Tell me about Kawasaki disease
Reading File
Finding Sources
Searching PubMed
"Kawasaki disease"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching PubMed
"Kawasaki disease" AND "coronary artery" AND treatment
Reading File
Reading Article
PMID: 39534969
Reading File
Loading Image
Loading Image
Reading File
I have very comprehensive information. Let me now compile the full answer.
Kawasaki Disease
Kawasaki disease (KD), also known as mucocutaneous lymph node syndrome, is the leading cause of acquired heart disease in children in developed nations. It is an acute, self-limited, systemic vasculitis of unknown etiology that primarily affects medium-sized muscular arteries - most dangerously the coronary arteries. About 25% of untreated children develop coronary artery aneurysms, which can lead to myocardial infarction and sudden death.
Epidemiology
-
Predominantly affects children under 5 years, with peak incidence at 6-24 months
-
More common in boys than girls
-
Highest incidence in Asian children - approximately 1 in 80 Japanese children develops KD by age 5 (incidence: 20-100 per 100,000 children under 5 in Asia)
-
Occurs in all racial groups; found worldwide
-
Seasonal variation: peaks in winter and spring
-
No confirmed infectious agent has been identified, though epidemiologic patterns (seasonality, community outbreaks) strongly support an infectious trigger
-
Fitzpatrick's Dermatology, Ch. 142
-
Rosen's Emergency Medicine, p. 2417
Pathogenesis
The etiology remains unknown. The best-supported hypothesis is that KD results from infection with a ubiquitous agent that causes asymptomatic disease in most but triggers KD in a genetically predisposed minority. Genetic polymorphisms in the ITPKC gene (a negative regulator of T-cell activation), as well as CASP3, BLK, CD40, FCGR2A, and ORAI1, are associated with susceptibility.
Three linked pathologic processes drive KD vasculopathy:
- Neutrophil necrotizing arteritis - occurs in the first 2 weeks; damages vessel wall structural integrity
- Subacute/chronic vasculitis - begins in the first 2 weeks, can persist months to years; comprised of CD8 T lymphocytes, IgA plasma cells, eosinophils, and macrophages
- Luminal myofibroblastic proliferation - closely linked to chronic vasculitis; leads to progressive arterial stenosis months to years later
These three processes explain the risk of aneurysm formation (from neutrophilic destruction), thrombosis, and late stenosis.
- Fitzpatrick's Dermatology, Ch. 142
Clinical Features
The illness unfolds in three phases:
Phase I: Acute Febrile Phase (~12 days)
- Prolonged high fever (often >39-40°C) lasting >5 days - the cardinal feature
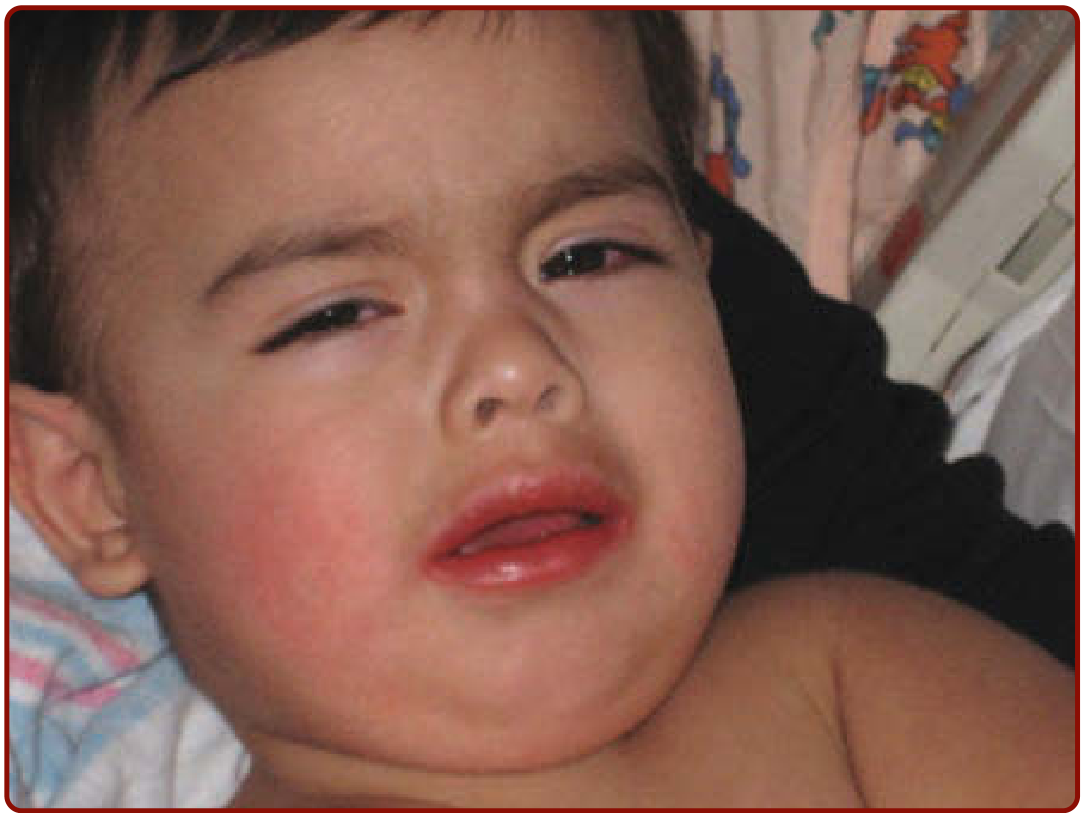
- Bilateral non-exudative conjunctival injection with limbal sparing (~90% of cases)
- Oral mucosal changes: red, dry, cracked, bleeding lips; "strawberry" tongue; diffuse oropharyngeal erythema (no ulcers)
- Polymorphous rash - begins on palms/soles, spreads to extremities and trunk within 2 days
- Erythema and painful edema of the hands and feet
- Cervical lymphadenopathy - at least one node >1.5 cm; usually unilateral and nonfluctuant (least common feature, ~75%)
- Arthritis of small interphalangeal joints can occur
- Myocarditis present in >50% of patients during this phase, manifested as tachycardia disproportionate to fever
Phase II: Subacute Phase (up to ~30 days)
- Fever resolves
- Periungual desquamation beginning at fingertips/toes, progressing to the entire soles and palms
- Thrombocytosis (platelet count often >450,000/mm³ after day 7)
- Arthritis, arthralgias
- High risk of sudden death if untreated (coronary aneurysm most vulnerable)
Phase III: Convalescent Phase (~6-8 weeks)
- Most signs resolve
- ESR normalizes
- Coronary aneurysms, if present, are diagnosed here (echocardiography or coronary angiography)

Diagnostic Criteria (CDC/AHA)
Classic KD = Fever ≥5 days plus at least 4 of the following 5 features:
| Feature | Detail |
|---|---|
| 1. Polymorphous rash | Non-vesicular, non-bullous |
| 2. Bilateral conjunctival injection | Non-exudative |
| 3. Oral mucosal changes | Strawberry tongue, red/cracked lips, pharyngeal erythema |
| 4. Cervical lymphadenopathy | At least one node >1.5 cm, typically unilateral |
| 5. Extremity changes | Erythema/edema of palms/soles; periungual desquamation (subacute phase) |
Other illnesses with similar presentations must be excluded.
Incomplete KD is recognized when a child has prolonged fever with fewer than 4 features but later develops coronary artery abnormalities. This is a major diagnostic challenge. Infants ≤6 months are especially vulnerable - they often have subtle findings but high risk of coronary involvement, and should be evaluated even without full criteria.
- Textbook of Family Medicine, 9e, p. 915
Laboratory Findings
Labs are supportive, not diagnostic:
- Leukocytosis (WBC ≥15,000/mm³ with neutrophil predominance)
- Elevated ESR and CRP (ESR >40 mm/h; elevated CRP) - elevated in acute/subacute phases
- Thrombocytosis (platelets ≥450,000/mm³ after day 7 of illness)
- Elevated ALT (liver involvement)
- Hypoalbuminemia (albumin ≤3.0 g/dL)
- Normocytic anemia
- Sterile pyuria (≥10 WBC/HPF on urinalysis)
- ECG: PR and QT prolongation, ST/T wave changes
- Aseptic meningitis may be found on lumbar puncture
Complications
Cardiovascular (the most feared):
- Coronary artery dilation and aneurysms in ~25% of untreated cases
- Myocardial infarction - from aneurysm thrombosis (most common in first few months) or from coronary stenosis (months to years later)
- Aneurysm rupture - less common, usually within the first month
- Pericardial effusion - present in the acute phase, usually resolves spontaneously
- Aneurysms of other medium-sized arteries (iliac, femoral, axillary) in severe cases
- Valvulitis (rare)
Long-term consequences are confined to the heart and vascular tree. There are no known long-term non-cardiovascular sequelae.
- Fitzpatrick's Dermatology, Ch. 142
Management
Hospitalization is required.
Acute Treatment (within first 10 days of fever):
- IVIG 2 g/kg as a single infusion - the cornerstone of treatment. IVIG given within the first 10 days reduces coronary artery aneurysm prevalence from 25% down to ~5% (a fivefold reduction)
- High-dose aspirin (80-100 mg/kg/day in 4 divided doses) during the acute febrile phase - anti-inflammatory
- After fever resolves, aspirin is reduced to low-dose (3-5 mg/kg/day) for antiplatelet effect, continued until echocardiography confirms no coronary abnormalities (typically 6-8 weeks)
What NOT to use:
- Antibiotics - not useful unless a concomitant bacterial infection is present
- Corticosteroids - may actually increase the incidence of aneurysms and should be avoided if possible in routine cases (though used as adjunct therapy for IVIG-resistant cases per recent data)
Monitoring:
-
Serial echocardiograms - at diagnosis, 2-3 weeks into illness, and 1 month later
-
Early cardiology evaluation is essential
-
Textbook of Family Medicine, 9e; Rosen's Emergency Medicine; Fitzpatrick's Dermatology, Ch. 142
Differential Diagnosis
Conditions that mimic KD include:
- Scarlet fever (streptococcal)
- Viral exanthems (measles, adenovirus, EBV)
- Stevens-Johnson syndrome / toxic epidermal necrolysis
- Juvenile idiopathic arthritis (systemic form)
- Toxic shock syndrome
- Drug hypersensitivity reactions
- Staphylococcal scalded skin syndrome
2024 AHA Update
A 2024 American Heart Association Scientific Statement on KD (Jone et al., Circulation, 2024) highlights several advances:
- New criteria defining North American patients at high risk for coronary artery aneurysms who may benefit from more intensive initial treatment
- Advances in cardiovascular imaging (CT angiography, MRI) improving detection of coronary stenosis
- Updated safety and dosing data for several anti-inflammatory adjunct therapies
- New anticoagulation strategies and MI management protocols for patients with established aneurysms
Key Summary Points
| Feature | Details |
|---|---|
| Disease type | Self-limited systemic vasculitis of medium arteries |
| Peak age | 6-24 months; rare after age 14 |
| Leading concern | Coronary artery aneurysms (25% untreated) |
| Key diagnosis sign | Fever ≥5 days + ≥4 of 5 mucocutaneous criteria |
| Treatment | IVIG 2 g/kg + aspirin within first 10 days |
| IVIG effect | Reduces aneurysm rate from 25% → 5% |
| Etiology | Unknown; suspected infectious trigger in genetically predisposed hosts |
This is a shared conversation. Sign in to Orris to start your own chat.