When to switch infliximab in ulcerative colitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
infliximab "ulcerative colitis" switching biologic loss of response
Finding Sources
Finding Sources
Searching PubMed
infliximab "ulcerative colitis" therapeutic drug monitoring optimization
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from the textbook. Let me compile the full answer.
When to Switch Infliximab in Ulcerative Colitis
The decision to switch infliximab centers on three distinct clinical scenarios, each requiring a different management pathway. The key principle from current guidelines is to use therapeutic drug monitoring (TDM) reactively - only when a patient has active persistent disease despite therapy.
Step 1: Define the Type of Failure
Primary Non-Response
- No meaningful benefit after the full induction regimen (5 mg/kg at weeks 0, 2, and 6)
- Should be apparent by the end of induction
- These patients are true non-responders to infliximab; dose escalation is unlikely to help
- Action: Switch mechanism - move to a biologic with a different mechanism (vedolizumab, ustekinumab) rather than another anti-TNF
Secondary Loss of Response (LOR)
- Patient had an initial response but subsequently reports diminished benefit
- Estimated at ~13% per year in IBD patients on infliximab
- Risk factors: prior anti-TNF exposure, low serum albumin, lack of concurrent immunomodulator
- Action: Measure trough levels and anti-drug antibodies (ADA) before switching
Step 2: TDM-Guided Decision Algorithm for Secondary LOR
| Finding | Interpretation | Action |
|---|---|---|
| Low trough level + No ADA | Pharmacokinetic failure (rapid clearance) | Dose escalate: increase from 5 mg/kg q8w to 10 mg/kg q8w, or shorten interval to q4-6w; add immunomodulator if not already on one |
| Low trough level + ADA present (low titer) | Immunogenic failure, potentially reversible | Add immunomodulator (azathioprine, 6-MP, or methotrexate); may rescue response |
| Low trough level + ADA present (high titer) | Immunogenic failure, likely irreversible | Switch - within class (adalimumab/golimumab) or out of class |
| Therapeutic trough level (≥5 μg/mL) + Active disease | Pharmacodynamic failure / escape mechanism | Switch mechanism - vedolizumab, ustekinumab, JAK inhibitor (tofacitinib); switching within anti-TNF class is unlikely to help |
- Yamada's Textbook of Gastroenterology (7th ed), p. 1349-1350, 1393-1394
Step 3: When to Switch Out of Class vs. Within Class
Switch within TNF class (e.g., infliximab → adalimumab or golimumab):
- Immunogenic failure with low or moderate ADA titers (especially if immunomodulator is added)
- Intolerance to IV administration / infusion reactions
- Note from the ULTRA-2 trial: 40% of adalimumab trial patients had prior infliximab loss of response, and adalimumab showed benefit (16.5% vs 9.3% remission at week 8)
Switch out of TNF class (vedolizumab, ustekinumab, tofacitinib, etc.):
- Primary non-response to infliximab
- Pharmacodynamic/true non-response with adequate drug levels
- High-titer ADA with no realistic chance of rescue
- Contraindication to further anti-TNF use (demyelinating disease, moderate-severe heart failure, recurrent serious infections, drug-induced lupus, lymphoma history)
- Tofacitinib is specifically approved only after TNF failure in UC
Step 4: Optimization Before Switching
Before declaring failure and switching, optimize:
- Ensure combination therapy - the UC-SUCCESS trial showed infliximab + azathioprine is superior to monotherapy for remission and endoscopic improvement, and reduces immunogenicity
- Dose escalation - can increase to 10 mg/kg every 4-8 weeks for secondary LOR with low levels but no ADA
- Assess concurrent disease triggers - rule out C. difficile, CMV colitis, non-adherence
- Biomarker reassessment - fecal calprotectin and CRP at 3-monthly intervals; endoscopy at 6-9 months post-initiation to confirm endoscopic activity (not just symptoms)
Important Caveats
- Proactive TDM is not routinely recommended - the TAXIT trial showed no significant improvement in clinical remission rates (69% vs 66%) with proactive drug concentration monitoring vs. clinical-feature-based management, though relapse rates were lower (7% vs 17%). Current guidelines recommend TDM only reactively.
- ADA at low levels may be transient - low-titer antibodies may disappear with continued scheduled dosing or addition of an immunomodulator, and should not automatically prompt switching.
- Assess for active disease objectively - symptoms alone can be misleading (IBS overlap, infection); confirm active inflammation before escalating or switching.
Switching Options After Infliximab Failure in UC
| Agent | Mechanism | Notes |
|---|---|---|
| Adalimumab | Anti-TNF (SC) | Within-class switch; evidence from ULTRA-2 in infliximab-exposed patients |
| Golimumab | Anti-TNF (SC) | Within-class; convenient SC dosing |
| Vedolizumab | Anti-α4β7 integrin (gut-selective) | Out-of-class; preferred if anti-TNF safety concerns (older age, cardiovascular risk, infection history) |
| Ustekinumab | Anti-IL-12/23 (p40) | Out-of-class; approved 2019 for UC; effective in TNF-exposed patients; very low immunogenicity (<5%) |
| Tofacitinib | JAK inhibitor (oral) | Approved only after TNF failure; risk of herpes zoster, thromboembolism in older patients |
- Yamada's Textbook of Gastroenterology (7th ed), pp. 1337-1354
Summary: Do not switch reflexively. Measure trough infliximab level and ADA when loss of response occurs. If levels are low without antibodies, escalate dose. If high-titer ADA or adequate levels with ongoing disease, switch - out of class being preferred in the latter scenario.
What is the evidence for switching within TNF-α inhibitors versus changing mechanism?
Finding Sources
Searching PubMed
"ulcerative colitis" "TNF" switching vedolizumab ustekinumab infliximab failure
Reading File
Searching PubMed
"ulcerative colitis" biologic switching vedolizumab ustekinumab anti-TNF
Reading File
Reading Article
PMID: 37057077
Reading Article
PMID: 40346848
Reading Article
PMID: 39743427
Reading Article
PMID: 40152278
Searching PubMed
VARSITY trial vedolizumab adalimumab ulcerative colitis
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the evidence needed. Here is the comprehensive answer.
Evidence: Within-Class TNF Cycling vs. Out-of-Class Mechanism Switch in UC
The Core Principle: Let TDM Guide the Decision
Before comparing strategies, the reason for failure determines the best next step. Sleisenger & Fordtran's makes this explicit:
"Patients with sufficient trough levels of the biologic agent will not benefit from continuing or escalating therapy and would benefit most from switching out of therapeutic class to a therapy acting by a different mechanism. Low or undetectable drug levels with high antibody titer should prompt a change to a different anti-TNF agent as there is low cross-reactivity between antibodies."
- Sleisenger and Fordtran's GI and Liver Disease, p. 2345
1. Within-Class Switching (TNF Cycling: infliximab → adalimumab/golimumab)
Rationale: Low cross-reactivity of anti-drug antibodies between different anti-TNF agents means that antibodies to infliximab (a chimeric IgG1) generally do not neutralize adalimumab or golimumab (fully human antibodies).
Clinical Evidence:
ULTRA-2 (adalimumab in UC): 40% of enrolled patients had prior infliximab exposure (loss of response or intolerance). In this TNF-experienced subgroup, adalimumab achieved clinical remission in 16.5% vs 9.3% placebo at week 8, maintained at 17.3% vs 8.5% at week 52 (p=0.004). This confirms within-class switching works - but remission rates are substantially lower than in TNF-naive patients.
VARSITY trial (vedolizumab vs adalimumab head-to-head, N=769): The figure below illustrates outcomes in TNF-experienced patients:
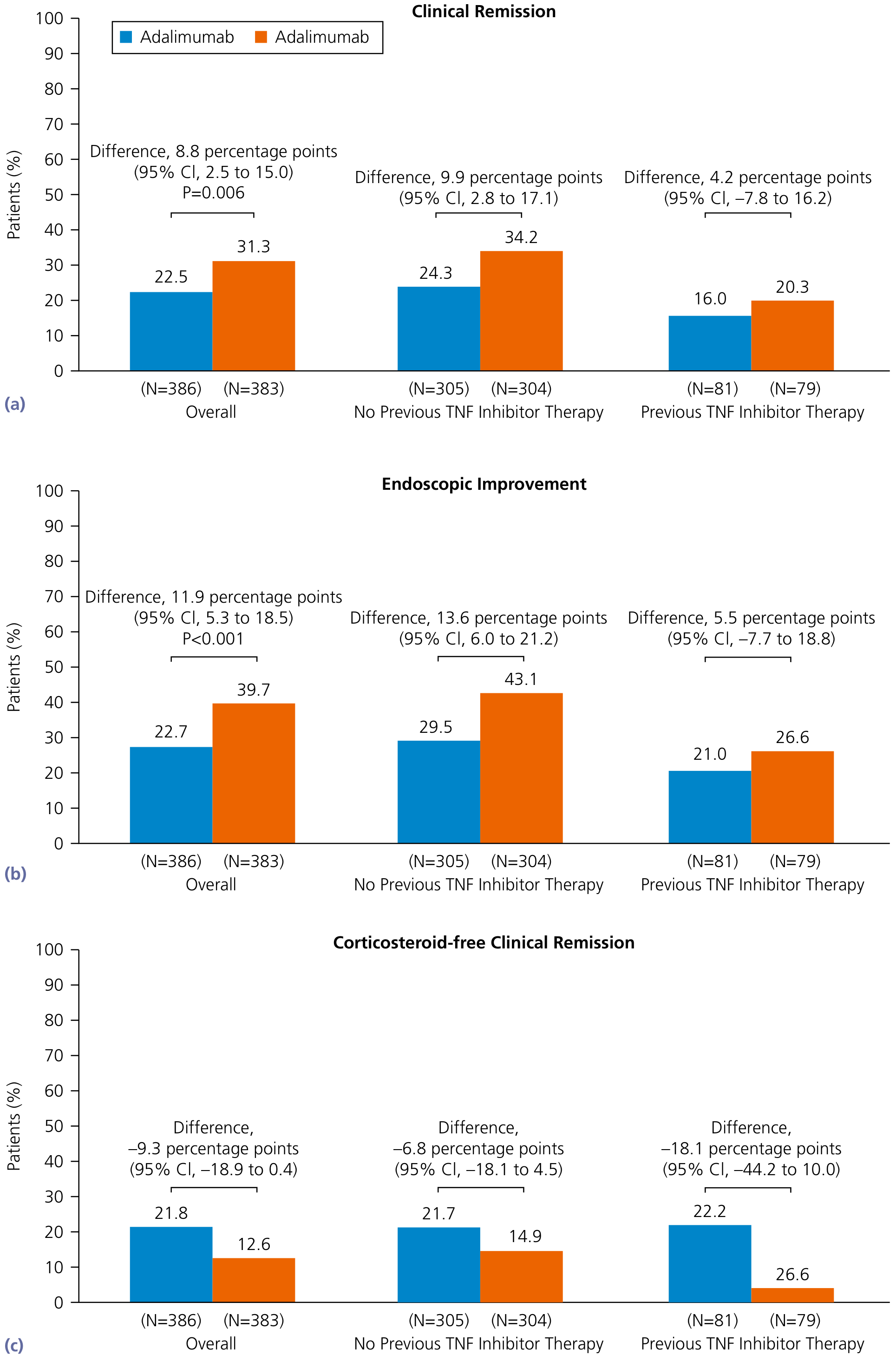
Key findings from VARSITY in prior TNF-inhibitor–exposed patients:
- Clinical remission at week 52: vedolizumab 20.3% vs adalimumab 16.0% (difference 4.2%; 95% CI -7.8 to 16.2 - not statistically significant)
- Endoscopic improvement: vedolizumab 26.6% vs adalimumab 21.0% (difference 5.5%; 95% CI -7.7 to 18.8 - not significant)
- Corticosteroid-free remission: adalimumab 22.2% vs vedolizumab 4.5% (vedolizumab numerically worse in this subgroup)
Important caveat: the TNF-experienced subgroup in VARSITY was small (n=160), so it was underpowered to detect a difference - but the trend favors vedolizumab for remission and endoscopic improvement.
- Yamada's Textbook of Gastroenterology (7th ed), p. 1355
2. Out-of-Class Switching: The Evidence Is Stronger
Vedolizumab (anti-α4β7 integrin)
- GEMINI 1 trial: ~47% clinical response at week 6 vs 25.5% placebo. Maintenance remission 42-45% vs 16% placebo at week 52.
- Limitation in TNF-experienced patients: Yamada's explicitly notes "the efficacy of vedolizumab is lower among those with prior anti-TNF failure." This is consistent across trials.
- Considered safer than anti-TNF (no systemic immunosuppression, very low immunogenicity ~5%), making it attractive when anti-TNF safety is a concern (older patients, infection risk, cardiovascular disease).
Ustekinumab (anti-IL-12/23, anti-p40)
- UNIFI trial: Studied 961 UC patients with and without prior anti-TNF exposure. Both TNF-naive and TNF-experienced patients responded, with significantly higher remission rates than placebo at week 8 and 44.
- Network meta-analysis advantage: A NMA of 7 RCTs in 1580 patients with prior TNF exposure found ustekinumab and tofacitinib were ranked highest for inducing clinical remission. Comparing active interventions:
- Ustekinumab vs adalimumab: OR 10.71 (95% CI 2.01-57.20)
- Ustekinumab vs vedolizumab: OR 5.99 (95% CI 1.13-31.76)
- Immunogenicity is very low (<5%), an advantage over anti-TNF cycling where re-immunization can occur.
- Yamada's Textbook of Gastroenterology (7th ed), p. 1349, 1353
Tofacitinib (JAK inhibitor - oral)
- Ranked alongside ustekinumab in the NMA for TNF-experienced patients (tofacitinib vs adalimumab: OR 11.05; tofacitinib vs vedolizumab: OR 6.18 for induction remission)
- Approved only after TNF failure in UC
- Concern: increased risk of herpes zoster, thromboembolism at 10 mg BID in older patients with cardiovascular risk factors
3. Real-World Comparative Data (Recent)
Zhdanava et al. 2025 (Clin Ther, IQVIA database, N=617 UC patients): Anti-TNF-experienced patients who switched to a different mechanism (ustekinumab or vedolizumab) vs those who cycled to another anti-TNF (adalimumab, infliximab, golimumab):
- 12-month treatment persistence: switch cohort 79.6% vs cycle cohort 64.9%
- Persistence on monotherapy: 74.6% vs 48.0% (HR 2.56, 95% CI 1.86-3.53)
- Persistence while corticosteroid-free: 60.1% vs 49.3% (HR 1.31, 95% CI 0.98-1.77 - not significant)
- Conclusion: "Patients with UC who switched to a biologic with a different mode of action were more persistent on treatment than patients who cycled to another anti-TNF agent."
- [PMID: 39743427]
Farkas et al. 2025 (Expert Opin Biol Ther, multicenter retrospective, N=683 UC after first anti-TNF failure):
- Ustekinumab had superior persistence and colectomy-free survival vs vedolizumab (p=0.02; p=0.05) and tofacitinib (p=0.05; p=0.001), and significantly higher persistence than cycling to another anti-TNF (p<0.001)
- Primary non-response to the first anti-TNF negatively predicted persistence with non-TNF agents (suggesting these patients may have disease biology less responsive to any biologic)
- Hypoalbuminemia increased colectomy risk; concomitant immunomodulator reduced it
- Conclusion: "Switching to a non-anti-TNF agent is worth considering in moderate-to-severe UC after first-line anti-TNF failure."
- [PMID: 40346848]
RUN-UC study 2025 (prospective observational, N=476 German UC patients, Bokemeyer et al.):
- 12-month treatment persistence: ustekinumab 93.9%, vedolizumab 87.0%, anti-TNF 75.0% (p<0.001)
- Clinical remission at 12 months: no statistically significant difference between groups (UST 26.9%, VDZ 40.9%, anti-TNF 34.7%; p=0.063)
- Higher persistence with ustekinumab despite similar efficacy - likely reflecting fewer adverse effects and immunogenicity
- [PMID: 40152278]
4. Optimal Sequencing: What the Evidence Suggests
| Scenario | Best Strategy | Evidence |
|---|---|---|
| High-titer ADA, low drug levels | Within-class switch (adalimumab/golimumab) | Low cross-reactivity; ULTRA-2 supports modest benefit |
| Low drug levels, no ADA | Dose escalate first; if inadequate, consider mechanism switch | Textbook guideline; TDM principle |
| Adequate drug levels, active disease (pharmacodynamic failure) | Mechanism switch (ustekinumab preferred > vedolizumab) | NMA data; Farkas 2025 |
| Primary non-response | Mechanism switch preferred; but note reduced efficacy with all biologics | Farkas 2025; UNIFI trial data |
| Safety concerns (elderly, infections, CVD) | Vedolizumab (gut-selective, safest profile) | GEMINI trial; safety data |
| Oral therapy preference | Upadacitinib or tofacitinib (after TNF failure) | U-ACHIEVE/U-ACCOMPLISH; OCTAVE |
Bottom line: The totality of evidence - NMA, real-world persistence data, and trial sub-analyses - favors out-of-class switching (especially ustekinumab) over within-class TNF cycling after infliximab failure in UC. Within-class cycling remains appropriate for immunogenic failure with low/moderate ADA titers or intolerance, but should not be the default strategy for pharmacodynamic failure.
- Yamada's Textbook of Gastroenterology (7th ed), pp. 1349-1356
- Bressler 2023 narrative review on optimal biologic sequencing in IBD (PMID: 37057077)
This is a shared conversation. Sign in to Orris to start your own chat.