Give me a proper definition of anemia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have rich, authoritative content from multiple major textbooks. Here is a thorough definition:
Anemia - Definition
Anemia is defined as a significant reduction in the volume or mass of circulating red blood cells (RBCs) in the body, relative to the normal range for a given population. Because directly measuring the total red cell mass is a complex process, clinicians rely on surrogate laboratory measures - primarily hemoglobin (Hb) concentration and hematocrit (Hct) - to identify and quantify anemia.
- Goldman-Cecil Medicine: "Anemia is defined as a significant reduction in the volume of erythrocytes, or red blood cells, in the body."
- Harrison's Principles of Internal Medicine (22nd ed., 2025): "Anemia is simply defined as blood counts below normal for a given population."
- Frameworks for Internal Medicine: "Anemia is defined by a reduced absolute quantity of circulating red blood cells in the setting of normal plasma volume."
How It Is Measured
| Measure | What It Reflects |
|---|---|
| Hemoglobin concentration (g/dL) | Directly measured; preferred in clinical practice |
| Hematocrit / packed cell volume (%) | Percentage of blood occupied by RBCs; approximately 3x the Hb value |
| RBC count (per µL) | Rarely used alone to define anemia |
Because hemoglobin is directly measured (while hematocrit is a calculated value in modern analyzers), many physicians prefer Hb concentration when defining anemia. - Goldman-Cecil Medicine
Diagnostic Thresholds in Adults
Per The Washington Manual of Medical Therapeutics:
| Group | Hb (g/dL) | Hct (%) |
|---|---|---|
| Non-pregnant women | < 12 | < 36% |
| Men | < 13 | < 39% |
These thresholds vary by age, sex, race, and altitude. In children, thresholds are age-specific (defined as Hb more than 2 standard deviations below the age-specific mean). - Harriet Lane Handbook, 23rd ed.
Why It Matters Physiologically
The RBC's primary job is oxygen delivery. Hemoglobin binds O2 in the lungs and releases it to peripheral tissues. The oxygen content of arterial blood (CaO2) is described by:
CaO2 = 1.34 × [Hb] × SaO2 + (0.003 × PaO2)
A 50% drop in hemoglobin (e.g., 14 → 7 g/dL) produces a 50% reduction in CaO2, making anemia a direct threat to tissue oxygenation. By contrast, the same proportional drop in PaO2 only reduces CaO2 by ~20%. - Frameworks for Internal Medicine
Classification
Anemias are classified in two main ways:
1. By Red Cell Size (MCV):
- Microcytic (low MCV): impaired hemoglobin synthesis - iron deficiency, thalassemia, anemia of chronic disease, sideroblastic anemias
- Macrocytic (high MCV): impaired DNA synthesis (oval macrocytes: B12/folate deficiency, medications, myelodysplasia) or membrane defects (round macrocytes: alcohol, liver disease, hypothyroidism)
- Normocytic (normal MCV): renal disease, aplastic anemia, endocrinopathies, marrow infiltration
2. By Mechanism (reticulocyte count):
-
Hyperproduction/Destructive (elevated reticulocytes): blood loss or hemolysis (acquired or congenital)
-
Underproduction (low/normal reticulocytes): nutritional deficiency, bone marrow failure, chronic disease
-
Harrison's Principles of Internal Medicine, 22nd ed.
All blood cells and formation with it's lineage
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
I have comprehensive content from multiple authoritative textbooks and two excellent diagrams. I now have everything needed for a thorough answer.
Blood Cell Formation and Lineage (Hematopoiesis)
Overview
All blood cells originate from a single cell type - the hematopoietic stem cell (HSC) - residing in the bone marrow. This process is called hematopoiesis. Normal adult marrow contains an estimated 50,000 to 200,000 HSCs, which maintain blood cell production throughout life. - Robbins & Cotran Pathologic Basis of Disease
Sites of Hematopoiesis Through Life
| Stage | Primary Site |
|---|---|
| Week 3 of embryogenesis | Yolk sac (primitive red cells, tissue macrophages) |
| 3rd month of fetal life | Liver (chief site until near birth); also fetal placenta |
| 4th month onward | Bone marrow (takes over, expands progressively) |
| Birth | All marrow spaces are active (red marrow) |
| After puberty | Only axial skeleton + proximal long bones; distal bones become fatty (yellow) marrow |
- Robbins & Cotran; Henry's Clinical Diagnosis and Management by Laboratory Methods
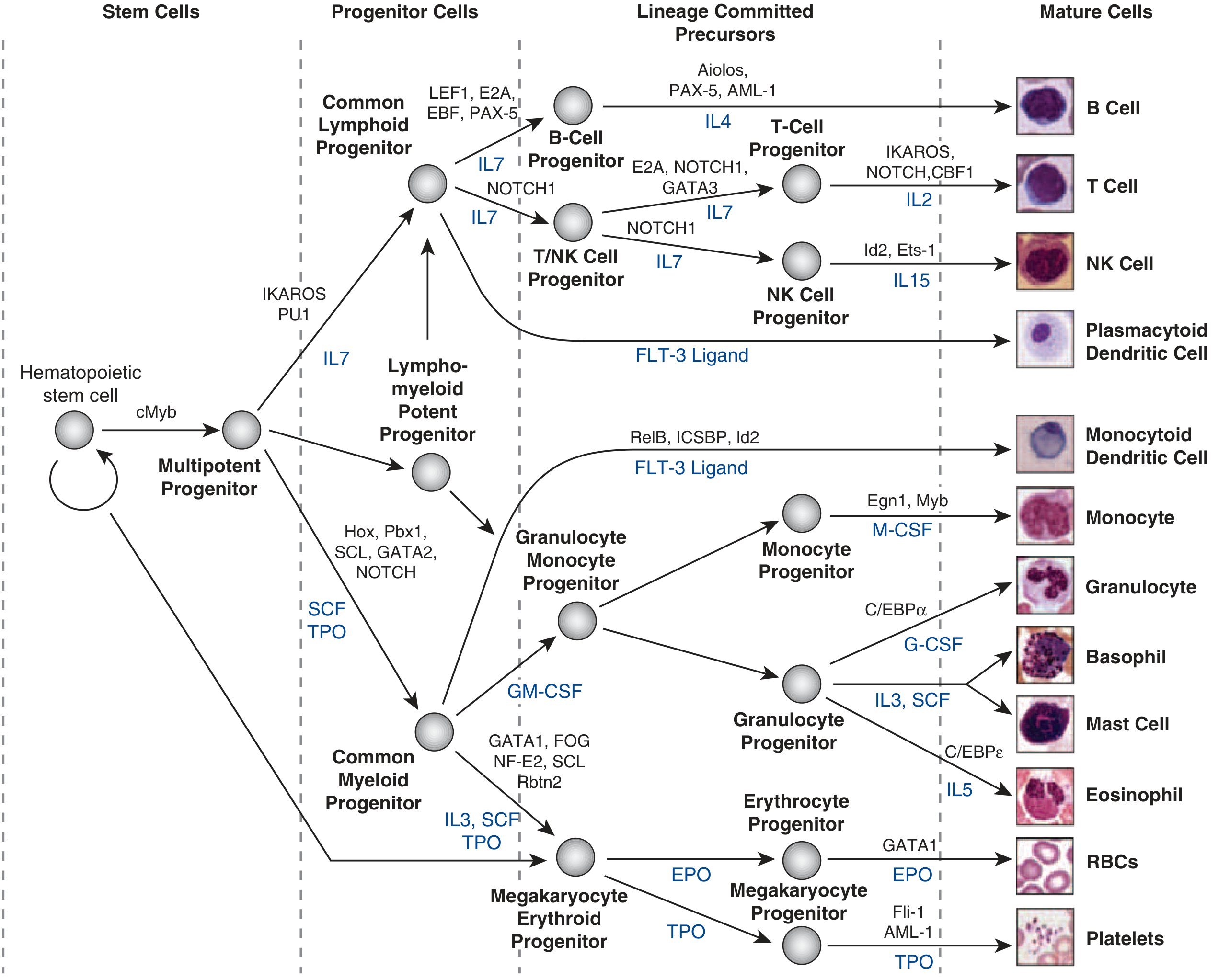
The Lineage Hierarchy - Full Diagram
Here is the complete hematopoietic differentiation map from Harrison's Principles of Internal Medicine (22nd ed., 2025):
And from Robbins & Cotran Pathologic Basis of Disease - a clearer CFU-based view:
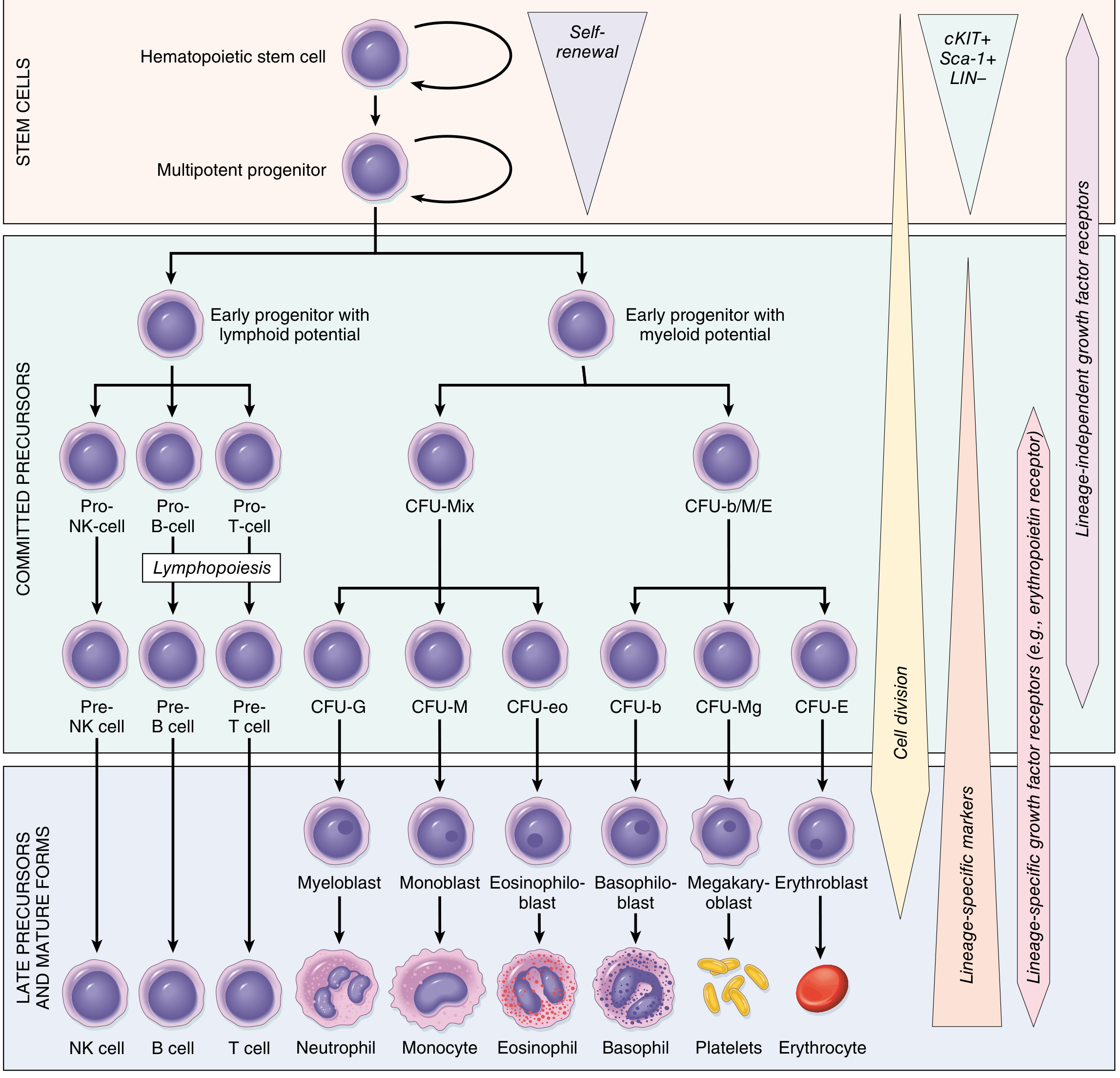
Four Levels of Maturation
| Level | Description |
|---|---|
| Stem cells | Multipotent; self-renewing; give rise to all cell types |
| Progenitor cells | More restricted; highly proliferative (transient amplifying cells); not morphologically recognizable |
| Precursor cells | Committed to one lineage; morphologically recognizable (e.g., myeloblast, pronormoblast); can still divide |
| Mature cells | Terminally differentiated effector cells; mostly cannot divide further |
- Harrison's Principles of Internal Medicine, 22nd ed.
The Two Main Arms
The HSC first splits into two broad arms:
1. Common Myeloid Progenitor (CMP)
Gives rise to all non-lymphoid blood cells via sub-progenitors.
2. Common Lymphoid Progenitor (CLP)
Gives rise to all lymphoid cells.
MYELOID LINEAGE
A. Erythrocyte (Red Blood Cell) Lineage
Pathway:
HSC → CMP → Megakaryocyte-Erythroid Progenitor (MEP) → BFU-E (burst-forming unit) → CFU-E → Pronormoblast → Basophilic normoblast → Polychromatophilic normoblast → Orthochromatic normoblast → Reticulocyte → Mature RBC
Key regulator: Erythropoietin (EPO), produced by the kidney in response to hypoxia.
Transcription factors: GATA1, SCL
Normoblastic maturation stages (Henry's Clinical Diagnosis):
| Stage | Size | Key Features |
|---|---|---|
| Pronormoblast | ~20 µm (largest) | Fine chromatin, prominent nucleolus, basophilic cytoplasm, no granules |
| Basophilic normoblast | Smaller | Coarser clumped chromatin, deeply basophilic cytoplasm (rich in RNA/ribosomes) |
| Polychromatophilic normoblast | Smaller | Cytoplasm turns gray-blue as hemoglobin accumulates; nucleus occupies ~50% |
| Orthochromatic normoblast | Smaller | Pyknotic (dense, small) nucleus; cytoplasm near-pink; no more mitosis |
| Reticulocyte | Slightly larger than RBC | Nucleus extruded; residual RNA/mitochondria remain; stays 1-2 days in marrow, 1 day in blood |
| Mature RBC (Erythrocyte) | ~7-8 µm | Anucleate biconcave disc; lives ~120 days |
One pronormoblast generates up to 16 reticulocytes through 3-4 mitotic divisions over 3 days. Developing erythroid cells cluster around macrophages in erythroblastic islands where iron is transferred for hemoglobin synthesis.
B. Granulocyte Lineage (Neutrophil, Eosinophil, Basophil)
Pathway:
HSC → CMP → Granulocyte-Monocyte Progenitor (GMP) → Granulocyte Progenitor → Myeloblast → Promyelocyte → Myelocyte → Metamyelocyte → Band form → Mature Granulocyte
Sub-lineages from the Granulocyte Progenitor:
- CFU-G → Neutrophil (regulated by G-CSF; transcription factor C/EBPα)
- CFU-eo → Eosinophil (regulated by IL-5; transcription factor C/EBPε)
- CFU-b → Basophil / Mast cell (regulated by IL-3, SCF)
Neutrophil is the most abundant granulocyte. Mature granulocytes cannot proliferate - numbers can only increase via production from precursors.
C. Monocyte / Macrophage Lineage
Pathway:
HSC → CMP → GMP → Monocyte Progenitor → Monoblast → Promonocyte → Monocyte (blood) → Macrophage (tissue)
Regulator: M-CSF (macrophage colony-stimulating factor)
Transcription factors: Egn1, Myb
Monocytes circulate briefly in blood (~1-3 days) then enter tissues and differentiate into tissue macrophages (e.g., Kupffer cells in liver, microglial cells in brain, alveolar macrophages in lung, osteoclasts in bone).
Dendritic cells (both monocytoid and plasmacytoid types) also arise from this progenitor pool, regulated by FLT-3 Ligand.
D. Megakaryocyte / Platelet Lineage
Pathway:
HSC → CMP → MEP → Megakaryoblast → Promegakaryocyte → Megakaryocyte → shedding of cytoplasm into Platelets
Regulator: Thrombopoietin (TPO)
Transcription factors: Fli-1, AML-1
Megakaryocytes are giant cells in the marrow that undergo endomitosis (DNA replication without cell division), becoming polyploid. They then extend long cytoplasmic processes called proplatelets through the marrow sinusoidal wall, from which platelets are pinched off into the bloodstream. Each megakaryocyte produces ~1,000-3,000 platelets. Platelets live ~7-10 days and are anucleate.
LYMPHOID LINEAGE
Pathway:
HSC → Common Lymphoid Progenitor (CLP) → three sub-lineages:
| Lineage | Progenitor | Mature Cell | Key Regulator | Transcription Factor |
|---|---|---|---|---|
| B cells | Pro-B → Pre-B | B lymphocyte → Plasma cell | IL-7, IL-4 | LEF1, E2A, EBF, PAX-5 |
| T cells | Pro-T → Pre-T (matures in thymus) | T lymphocyte (CD4+ helper, CD8+ cytotoxic) | IL-7, IL-2 | NOTCH1, IKAROS, GATA3 |
| NK cells | T/NK progenitor → NK progenitor | Natural killer cell | IL-7, IL-15 | Id2, Ets-1 |
| Plasmacytoid Dendritic cells | Direct from CLP | pDC | FLT-3 Ligand | - |
B cells mature entirely in the bone marrow. T cells complete their maturation in the thymus (positive and negative selection). NK cells are innate lymphoid cells that do not require antigen-specific activation.
- Harrison's Principles of Internal Medicine, 22nd ed.
Key Cytokines and Growth Factors Summary
| Factor | Primary Target |
|---|---|
| EPO (erythropoietin) | Erythrocyte production |
| TPO (thrombopoietin) | Megakaryocyte / platelet production |
| G-CSF | Neutrophil production and mobilization |
| M-CSF | Monocyte / macrophage production |
| GM-CSF | Granulocyte + monocyte progenitors |
| IL-3 | Multi-lineage progenitor support |
| IL-4 | B-cell differentiation |
| IL-5 | Eosinophil production |
| IL-7 | Lymphoid progenitors (B and T cells) |
| IL-15 | NK cell development |
| SCF (stem cell factor) | HSC and early progenitors |
| FLT-3 Ligand | Dendritic cells, early progenitors |
Summary Tree (Text Form)
Hematopoietic Stem Cell (HSC)
├── Common Myeloid Progenitor (CMP)
│ ├── Granulocyte-Monocyte Progenitor (GMP)
│ │ ├── CFU-G → Neutrophil
│ │ ├── CFU-eo → Eosinophil
│ │ ├── CFU-b → Basophil / Mast cell
│ │ └── Monocyte Progenitor → Monocyte → Macrophage / Dendritic cell
│ └── Megakaryocyte-Erythroid Progenitor (MEP)
│ ├── CFU-E → Pronormoblast → ... → Erythrocyte (RBC)
│ └── CFU-Mg → Megakaryoblast → Megakaryocyte → Platelets
└── Common Lymphoid Progenitor (CLP)
├── Pro-B → Pre-B → B cell → Plasma cell
├── Pro-T → Pre-T → T cell (CD4+/CD8+) [matures in thymus]
├── T/NK Progenitor → NK cell
└── Plasmacytoid Dendritic cell
Sources: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar Pathologic Basis of Disease; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.