or ventricular myocardium (wide QRS, ~20–40 bpm). Causes include inferior STEMI, Lyme disease, calcific aortic valve disease, and medications.
Clinical features: Syncope (Stokes-Adams attacks), severe bradycardia, heart failure, hypotension. May present with sudden cardiac death if no escape rhythm.
ECG hallmarks:
- Complete AV dissociation — P waves and QRS complexes bear no relationship to each other
- P waves march at their own regular atrial rate (faster)
- QRS complexes fire at their own slower escape rate (regular but slow)
- Wide QRS if infra-Hisian escape; narrow QRS if junctional escape
- P waves may "march through" and be buried in QRS or T waves

Management: Urgent temporary pacing (transcutaneous or transvenous), followed by permanent pacemaker implantation.
5. Ventricular Tachycardia (VT)
Pathophysiology: Rapid, sustained ventricular rhythm (≥3 consecutive beats at ≥100 bpm) originating below the His bundle. Commonly arises from re-entry circuits around areas of ventricular scar (post-MI, cardiomyopathy). Hemodynamically stable VT can degenerate into VF.
Clinical features: Palpitations, syncope, presyncope, hypotension. May be asymptomatic in some structural heart disease patients. Pulseless VT = cardiac arrest.
ECG hallmarks:
- Wide QRS complexes (>120 ms), monomorphic (regular shape) or polymorphic
- Rapid regular rate (100–250 bpm)
- AV dissociation (P waves independent of QRS) — most specific sign
- Fusion beats and capture beats — pathognomonic
- Concordance in precordial leads (all positive or all negative V1–V6)
- QRS axis extremes ("northwest" axis: negative in I and aVF)
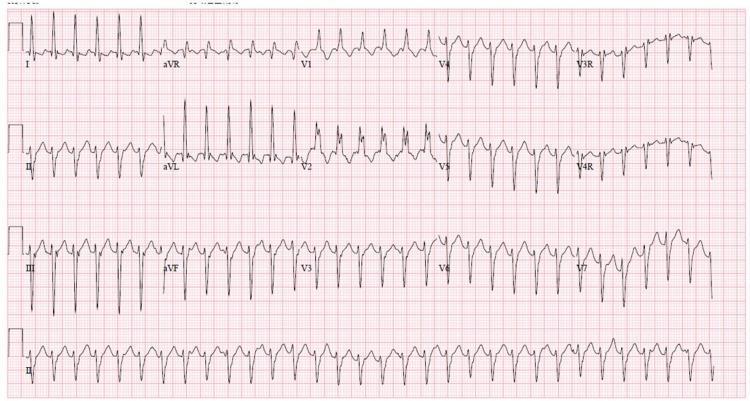
Management: Stable VT → amiodarone or cardioversion; unstable/pulseless → immediate defibrillation + ACLS.
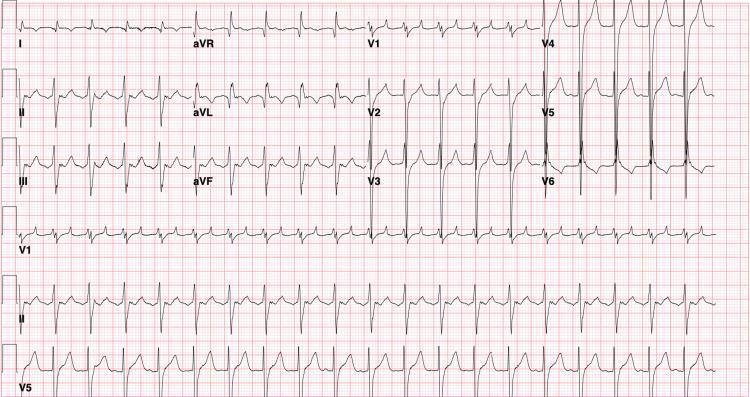
6. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, conducting impulses directly from atria to ventricles. This produces ventricular pre-excitation — part of the ventricle depolarizes early via the accessory pathway (producing the delta wave) while the rest depolarizes normally via the AV node. Orthodromic AVRT (most common), antidromic AVRT, and AF (potentially lethal at rates >300 bpm) can occur. — Tintinalli's Emergency Medicine
Clinical features: Palpitations, syncope, sudden cardiac death (rare). Affects ~1–3/1000 population; symptoms in ~50%.
ECG hallmarks (classic triad):
- Short PR interval (<120 ms) — AV node bypassed
- Delta wave — slurred upstroke at onset of QRS (early ventricular activation)
- Widened QRS complex (>120 ms total) — fusion of delta wave + normal conduction
- Secondary ST-T wave changes (discordant to QRS)
- Accessory pathway location can be inferred from delta wave polarity in different leads

Management: Acute SVT → adenosine or cardioversion. Avoid AV nodal blockers (verapamil, digoxin) in WPW with AF — may accelerate accessory pathway conduction and precipitate VF. Definitive treatment: radiofrequency catheter ablation.
7. Long QT Syndrome (LQTS)
Pathophysiology: Inherited or acquired channelopathy causing prolonged ventricular repolarization. Inherited forms (LQT1, LQT2, LQT3) involve mutations in cardiac K⁺ or Na⁺ channels. Acquired causes: drugs (sotalol, amiodarone, antipsychotics, macrolides), hypokalemia, hypomagnesemia, hypothyroidism. Prolonged repolarization creates a vulnerable window for early afterdepolarizations (EADs) triggering torsades de pointes (TdP). — Tintinalli's Emergency Medicine
Clinical features: Syncope (often exertional or emotion-triggered in LQT1/2), seizures, sudden cardiac death in young individuals with structurally normal hearts. Prevalence 1:2,000–5,000.
ECG hallmarks:
- Prolonged QTc >440 ms (men) / >460 ms (women) — corrected using Bazett's formula
- Abnormal T-wave morphology: broad/notched T waves (LQT1), biphasic/notched T wave (LQT2), late-onset T wave (LQT3)
- T-wave alternans in severe cases — beat-to-beat alternation in T-wave morphology (high-risk marker)
- Torsades de pointes: polymorphic VT with characteristic "twisting" of QRS complexes around the isoelectric baseline
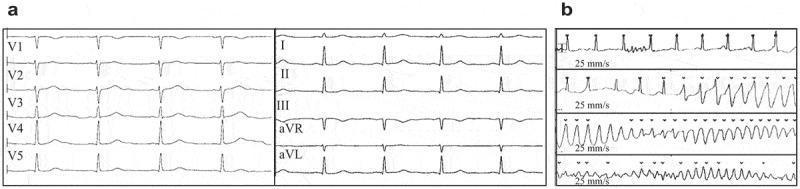
Management: Avoid QT-prolonging drugs and electrolyte disturbances. Beta-blockers (LQT1/2), mexiletine (LQT3), ICD for high-risk patients, left cardiac sympathetic denervation.
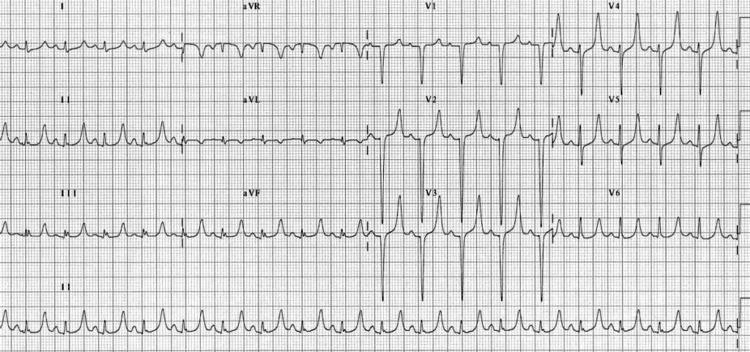
8. Atrial Flutter
Pathophysiology: Macro-reentrant tachycardia within the right atrium — typically counterclockwise around the tricuspid valve annulus (typical/isthmus-dependent flutter). Atrial rate is very rapid (~300 bpm); the AV node acts as a filter, conducting in a fixed ratio (2:1, 3:1, 4:1), producing the characteristic regular ventricular rate.
Clinical features: Palpitations, dyspnea, fatigue. Ventricular rate typically 150 bpm at 2:1 conduction. Similar thromboembolic risk to AF; anticoagulation required if >48 hours.
ECG hallmarks:
- Sawtooth flutter waves (F-waves) — most prominent in inferior leads (II, III, aVF) and V1
- Atrial rate ~300 bpm (250–350 bpm)
- Regular ventricular response if fixed AV conduction ratio; irregular if variable
- Most common: 2:1 block → ventricular rate ~150 bpm (must look for flutter waves within QRS/ST segments)
- Narrow QRS complexes (unless aberrant conduction)
Management: Rate control (beta-blockers, calcium channel blockers), cardioversion or antiarrhythmics for rhythm control, anticoagulation, catheter ablation (cavotricuspid isthmus ablation — highly effective, >95% cure).
9. Hyperkalemia
Pathophysiology: Elevated extracellular K⁺ reduces the resting membrane potential gradient, reducing phase 0 depolarization velocity. This slows conduction throughout the heart in a predictable sequence: first affects repolarization (T waves), then atrial conduction (P waves disappear), then ventricular conduction (QRS widens). Progressive untreated hyperkalemia leads to ventricular fibrillation and asystole. — Medical Physiology (Boron & Boulpaep)
Common causes: Acute kidney injury, Addison's disease, ACE inhibitors/ARBs/spironolactone, rhabdomyolysis, massive hemolysis.
ECG hallmarks (progressive with rising K⁺):
| K⁺ level | ECG change |
|---|---|
| 5.5–6.5 mEq/L | Peaked ("tented") T waves — narrow base, symmetric, high amplitude; best seen V2–V5 |
| 6.5–7.5 mEq/L | PR prolongation, P wave flattening/loss |
| 7.5–8.0 mEq/L | QRS widening — intraventricular conduction delay |
| >8.0 mEq/L | Sine wave pattern — QRS merges with T wave; VF/asystole imminent |
Management: Membrane stabilization (IV calcium gluconate), shift K⁺ intracellularly (insulin/dextrose, salbutamol, sodium bicarbonate), K⁺ elimination (kayexalate, patiromer, dialysis in severe cases).
10. Pulmonary Embolism (PE)
Pathophysiology: Thrombus occlusion of pulmonary vasculature raises right ventricular afterload acutely, leading to RV dilation, RV strain, and reduced LV filling. The ECG reflects acute cor pulmonale — right heart strain. Most ECG findings are non-specific; sinus tachycardia is the most common finding. Massive PE can cause hemodynamic collapse.
Clinical features: Sudden dyspnea, pleuritic chest pain, hemoptysis, hypoxia, tachycardia. High mortality if massive (>50% central pulmonary vasculature occluded).
ECG hallmarks:
- Sinus tachycardia (most common finding — ~50% of cases)
- S1Q3T3 pattern (classic but only ~20% sensitive): Deep S in lead I, Q wave in lead III, inverted T wave in lead III
- Right axis deviation
- Incomplete/complete RBBB — RV conduction delay
- T-wave inversions V1–V4 (anterior RV strain pattern)
- Right heart strain: P pulmonale, right axis, new RBBB
- Atrial arrhythmias (AF, atrial flutter) — in severe cases

Management: Anticoagulation (LMWH or unfractionated heparin → DOAC/warfarin). Massive PE: systemic thrombolysis (alteplase) or catheter-directed therapy. Submassive: risk-stratify with echocardiogram and troponin.
Quick Reference Summary Table
| Condition | Key ECG Finding | Mechanism |
|---|---|---|
| Atrial Fibrillation | Absent P waves, irregularly irregular RR | Chaotic atrial re-entry |
| STEMI | Convex ST elevation + reciprocal changes | Transmural ischemia/injury |
| Ventricular Fibrillation | Chaotic, no QRS/P/T | Disorganized ventricular depolarization |
| Complete Heart Block | P-QRS dissociation, slow escape | Total AV conduction failure |
| Ventricular Tachycardia | Wide QRS >120 ms, AV dissociation | Ventricular re-entry/automaticity |
| WPW Syndrome | Short PR, delta wave, wide QRS | Accessory pathway pre-excitation |
| Long QT Syndrome | QTc >440–460 ms, torsades de pointes | Delayed ventricular repolarization |
| Atrial Flutter | Sawtooth F-waves ~300 bpm, regular RR | Tricuspid annulus macro-reentry |
| Hyperkalemia | Peaked T → P loss → QRS widening → sine wave | K⁺ reduces membrane potential gradient |
| Pulmonary Embolism | S1Q3T3, sinus tachycardia, RV strain | Acute right ventricular pressure overload |
Sources: Guyton & Hall Textbook of Medical Physiology; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine; Braunwald's Heart Disease; Medical Physiology (Boron & Boulpaep); Morgan & Mikhail's Clinical Anesthesiology
This is a shared conversation. Sign in to Orris to start your own chat.