Carbonic anhydride inhibitors in ophthalmology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"carbonic anhydrase inhibitors"[MeSH Terms] AND glaucoma[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full, detailed response.
Carbonic Anhydrase Inhibitors (CAIs) in Ophthalmology
Mechanism of Action
Carbonic anhydrase (CA) catalyzes the reversible reaction: CO₂ + H₂O ⇌ H₂CO₃ ⇌ H⁺ + HCO₃⁻. In the ciliary body epithelium, CA (primarily isoform II) drives HCO₃⁻ secretion from blood into the posterior chamber, which osmotically draws water and lowers IOP. CAIs inhibit this process, reducing aqueous humor formation and thereby lowering IOP. This is the most common therapeutic indication for CAIs.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Drug Classes and Agents
Topical CAIs (Preferred Route)
Developed specifically because oral CAIs carry a poor systemic side effect profile. Both inhibit CA isoform II in the ciliary body epithelium without producing renal or systemic effects at standard doses.
| Drug | Formulation | Dosing | Notes |
|---|---|---|---|
| Dorzolamide | 2% solution | TID monotherapy; BID adjunctive | Burning, stinging, transient metallic/bitter taste; allergic blepharoconjunctivitis (uncommon) |
| Brinzolamide | 1% suspension | TID monotherapy; BID adjunctive | Less stinging and local allergy than dorzolamide; white residue on lids possible |
Both are slightly less effective than topical beta-blockers for IOP reduction, but may provide a supplementary neuroprotective effect - a notable advantage in glaucoma management.
- Kanski's Clinical Ophthalmology, 10th Ed.
- Goodman & Gilman's, Table 24-9
Systemic CAIs
Generally reserved for short-term use (especially acute glaucoma), or long-term only in patients at high risk of visual loss who cannot tolerate or do not respond to topical therapy.
| Drug | Formulation | Typical Dose | Notes |
|---|---|---|---|
| Acetazolamide | Tablets 125/250 mg; SR 500 mg; IV 500 mg | 250-1000 mg/day in divided doses; IV single dose for acute angle-closure | Most widely used systemic CAI |
| Methazolamide | Tablets 50 mg | 50-100 mg 2-3x daily | Longer duration than acetazolamide; generally fewer GI/paresthesia side effects; less available |
| Dichlorphenamide | Tablets 50 mg | 50-100 mg 2-3x daily | FDA-approved for familial periodic paralysis |
- Kanski's Clinical Ophthalmology, 10th Ed.
- Katzung's, Table 10-3
Ophthalmic Indications
- Primary open-angle glaucoma (POAG) - the most common indication; topical CAIs used as first-line (when prostaglandins/beta-blockers are contraindicated) or adjunctive second/third-line therapy
- Secondary glaucoma - including neovascular, uveitic, steroid-induced
- Acute angle-closure glaucoma - IV or oral acetazolamide is used preoperatively/emergently to rapidly lower IOP before laser or surgery
- Ocular hypertension - to prevent progression to glaucoma
- Congenital/infantile glaucoma - topical CAIs (dorzolamide, brinzolamide BID) are used alongside beta-blockers
- Idiopathic intracranial hypertension (pseudotumor cerebri) - acetazolamide reduces CSF pressure via the same mechanism in the choroid plexus
- Cystoid macular edema (CME) - topical CAIs (particularly dorzolamide) have been used off-label in retinitis pigmentosa-associated CME
- Wills Eye Manual; Goodman & Gilman's; Lippincott Illustrated Reviews: Pharmacology
Combination Preparations
Combined topical formulations improve convenience and adherence with additive IOP-lowering effects:
-
Cosopt - timolol 0.5% + dorzolamide 2% (twice daily)
-
Azarga - timolol 1% + brinzolamide 1% (twice daily)
-
Simbrinza - brimonidine 0.2% + brinzolamide 1% (twice daily) - the only beta-blocker-free combination; useful in patients with beta-blocker contraindications
-
Kanski's Clinical Ophthalmology, 10th Ed.
Adverse Effects
Topical CAIs
- Local: burning/stinging on instillation (dorzolamide > brinzolamide), transient bitter/metallic taste, white eyelid residue (brinzolamide)
- Allergic blepharoconjunctivitis (uncommon)
- Corneal decompensation in patients with pre-existing corneal endothelial dysfunction - an important ophthalmic-specific concern
- Idiosyncratic bone marrow suppression (rare)
Systemic CAIs
-
Very common: Paresthesias ("pins and needles" in extremities), malaise, lowered mood, fatigue, GI symptoms (nausea, anorexia)
-
Metabolic: Hypokalemia, hyperchloremic metabolic acidosis
-
Renal: Nephrolithiasis (calcium phosphate stones in alkaline urine); rarely, acute kidney injury
-
Ocular (specific): Choroidal effusion (especially post-cataract surgery), which can cause angle closure
-
Rare/serious: Stevens-Johnson syndrome; dose-related bone marrow suppression; idiosyncratic aplastic anemia (~50% mortality)
-
Hepatic: Contraindicated in cirrhosis - decreased NH₄⁺ excretion raises risk of hepatic encephalopathy
-
Respiratory: Contraindicated in severe COPD (worsens respiratory acidosis)
-
Kanski's Clinical Ophthalmology; Goodman & Gilman's; Lippincott Pharmacology
Contraindications and Cautions
- Sulfonamide allergy - CAIs are sulfonamide derivatives; relative contraindication for topical and systemic forms (cross-reactivity uncommon but possible)
- Corneal endothelial dysfunction - topical CAIs risk precipitating corneal decompensation
- Hepatic cirrhosis
- Severe COPD / hyperchloremic acidosis
- Concomitant topical + systemic CAI - generally does NOT produce additive IOP-lowering effect
- High-dose salicylates - drug interaction; reduced urinary excretion of weak organic bases
- Caution with young children: systemic absorption from topical beta-blocker combinations can cause severe systemic effects
Place in Therapy
CAIs are second- or third-line topical agents for POAG when prostaglandin analogues (first-line) or beta-blockers are insufficient or contraindicated. Systemic acetazolamide remains an important bridge therapy in acute angle-closure glaucoma, used IV to rapidly break an acute attack before definitive laser iridotomy.
A 2025 systematic review and network meta-analysis in Ophthalmology (PMID: 40701331) analyzed glaucoma medication efficacy and drug interactions - the most recent high-level evidence update for this drug class.
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed.
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
- Lippincott Illustrated Reviews: Pharmacology
- The Wills Eye Manual
- Morgan and Mikhail's Clinical Anesthesiology, 7th Ed.
Factors affecting retinal adherance
Reading File
Finding Sources
Finding Sources
Searching PubMed
"retinal adhesion" AND "subretinal space" AND mechanisms
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
I now have all the material needed for a comprehensive, well-illustrated answer. Let me compile it.
Factors Affecting Retinal Adherence
The neurosensory retina (neural retina) and the retinal pigment epithelium (RPE) are not anatomically fused - they are apposed across a potential space that is a vestige of the embryonic optic cup lumen. Retinal adherence is therefore maintained by a combination of active and passive forces. Failure of any of these can allow subretinal fluid to accumulate and produce retinal detachment.
Histology: A Text and Atlas explains this well: "A potential space exists between the two layers of the retina... Separation of the layers, retinal detachment, also occurs in the living state because of eye disease or trauma."
1. Structural Anatomy - The Foundation
The RPE sits on Bruch's membrane, which anchors it firmly to the choriocapillaris of the choroid. The RPE is firmly attached at this outer boundary. The neural retina above it, however, has no equivalent firm anatomical bond to the RPE - adherence depends on the factors below.
Two anatomical zones have particularly strong adhesion:
-
Ora serrata - fusion of the sensory retina with the RPE and choroid at the peripheral boundary limits forward extension of subretinal fluid during detachment
-
Vitreous base - a 3-4 mm zone straddling the ora serrata where the cortical vitreous is strongly attached to the retinal internal limiting membrane
-
Kanski's Clinical Ophthalmology, 10th Ed.
2. Active RPE Fluid Pump (Most Important Factor)
The RPE actively transports fluid from the subretinal space toward the choroid, maintaining a slight negative pressure (subatmospheric) in the potential subretinal space. This is the dominant force keeping the retina apposed to the RPE. The pump relies on:
- Na⁺/K⁺-ATPase activity on the basolateral RPE membrane
- Ion channels and aquaporins
- Metabolic integrity of the RPE cells (oxygen, glucose supply from choriocapillaris)
Any disease that damages RPE cells - such as malignant hypertension (focal choroidal infarcts damaging RPE), inflammation, or choroidal tumors - impairs this pump and permits fluid to leak from the choroidal circulation into the subretinal space.
- Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology
3. Choroidal Oncotic and Hydrostatic Pressure
The choriocapillaris is highly permeable. The colloid oncotic pressure of the choroid (due to plasma proteins that cannot cross) creates a net osmotic gradient drawing fluid outward through the RPE from the subretinal space toward the choroid. This supplements the RPE pump. Conversely, elevated choroidal hydrostatic pressure (as in malignant hypertension) can overwhelm this gradient and push fluid in the opposite direction - under the retina.
4. Photoreceptor Outer Segment - RPE Interdigitation
The apical microvilli of the RPE interdigitate with the outer segments of the photoreceptor cells (rods and cones). This mechanical coupling provides physical contact adhesion and also serves a metabolic function - the RPE phagocytoses shed outer segment discs and supplies nutrients (particularly for the outer retina, which has no direct blood supply and depends entirely on diffusion from the choriocapillaris).
As Guyton & Hall notes: "The outermost layer of the retina is adherent to the choroid... The outer layers of the retina, especially the outer segments of the rods and cones, depend mainly on diffusion from the choroid blood vessels for their nutrition."
- Guyton & Hall Textbook of Medical Physiology
5. Vitreous Support
The vitreous body (composed primarily of water and type II collagen) fills the posterior segment and normally rests against the inner surface of the retina, providing gentle forward support. However, the vitreous plays a dual role:
-
Normal state: supports retinal apposition; Goldman-Cecil describes it as functioning "to maintain neural retinal attachment"
-
Pathological state: as the vitreous ages and liquefies (syneresis), it can shrink and exert traction on points of strong adhesion to the retinal internal limiting membrane. If the posterior hyaloid does not separate cleanly (incomplete posterior vitreous detachment, PVD), it pulls and tears the retina - the mechanism of rhegmatogenous retinal detachment
-
Goldman-Cecil Medicine; Guyton & Hall
6. Integrity of the Blood-Retinal Barrier
Goldman-Cecil describes the blood-retinal barrier as composed of:
- Tight junctions between neighboring RPE cells (outer barrier)
- Tight junctions between retinal vascular endothelial cells (inner barrier)
Disruption of these barriers (by inflammation, ischemia, neovascularization, or trauma) allows protein-rich fluid to leak into the subretinal space, creating an exudative (non-rhegmatogenous) detachment.
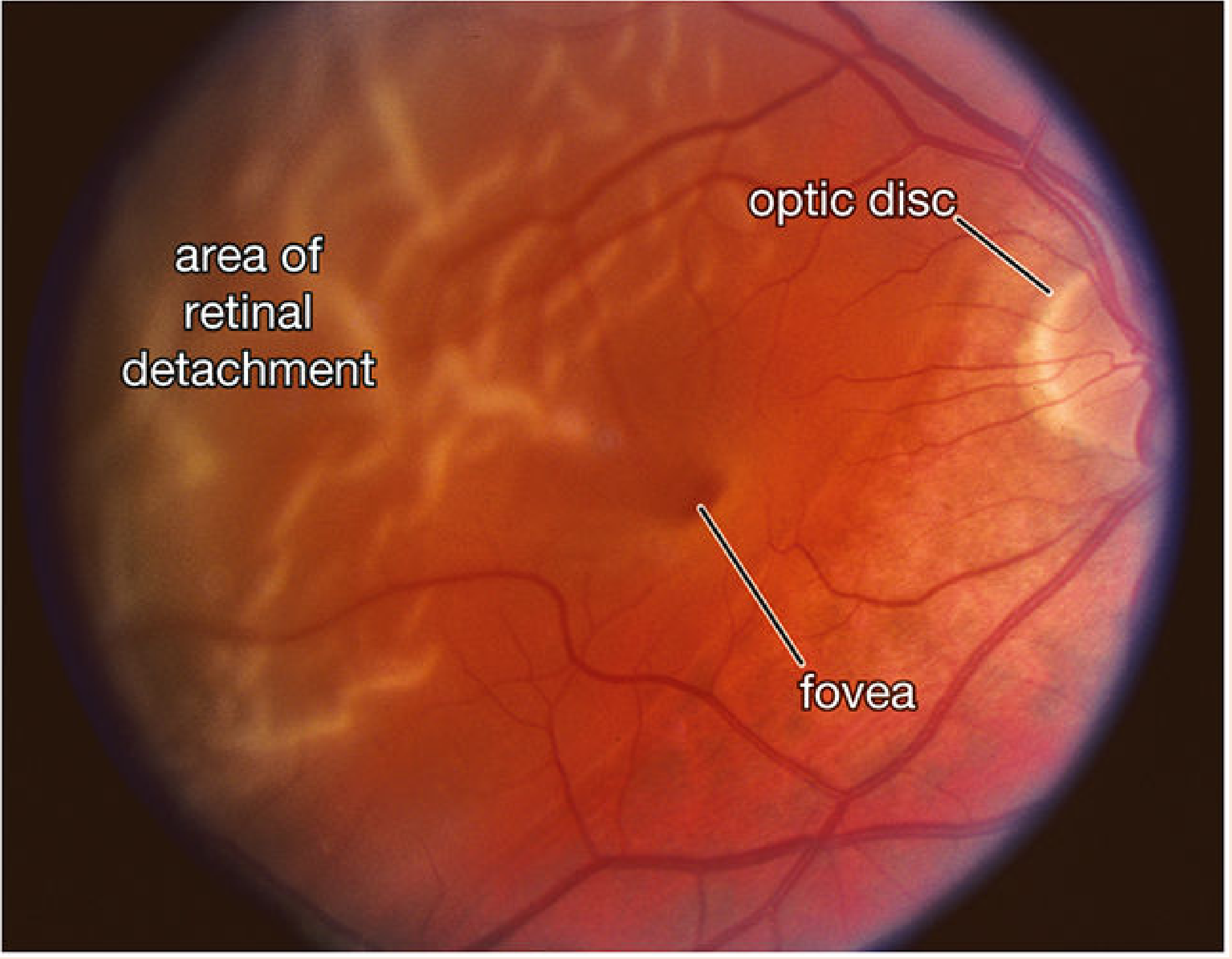
Pathological Consequences - Types of Retinal Detachment
When the above factors are overcome, three classic mechanisms lead to retinal detachment:
| Type | Mechanism | Cause of failure |
|---|---|---|
| Rhegmatogenous | Full-thickness retinal break - liquefied vitreous seeps through | Vitreous traction/tear; most common |
| Exudative (non-rhegmatogenous) | Subretinal fluid from damaged RPE/choroidal vasculature | Malignant hypertension, choroidal tumors, inflammation |
| Tractional | Fibrovascular membranes pull retina away from RPE | Proliferative diabetic retinopathy, PVR |
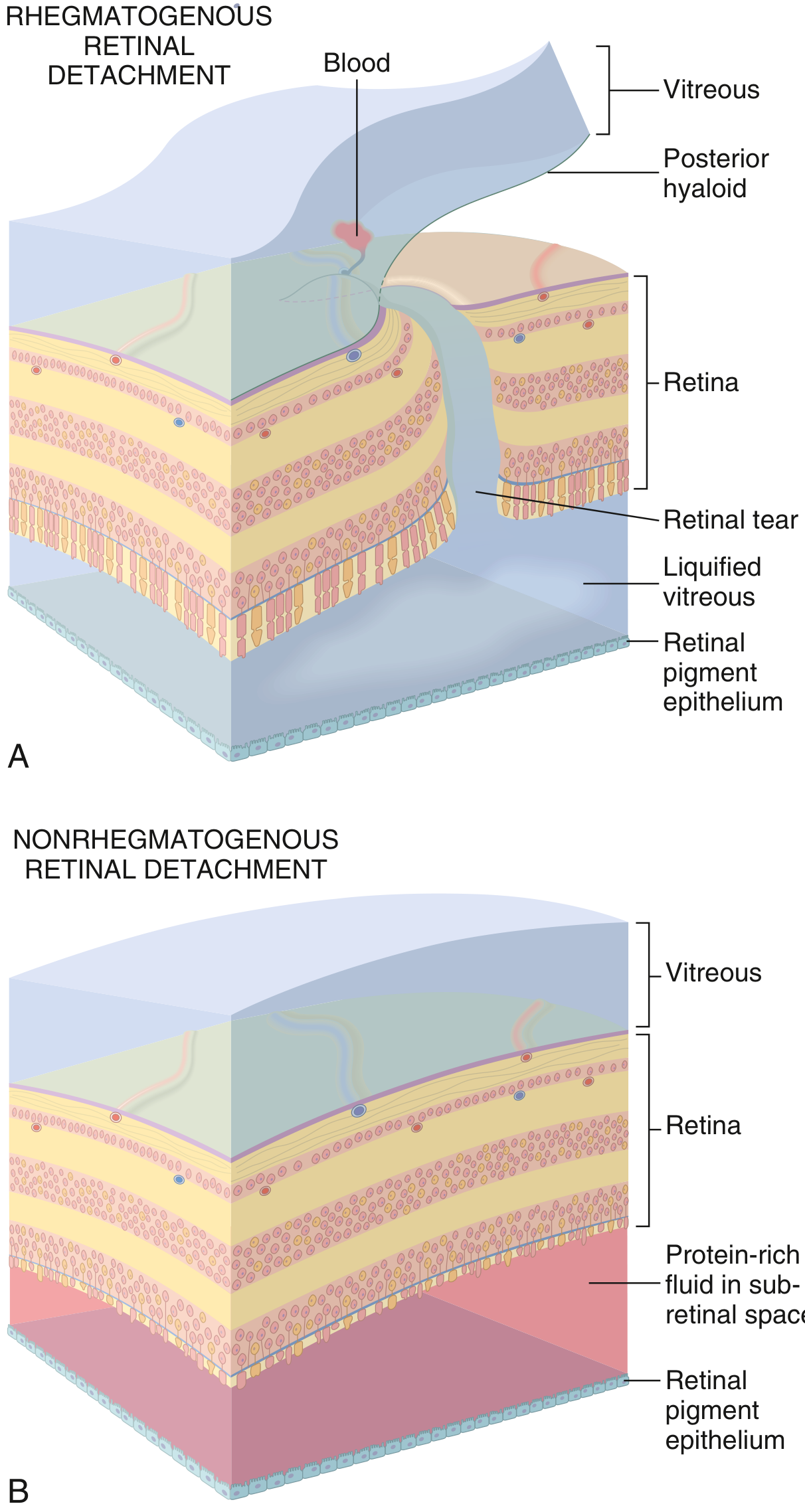
From Robbins & Kumar Basic Pathology
From Histology: A Text and Atlas
Summary of Factors
| Factor | Role in Adherence | Failure Leads To |
|---|---|---|
| RPE active fluid pump | Primary force - removes subretinal fluid | Exudative detachment |
| Choroidal oncotic pressure | Passive osmotic draw | Exudative detachment |
| Photoreceptor-RPE interdigitation | Mechanical contact adhesion | Separation on injury/disease |
| Vitreous support | Posterior pressure keeps retina apposed | Tractional / rhegmatogenous if pathological |
| Blood-retinal barrier integrity | Prevents fluid accumulation | Exudative detachment |
| Structural fusion at ora serrata | Limits anterior spread of SRF | Detachment stays posterior |
| Vitreous base adhesion | Strong peripheral anchorage | Avulsion in trauma |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed.
- Robbins & Kumar Basic Pathology
- Goldman-Cecil Medicine, International Ed.
- Guyton & Hall Textbook of Medical Physiology
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology
This is a shared conversation. Sign in to Orris to start your own chat.