Principles of left heart bypass (left aorta femoral bypass) university surgery exam
Reading File
Finding Sources
Finding Sources
Searching the Web
left heart bypass left aorta femoral bypass principles thoracic aortic surgery
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from four authoritative surgical textbooks plus the diagram. I have everything needed for a thorough exam answer.
Principles of Left Heart Bypass (Left Atrial-to-Femoral Bypass)
Definition and Rationale
Left heart bypass (LHB), also called partial bypass or left atrial-femoral bypass, is a form of distal aortic perfusion used during open repair of the descending thoracic aorta (DTAA) and thoracoabdominal aortic aneurysms (TAAA). The fundamental problem it solves is: application of a proximal aortic cross-clamp acutely increases left ventricular afterload and causes global ischemia in all structures distal to the clamp - spinal cord, kidneys, gut, and lower limbs.
"The application of vascular clamps to this major vessel acutely increases the afterload of the heart and produces global ischemia in all parts of the body distal to the clamp." - Miller's Anesthesia, 10e
Circuit Description
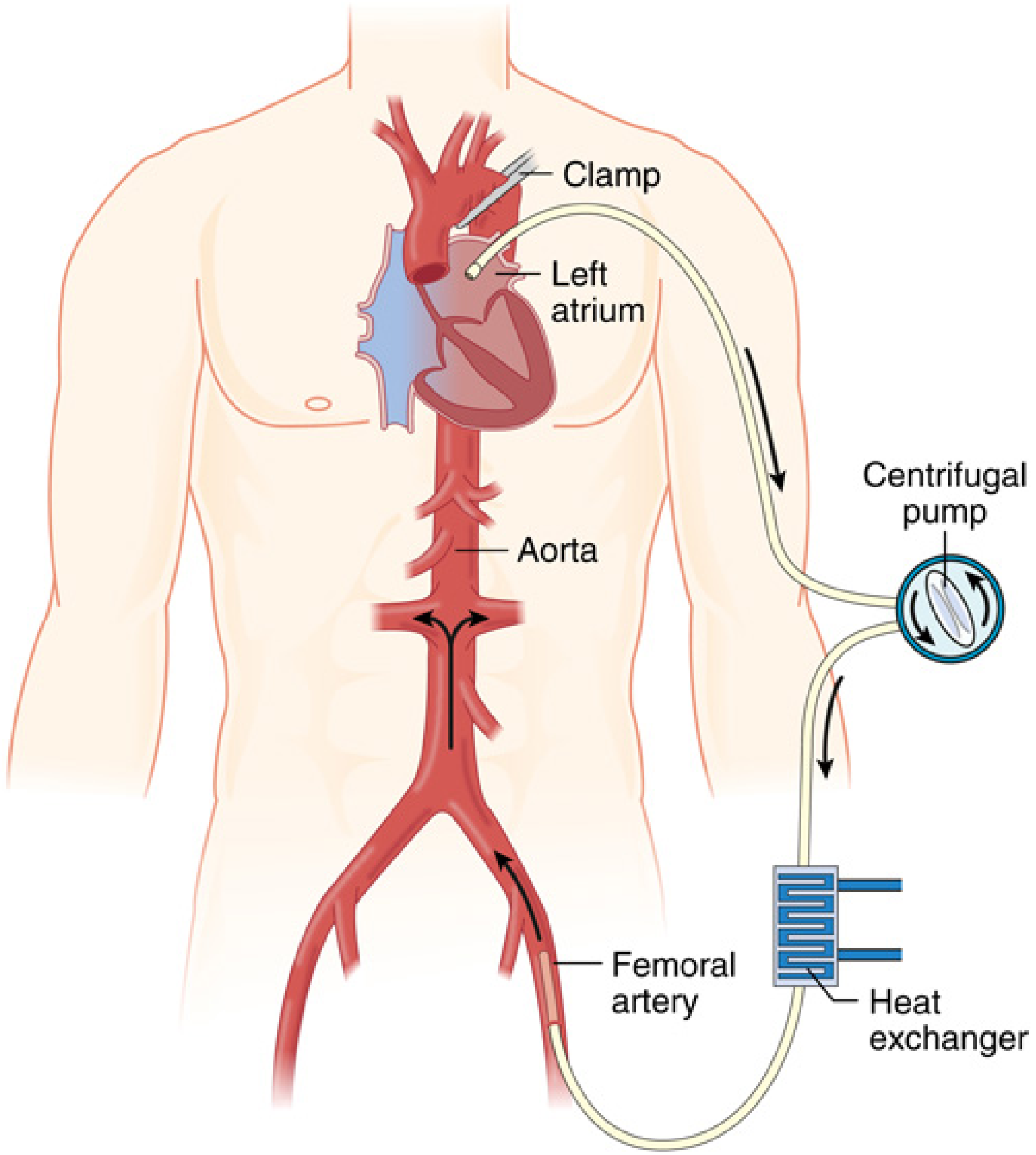
FIG. 52.8 - Diagram of left atrial-femoral bypass. The left atrium and left femoral artery are cannulated; a centrifugal pump is used with heparin-coated tubing. A heat exchanger may be added for cooling and rewarming. - Miller's Anesthesia, 10e
Components
| Component | Role |
|---|---|
| Inflow cannula | Left atrium (standard) or proximal descending aorta/aortic arch |
| Centrifugal pump (e.g. Biomedicus) | Provides non-pulsatile flow without roller pump |
| Heparin-coated tubing | Allows reduced anticoagulation |
| Outflow cannula | Left femoral artery (standard) |
| Heat exchanger (optional) | Allows mild hypothermia and rewarming |
| Oxygenator (in complex/complete circuit) | Added only if oxygenation support is needed |
Why No Oxygenator in Simple LHB?
Because only the left side of the heart is bypassed - oxygenated blood is drawn from the left atrium (post-pulmonary circulation) and returned directly to the systemic circulation. This contrasts with full cardiopulmonary bypass (CPB) which handles deoxygenated venous blood.
Physiological Goals
The two simultaneous targets during aortic cross-clamping are:
- Proximal arterial pressure (above clamp): Controlled to prevent left ventricular overload, hypertension, and myocardial strain
- Distal arterial pressure (below clamp): Maintained above 60 mmHg to perfuse the spinal cord, kidneys, and viscera
"The management goal is to keep arterial blood pressure higher than 60 mm Hg both proximal and distal to the aortic cross-clamp throughout the procedure." - Miller's Anesthesia, 10e
Mechanism of Cardiac Unloading
The effect on the left ventricle depends on the cannulation site:
| Cannulation Site | LV Effect | Mechanism |
|---|---|---|
| Left atrium (standard) | Reduces preload | Diverts LV filling; cardiac output falls |
| Aortic arch / proximal descending aorta | Reduces afterload | Bypasses resistance of cross-clamp |
Either way, proximal hypertension is controlled and the workload of the heart is decreased. Importantly, with left atrial cannulation and mild hypothermia (~30°C), approximately 15% of patients develop new atrial fibrillation - most revert on rewarming but direct cardioversion may be required.
Anticoagulation
- Standard LHB uses heparin-bonded (coated) tubing - full-dose systemic heparin is not required
- Typical heparin dose: 100 units/kg (rather than the 300-400 units/kg used for full CPB)
- ACT targets: 180-220 seconds (compared to >400 seconds for CPB)
- This reduced anticoagulation is important in trauma patients and those at bleeding risk
Circuit Variants
1. Simple LHB
- Left atrium → centrifugal pump → femoral artery
- No oxygenator, no reservoir
- Suitable for most elective DTAA/TAAA repairs
2. Complete LHB (Complex Circuit)
- Adds: oxygenator + heat exchanger + reservoir
- Indicated when the patient also has:
- Hypoxia (single-lung ventilation failure)
- Hypothermia risk
- Anticipated massive hemorrhage
- The reservoir is positioned out of the main blood pathway (unlike CPB), reducing the effective extracorporeal surface area and minimizing contact activation of blood
"The major difference between a complete LHB circuit and the standard CPB circuit is the position of the reservoir in the circuit." - Miller's Anesthesia, 10e
Operative Management During LHB
Hemodynamic Management
- Initial pump flow is set to approximately 50% of cardiac output when the proximal clamp is applied
- Flow is then titrated to achieve target proximal and distal pressures
- Vasodilators are rarely needed at initial clamping
- Careful coordination between surgeon, anesthesiologist, and perfusionist is mandatory
Sequential Aortic Clamping
- As repair proceeds from proximal to distal, the clamp is moved stepwise down the graft
- This restores perfusion to each newly anastomosed branch (intercostal/lumbar arteries) progressively
- Intercostal artery reimplantation can be done with minimal pump flow adjustments
Visceral and Renal Phase
- During reimplantation of visceral and renal vessels, pump flow is reduced significantly
- Distal perfusion is only to the lower limbs during this phase
- Balloon perfusion cannulas from the LHB circuit can deliver blood directly into the celiac axis and superior mesenteric artery orifices during reattachment - reducing bowel and hepatic ischemia
Protection of the Spinal Cord (Key Exam Topic)
LHB is part of a multi-modal strategy. Schwartz's Principles of Surgery outlines the full protocol:
For All Extents of TAAA Repair:
- Permissive mild hypothermia (32-34°C nasopharyngeal)
- Moderate heparinization (1 mg/kg)
- Aggressive reattachment of segmental arteries, especially T8-L1 (region of the artery of Adamkiewicz)
- Sequential aortic clamping when possible
- Perfusion of renal arteries with cold 4°C crystalloid
For Crawford Extent I and II (Highest Risk):
- Cerebrospinal fluid (CSF) drainage - reduces CSF pressure, improves spinal perfusion pressure (Class I, Level B evidence from RCT; reduced paraplegia from 13% to 2.6%)
- Left heart bypass during proximal anastomosis
- Selective perfusion of celiac axis and SMA during intercostal/visceral anastomoses
- Motor evoked potential (MEP) monitoring
Comparison: LHB vs. Clamp-and-Sew vs. Full CPB
| Feature | Clamp-and-Sew | LHB | Full CPB |
|---|---|---|---|
| Distal perfusion | None | Yes | Yes |
| Heparin dose | Low | Partial (100 U/kg) | Full (300-400 U/kg) |
| Oxygenator required | No | No (simple) | Yes |
| Spinal protection | Relies on speed | Active | Active |
| Best for | Short, isolated DTAA | Most DTAA/TAAA | Complex/cardiac failure |
| Risk of paraplegia | Highest | Reduced | Lowest (with arrest) |
Indications
- Repair of descending thoracic aortic aneurysm (DTAA)
- Repair of thoracoabdominal aortic aneurysm (TAAA) - all extents when cardiac reserve permits
- Open repair of acute aortic dissection (Type B / DeBakey III)
- Traumatic aortic injury (open repair)
- Patients with poor cardiac reserve - LHB unloads the LV which is particularly beneficial
Monitoring Requirements
- Two arterial lines: one in the right radial artery (above clamp) and one in the femoral artery (below clamp) - to continuously monitor both proximal and distal pressures
- Neuromonitoring: MEPs and/or SSEPs for spinal cord function
- NIRS cerebral and flank saturation probes
Complications Specific to LHB
| Complication | Cause |
|---|---|
| Proximal hypertension | Inadequate pump flow |
| Distal hypotension | Excessive pump flow "stealing" from proximal circuit |
| Atrial fibrillation (~15%) | Hypothermia + left atrial cannulation |
| Femoral artery injury | Cannulation site |
| Heparin-induced complications | Anticoagulation |
| Paraplegia (spinal cord ischemia) | Inadequate distal perfusion or failure to revascularize intercostals |
Note on flow dynamics - LHB acts opposite to normal CPB: increasing pump flow decreases proximal pressure and increases distal pressure. Decreasing pump flow has the reverse effect.
Summary
Left heart bypass is the preferred method of distal aortic perfusion for open thoracic aortic surgery. It draws oxygenated blood from the left atrium, drives it through a centrifugal pump with heparin-coated tubing (no oxygenator needed), and returns it to the left femoral artery, maintaining perfusion distal to the aortic clamp while simultaneously unloading the left ventricle. Initial pump flow is set to ~50% of cardiac output and titrated to keep distal mean pressure >60 mmHg. It is paired with mild permissive hypothermia, CSF drainage, sequential clamping, and selective visceral/renal perfusion to minimize the catastrophic complications of paraplegia and organ failure.
Sources: Miller's Anesthesia 10e; Schwartz's Principles of Surgery 11e; Current Surgical Therapy 14e; Sabiston Textbook of Surgery 21e
It's not enough for 10 marks ?
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Now I have everything needed for a complete 10-mark answer. Here is the full, expanded, exam-grade response:
Principles of Left Heart Bypass (Left Atrial-to-Femoral Bypass)
Complete 10-Mark Answer
1. Definition and Context
Left heart bypass (LHB), also called partial bypass or left atrial-to-femoral artery bypass, is a form of active distal aortic perfusion used during open repair of the descending thoracic aorta (DTAA) and thoracoabdominal aortic aneurysms (TAAA). It is the most commonly used distal aortic perfusion technique and is preferred over simple "clamp-and-sew" whenever cross-clamp time is expected to exceed 30 minutes.
2. The Problem It Solves: Effects of Aortic Cross-Clamping
Applying a vascular clamp to the thoracic aorta produces two simultaneous threats:
| Effect | Consequence |
|---|---|
| Acute increase in LV afterload (proximal to clamp) | Myocardial strain, proximal hypertension, LV distention |
| Global ischemia (distal to clamp) | Spinal cord ischemia (paraplegia), renal failure, bowel ischemia, lower limb ischemia |
The duration of cross-clamping is the single most important determinant of paraplegia and renal failure with the simple clamp-and-sew technique.
3. Circuit Setup and Components
Left atrial-femoral bypass circuit - Miller's Anesthesia, 10e
Blood flows: Left Atrium → Heparin-coated circuit → Centrifugal Pump → (Heat Exchanger) → Left Femoral Artery
| Component | Role |
|---|---|
| Inflow cannula - Left atrium (standard) | Withdraws oxygenated blood from left side of heart |
| Heparin-bonded tubing | Avoids need for full systemic anticoagulation |
| Centrifugal pump (Biomedicus) | Provides controlled, adjustable non-pulsatile flow |
| Heat exchanger (optional but beneficial) | Induces mild hypothermia (32-34°C) and allows rewarming |
| Oxygenator (added only in complex circuit) | Not needed in simple LHB - blood is already oxygenated |
| Outflow cannula - Left femoral artery | Returns blood to distal circulation |
Why no oxygenator? Because only the left (arterial) side of the heart is bypassed. Blood withdrawn from the left atrium is already fully oxygenated by the lungs. This distinguishes LHB from full cardiopulmonary bypass (CPB), which handles deoxygenated venous blood and requires an oxygenator.
4. Anticoagulation
- Full CPB requires: heparin 300-400 U/kg, ACT >400 seconds
- LHB requires: heparin 100 U/kg, ACT 180-220 seconds
- Heparin-bonded tubing reduces the extracorporeal surface area that activates the clotting cascade, allowing this reduced dose
- In trauma cases, the surgeon may choose to proceed without heparinization
5. Physiological Principles: Cardiac Unloading
The effect on the left ventricle depends on where the inflow cannula is placed:
| Inflow Site | LV Effect | Mechanism |
|---|---|---|
| Left atrium (standard) | Reduces preload | Diverts blood from LV filling; cardiac output falls |
| Aortic arch / proximal descending aorta | Reduces afterload | Bypasses the resistance imposed by the cross-clamp |
In either configuration: proximal hypertension is controlled, LV workload is reduced, and distal perfusion is restored. Because the circuit does not include a reservoir (unlike CPB), blood contact with artificial surfaces is minimized, reducing complement and clotting cascade activation.
6. Hemodynamic Management During LHB
- Mandatory: two arterial lines - one right radial (proximal, above clamp) and one femoral (distal, below clamp)
- Target distal mean pressure: >60 mmHg throughout clamping
- Initial pump flow: ~50% of cardiac output at time of clamp application, then titrated
- Vasodilators are rarely needed at onset of clamping
- Continuous coordination between surgeon, anesthesiologist, and perfusionist is essential
Critical rule: LHB flow dynamics are the opposite of normal CPB:
- Increasing pump flow → lowers proximal pressure, raises distal pressure
- Decreasing pump flow → raises proximal pressure, lowers distal pressure
7. Surgical Conduct: Sequential Clamping Strategy
- Proximal anastomosis phase: Clamp applied; LHB at ~50% CO; surgeon performs proximal graft anastomosis
- Intercostal reimplantation phase: Clamp moved sequentially downward as repair progresses; each segment reperfused progressively; intercostal arteries reimplanted with minimal flow adjustments
- Visceral/renal anastomosis phase: Pump flow is reduced significantly (distal perfusion now only to lower limbs). Balloon perfusion cannulas from the LHB circuit are placed directly into the celiac axis and superior mesenteric artery orifices to deliver oxygenated blood during their reattachment - reducing hepatic and bowel ischemia
- Renal protection: Kidneys perfused with cold 4°C crystalloid via separate catheters placed into renal orifices (independently confirmed by RCT to preserve renal function)
- Completion: Distal anastomosis completed, pump flow increased, patient actively warmed to 37°C
8. Spinal Cord Protection - The Critical Complication
Incidence of Paraplegia (without adjuncts):
- Coarctation repair: 0.5-1.5%
- DTAA repair: 0-10%
- TAAA repair: 10-20%
- Extensive (Crawford Extent II) dissecting TAAA: up to 40%
- With adjuncts (including LHB): reduced to ~7.2%
Anatomy of Spinal Cord Blood Supply:
- Anterior spinal artery (supplies 75% - motor tracts): formed from vertebral arteries, fed by anterior radicular arteries including the artery of Adamkiewicz (great anterior radicular artery)
- Artery of Adamkiewicz - usually branches from the aorta at T9-T12 (range T7-L2), predominantly on the left side - this is the most vulnerable vessel
- Posterior spinal arteries (25% - sensory tracts): from posterior cerebellar and vertebral arteries
How LHB Protects the Spinal Cord:
- Maintains perfusion pressure to the collateral network (intercostal/lumbar arteries feeding the anterior spinal artery) while segmental perfusion is interrupted
- Aortic cross-clamping raises CSF pressure by 10-15 mmHg, compressing spinal cord perfusion pressure
- Spinal cord perfusion pressure = Distal mean aortic pressure - CSF pressure (or CVP, whichever is greater)
- LHB keeps distal aortic pressure >60 mmHg, directly protecting this equation
Reimplantation of Intercostal Arteries:
- Ligation of T9-T12 intercostals significantly increases neurologic deficit risk
- Patent intercostals in this region should be reimplanted as one large patch, separate buttons, or with interposition grafts
- Decision guided by intraoperative MEP loss and/or preoperative identification of the artery of Adamkiewicz on CT/MRA or DSA angiography
9. Multi-Modal Organ Protection Strategy (Schwartz's, 11e)
LHB is never used in isolation. The complete protocol by Crawford extent:
For ALL TAAA Extents:
- Permissive mild hypothermia (32-34°C nasopharyngeal)
- Moderate heparinization (1 mg/kg)
- Aggressive reattachment of segmental arteries, especially T8-L1
- Sequential aortic clamping when possible
- Cold (4°C) crystalloid renal perfusion
Additional for Crawford Extent I and II (Highest Risk):
- CSF drainage - target CSF pressure ≤10 mmHg
- Prospective RCT (Coselli et al.): paraplegia rate reduced from 13% to 2.6% (80% relative risk reduction)
- Meta-analysis shows 10% absolute risk reduction
- Left heart bypass during proximal anastomosis
- Selective celiac/SMA perfusion via balloon cannulas during visceral anastomoses
- MEP monitoring intraoperatively
Note: Nitroprusside must NOT be used as an antihypertensive intraoperatively - it raises CSF pressure and causes systemic hypotension, worsening spinal cord perfusion.
10. Simple vs. Complete LHB vs. Full CPB
| Feature | Simple LHB | Complete LHB | Full CPB |
|---|---|---|---|
| Inflow | Left atrium | Left atrium | Right atrium/vena cava |
| Oxygenator | No | Yes | Yes |
| Heat exchanger | Optional | Yes | Yes |
| Reservoir | No | Yes (off-circuit) | Yes (in-circuit) |
| Heparin dose | 100 U/kg | 100-200 U/kg | 300-400 U/kg |
| Main indication | Most DTAA/TAAA | Hypoxia, hemorrhage risk | Complex arch, DHCA needed |
| Advantage | Simple, reduced anticoag | Manages hypoxia/hypothermia | Maximum protection |
| Disadvantage | Cannot manage oxygenation | More complex | High heparin, bleeding risk |
11. Complications of LHB
| Complication | Mechanism |
|---|---|
| Paraplegia | Inadequate distal perfusion pressure; failure to reimplant intercostals |
| Proximal hypertension | Insufficient pump flow |
| Distal hypotension | Excessive pump stealing from proximal |
| Atrial fibrillation (~15%) | Hypothermia + left atrial cannulation; most revert on rewarming |
| Femoral artery injury/thrombosis | Cannulation site |
| Renal failure | Inadequate renal perfusion/protection |
| Bleeding | Anticoagulation, extensive dissection |
| Subdural hematoma | Complication of CSF drainage (3.5% in one series) - related to high-volume drainage |
12. Indications and Surgical Approach
Indications:
- DTAA repair (especially if cross-clamp time >30 minutes)
- TAAA repair (Crawford Extent I-IV)
- Type B / DeBakey III aortic dissection - open repair
- Traumatic aortic transection (open repair)
- Poor cardiac reserve (LHB's LV unloading is especially valuable)
Surgical access:
- Left posterolateral thoracotomy (level depends on extent: 4th-5th interspace for extent I-II; 6th-7th for extent III; 8th for extent IV)
- Double-lumen ETT or bronchial blocker for single-lung ventilation
- Patient in right lateral decubitus, pelvis rotated 30° for femoral access
- Diaphragm divided circumferentially to preserve phrenic nerve branches
Summary (Exam Closing Points)
Left heart bypass is the standard of care for distal aortic perfusion during open thoracic aortic surgery. It draws already-oxygenated blood from the left atrium, propels it via a centrifugal pump through heparin-coated tubing (no oxygenator needed, reduced anticoagulation at 100 U/kg), and returns it to the femoral artery, maintaining distal pressure >60 mmHg while simultaneously unloading the left ventricle. Flow is initiated at ~50% cardiac output and titrated with two arterial lines above and below the clamp. It is always combined with mild hypothermia (32-34°C), sequential clamping, intercostal artery reimplantation (especially T9-T12, artery of Adamkiewicz territory), visceral/renal selective perfusion, and CSF drainage in high-risk extents. This multi-modal approach has reduced catastrophic paraplegia rates from 40% to under 8% in extensive TAAA repair.
Sources: Miller's Anesthesia 10e; Schwartz's Principles of Surgery 11e; Fischer's Mastery of Surgery 8e; Mulholland & Greenfield's Surgery 7e; Current Surgical Therapy 14e; Sabiston Textbook of Surgery 21e
This is a shared conversation. Sign in to Orris to start your own chat.