Mastoidectomy surgery Along with Mastoid anatomy from basic to clinical
Reading File
Finding Sources
Finding Sources
Searching the Web
mastoidectomy surgery steps anatomy mastoid bone clinical 2024
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive material from Cummings Otolaryngology and Scott-Brown's. I have enough to write a thorough, well-structured answer. Let me compile this now.
Mastoid Anatomy and Mastoidectomy Surgery
Basic to Clinical - A Comprehensive Guide
PART 1: MASTOID ANATOMY - FROM BASIC TO CLINICAL
1.1 Mastoid Bone - Overview
The mastoid process is the posterior part of the temporal bone, projecting downward behind the ear. It is a pneumatized (air-filled, honeycomb-like) structure whose cells communicate with the middle ear via the aditus ad antrum.
The temporal bone has five parts:
- Squamous - forms the lateral skull wall
- Petrous - contains inner ear structures
- Mastoid - houses air cells
- Tympanic - forms the bony ear canal
- Styloid - attachment for ligaments/muscles
1.2 Pneumatization of the Mastoid
The mastoid is the largest pneumatized region of the temporal bone. It is located lateral to the labyrinth and communicates directly with the attic (epitympanum) via its medial compartment, the antrum.
"The mastoid also extends posteriorly into the occipital bone and communicates with medial cell tracts. Although the vestibular portion of the inner ear forms the medial wall of the antrum, the Koerner septum - the embryologic junction between petrosal and squamosal portions of the temporal bone - forms the lateral limit."
- Cummings Otolaryngology Head and Neck Surgery
Primary Regions of Temporal Bone Pneumatization:
| Primary Region | Component Cell Tracts |
|---|---|
| Mastoid | Antrum, central mastoid tract, tegmental, sinodural, sinal, facial, and tip cells |
| Perilabyrinthine | Supralabyrinthine and infralabyrinthine |
| Petrous apex | Peritubal and apical areas |
| Accessory regions | Zygomatic, squamous, occipital, and styloid |
Three phases of pneumatization occur during development, reaching adult size at puberty. Extent of pneumatization depends on:
- Early otologic history
- Middle ear ventilation
- History of otitis media
- Heredity
Poor pneumatization is clinically significant - it is a marker of reduced capacity to ventilate the middle ear and mastoid, associated with a greater likelihood of chronic ear disease, otomastoiditis, and cholesteatoma.
1.3 Key Surgical Landmarks of the Mastoid
These are the essential landmarks every surgeon must identify:
| Landmark | Significance |
|---|---|
| Spine of Henle (MacEwen's spine) | Posterior-superior edge of the EAC; marks the level of the antrum |
| Temporal line (linea temporalis) | Marks the floor of the middle cranial fossa (tegmen) |
| Posterior bony ear canal | Defines the anterior border of the mastoid cavity |
| Sigmoid sinus | Posterior/deep border; dural venous sinus |
| Tegmen tympani | Roof of tympanic cavity; floor of middle cranial fossa dura |
| Mastoid antrum | Gateway between mastoid and middle ear |
| Sinodural angle (Citelli's angle) | Angle between sigmoid sinus and dural plate |
| Lateral semicircular canal (LSC) | Deep landmark; dome visible at the antrum; must not be violated |
| Koerner's septum | Embryologic junction; can falsely give impression of antrum being reached |
| Facial nerve (CN VII) | Mastoid segment runs vertically from 2nd genu to stylomastoid foramen |
1.4 The Facial Nerve in the Mastoid - Critical Anatomy
The facial nerve is the most feared structure in mastoid surgery. Its mastoid (vertical) segment runs from the second genu (posterior genu, behind the oval window) downward to the stylomastoid foramen.
Vulnerabilities:
| Segment | Vulnerability | Mechanism |
|---|---|---|
| Labyrinthine | Narrow canal; no epineurium; watershed vascularity | Viral infection/fracture at geniculate fossa |
| Geniculate ganglion | Dehiscent geniculate fossa; adjacent to supratubal recess | Cholesteatoma erosion; surgical trauma |
| Tympanic segment / 2nd genu | Most common site of congenital dehiscence (especially above oval window) | Suppurative OtM; iatrogenic |
| Mastoid segment | Displaced nerve; underdeveloped mastoid tip in infants | Iatrogenic during mastoidectomy; postauricular incision in neonate |
"The tympanic segment is the most common site of congenital dehiscence of the bony canal, especially above the oval window... Bony dehiscence by cholesteatoma is also common proximal to the second genu."
- Cummings Otolaryngology
In neonates: the mastoid tip is underdeveloped, placing the stylomastoid foramen and facial nerve more superficial, making it susceptible to injury from postauricular incisions and forceps delivery.
1.5 Trautmann's Triangle
An important anatomical triangle bounded by:
- Anteriorly: The posterior semicircular canal
- Posteriorly: The sigmoid sinus
- Superiorly: The superior petrosal sinus/dura
This is the zone accessed during retrolabyrinthine and translabyrinthine approaches to the posterior fossa.
PART 2: MASTOIDECTOMY - TYPES, INDICATIONS, AND TECHNIQUE
2.1 What is Mastoidectomy?
Mastoidectomy is a surgical procedure of the temporal bone that opens postauricular air cells by removing the thin bony partitions between them (exenteration of mastoid air cells), with the goal of:
- Eradicating disease
- Creating a safe, dry ear
- Restoring/preserving hearing
2.2 Indications
- Acute coalescent mastoiditis with subperiosteal abscess (emergency)
- Chronic suppurative otitis media (CSOM) with cholesteatoma
- Cholesteatoma (most common elective indication)
- Access route for cochlear implantation (facial recess approach)
- Access for acoustic neuroma (translabyrinthine approach)
- Chronic otitis media with intracranial complications (meningitis, lateral sinus thrombosis, epidural/subdural abscess, cerebral abscess, petrositis)
- Temporal bone malignancy (temporal bone resection)
2.3 Nomenclature - Types of Mastoidectomy
"The nomenclature for mastoid surgery is often confusing and may describe a variety of approaches and techniques."
- Cummings Otolaryngology
Standard mastoid procedures:
| Procedure | Description |
|---|---|
| Simple (Cortical) Mastoidectomy | Canal wall preserved; mastoid air cells exenterated; antrum opened; middle ear not entered |
| Canal Wall-Up (Intact Canal) Mastoidectomy | More complete air cell removal while maintaining posterior bony EAC wall; usually includes facial recess approach |
| Canal Wall-Down Mastoidectomy | Superior and posterior canal walls removed; creates common cavity between mastoid, antrum, and EAC; requires meatoplasty |
| Radical Mastoidectomy | CWD + tympanic membrane and lateral ossicular chain sacrificed + eustachian tube obliterated |
| Modified Radical Mastoidectomy (Bondy) | Disease limited to epitympanum exteriorized; uninvolved middle ear NOT entered; cholesteatoma matrix maintained as cavity lining |
| Mastoid Obliteration | Mastoid cavity filled with autogenous bone, cartilage, fat, or alloplastic material |
| Canal Reconstruction Mastoidectomy | Canal wall reconstructed after CWD to reduce long-term bowl care |
| Retrograde Mastoidectomy | Inside-out technique for cholesteatoma |
2.4 Surgical Steps - Canal Wall-Up Mastoidectomy
(The foundational operation - all other techniques build on this)
Pre-operative preparation:
- Continuous intraoperative facial nerve monitoring (mandatory)
- Preoperative audiogram
- CT temporal bone to delineate anatomy and disease extent
Step-by-step (from Cummings Otolaryngology):
Step 1 - Soft Tissue Exposure:
- Shave 1-2 cm of hair around the ear
- Inject 5-10 mL of 1% lidocaine with 1:100,000 epinephrine postauricularly and in the EAC
- C-shaped postauricular incision placed ~1 cm behind the postauricular crease (Fig. 143.3)
- Incision carried down to temporalis fascia superiorly; to anterolateral mastoid tip inferiorly
- Two periosteal incisions: one along the temporal line, one perpendicular extending to mastoid tip
- Periosteum elevated and retracted forward with the auricle
Step 2 - Cortical Exposure:
- Mastoid cortex fully exposed
- Identify surface landmarks: temporal line, spine of Henle, posterior EAC wall
Step 3 - Exposure of the Antrum:
- First burr cut: along the temporal line (approximates level of middle cranial fossa floor / tegmen)
- Second burr cut: perpendicular to first, tangential to external bony canal, carried inferiorly to mastoid tip
- Larger burrs (cutting/fluted) used for cortical bone
- Diamond burrs used when approaching facial nerve or sigmoid sinus
- Continuous saline irrigation to clear bone dust, prevent heat transfer
Step 4 - Identify Key Structures:
- Identify position of tegmen (superior) and sigmoid sinus (posterior)
- Exenterate mastoid air cells between these key structures
- Thin the external auditory canal; remove bone from the zygomatic root area
Step 5 - Open the Antrum:
- Identify and open the mastoid antrum
- Identify the short process of the incus (fossa incudis) - key landmark
- Identify the dome of the lateral semicircular canal - most reliable deep landmark
Step 6 - Facial Nerve Identification:
- Identify and skeletonize the mastoid segment of the facial nerve (CN VII)
- Nerve runs vertically just anterior to the digastric ridge
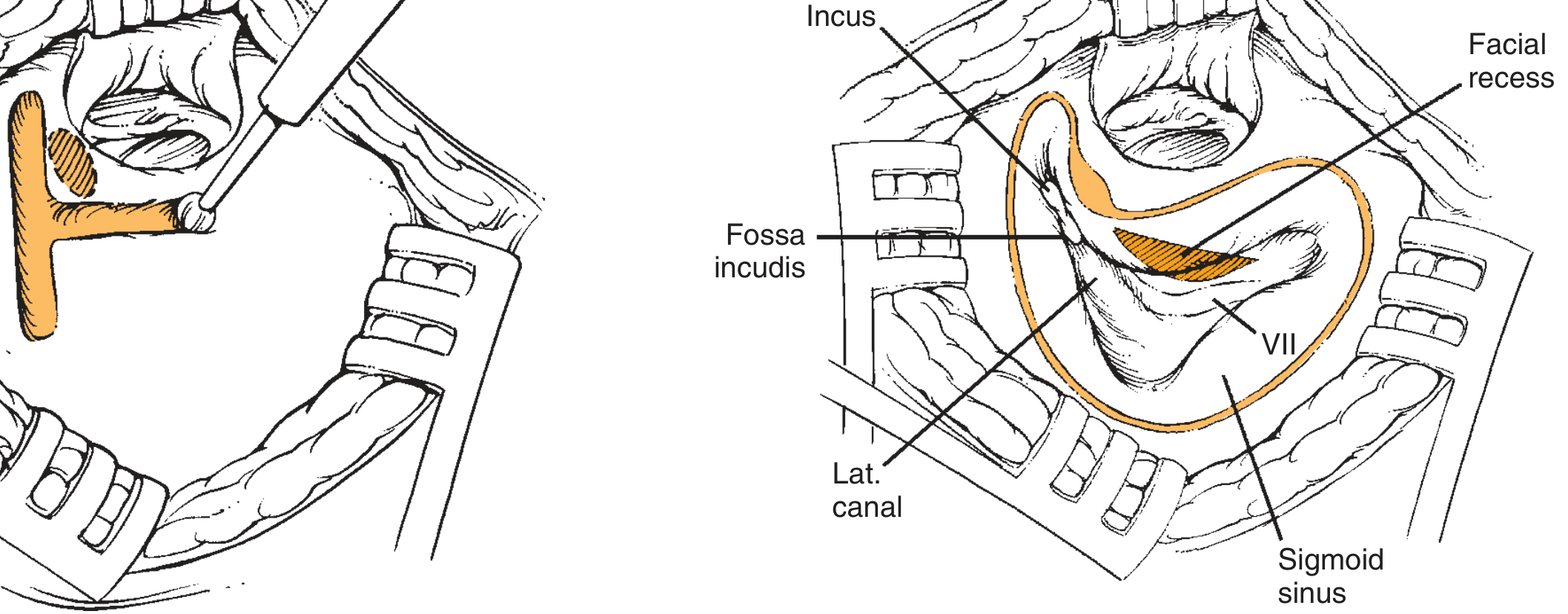
Step 7 - Facial Recess:
- Open the facial recess - the triangle bounded by the facial nerve (posteriorly), chorda tympani (anteriorly), and incus buttress (superiorly)
- This gives access to the posterior middle ear without disturbing the canal wall
- Used for cochlear implant electrode insertion
2.5 Canal Wall-Down Mastoidectomy - Additional Steps
Beyond the CWU technique, CWD also involves:
- Thorough removal of ALL mastoid air cells
- Aggressive saucerization of the cortical edges of the mastoid and tip
- Complete removal of the superior and posterior canal walls
- Meatoplasty (widening of the external meatus for cavity access and maintenance)
- Tympanic membrane usually reconstructed to create pneumatized middle ear space
Saucerization principle: The cavity must be saucerized so that the edges of the cavity slope smoothly outward, allowing epithelium to migrate naturally and reducing debris accumulation.
2.6 CWU vs CWD - Clinical Decision-Making
| Feature | Canal Wall-Up (CWU) | Canal Wall-Down (CWD) |
|---|---|---|
| Cholesteatoma recidivism | High: 25-45% | Lower: 6-20% |
| Residual disease detection | Harder (middle ear hidden) | Easier (only mesotympanum hidden) |
| Second-look surgery | Often required | Less often required |
| Healing | Faster | Slower (months) |
| Water tolerance | Better | Poorer (bowl care needed) |
| Hearing aid use | Well tolerated | Increased infection risk |
| Long-term bowl debridement | Not required | Often required |
| Children | Higher recidivism, significant concern | Preferred if disease is extensive |
Prefer CWD in:
- Only-hearing ear (single operation eradication preferred)
- Poor anesthetic risk patients
- Poor follow-up compliance
- Low-lying middle cranial fossa dura + anteriorly positioned sigmoid sinus (small mastoid - limits CWU exposure)
- Extensive disease found intraoperatively
- Poorly developed mastoid with sclerotic bone
2.7 Modified Radical Mastoidectomy (Bondy Procedure)
- Specifically for disease limited to the epitympanum
- Portions of the adjacent superior or posterior canal wall removed to exteriorize the disease
- The uninvolved middle ear is NOT entered
- Cholesteatoma matrix on the lateral surface of the ossicular heads is maintained in place as a lining for the cavity
- Defects of the canal and tympanic membrane are not repaired (unlike retrograde mastoidectomy)
- Suitable for small attic cholesteatomas
2.8 Radical Mastoidectomy
- Performed for extensive disease not amenable to less aggressive procedures
- All mastoid air cells removed + canal wall down
- Tympanic membrane sacrificed
- Lateral ossicular chain sacrificed (malleus head, incus)
- Eustachian tube obliterated
- Creates a large common cavity
- Hearing loss is significant and expected; no attempt at reconstruction
PART 3: COMPLICATIONS OF MASTOIDECTOMY
Intraoperative Complications
| Complication | Mechanism | Prevention |
|---|---|---|
| Facial nerve injury | Dehiscent nerve, altered anatomy, inadvertent burr contact | Continuous nerve monitoring; diamond burr near nerve; identify nerve early |
| Sigmoid sinus injury | Bleeding during exposure | Identify sinus early; compress with Surgicel/bone wax |
| Dural injury (tegmen) | Low-lying dura, aggressive drilling | Identify tegmen first; larger burrs |
| Labyrinthine fistula | Drilling over semicircular canals | Identify LSC dome; do not over-thin |
| Ossicular damage | Inadvertent drill contact | Identify short process of incus before deepening |
| Chorda tympani injury | Facial recess drilling | Identify and preserve |
Postoperative Complications
| Early | Late |
|---|---|
| Wound infection / hematoma | Recurrent/residual cholesteatoma |
| CSF leak (if dura breached) | Mastoid cavity problems (chronic otorrhea) |
| Facial nerve paresis | Conductive hearing loss |
| Sensorineural hearing loss | Canal stenosis |
| Vertigo/labyrinthitis | Tympanic membrane reperforation |
| Lateral sinus thrombosis | Meningoencephalocele |
Intracranial complications (from the disease process itself, often the reason for surgery):
- Meningitis
- Epidural/subdural abscess
- Intraparenchymal (brain) abscess
- Lateral sinus thrombosis
- Petrous apicitis (Gradenigo's syndrome)
PART 4: CLINICAL PEARLS - HIGH-YIELD SUMMARY
-
MacEwen's (Henle's) triangle - the suprameatal triangle on the posteromedial surface of the EAC - marks the position of the antrum on the surface (clinically useful to find the mastoid antrum).
-
"Safe" vs "unsafe" ear: Atticoantral disease (unsafe - associated with bone destruction and cholesteatoma) warrants mastoid surgery; tubotympanic disease (safe - only mucosal disease, no bone destruction) can usually be managed medically or with tympanoplasty alone.
-
Koerner's septum is a thin bony plate that is the embryologic fusion line between squamous and petrous temporal bone. It can falsely give the surgeon the impression of reaching the antrum - the true antrum lies medial to this.
-
Scutum (tympanic spine) - the lateral wall of the attic; its erosion on CT is an early sign of attic cholesteatoma.
-
Triad of danger: When drilling, always maintain awareness of the tegmen (superior), sigmoid sinus (posterior), and facial nerve (anterior-inferior) - these are the three structures that, if violated, can be catastrophic.
-
Citelli's angle (sinodural angle) - the angle between the sigmoid sinus and the dural plate. Citelli's abscess forms here in acute mastoiditis.
-
Canal wall-down cholesteatoma recidivism is 6-20% vs 25-45% in canal wall-up procedures - a major factor in choosing approach.
-
Second-look surgery after CWU at 9-12 months is standard to detect residual cholesteatoma, especially in children.
-
Facial recess = most important space in CWU mastoidectomy. Bounded by facial nerve, chorda tympani, and incus buttress. Opening it provides posterior middle ear access without removing the canal wall.
-
Cochlear implantation uses a modified CWU mastoidectomy with facial recess approach to insert the electrode array through the round window or cochleostomy.
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Ch. 143 (Mastoidectomy) and Ch. 126 (Temporal Bone Anatomy)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, Ch. 103 (Translabyrinthine/Cortical Mastoidectomy)
- StatPearls - Mastoidectomy (NCBI)
- Cleveland Clinic - Mastoidectomy
This is a shared conversation. Sign in to Orris to start your own chat.