
Screenshot_20260620-061057.png
Explain trophoboastic tumour with gross and microscopy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content and images needed for a thorough answer. Let me compile everything.
Gestational Trophoblastic Disease (GTD) - Trophoblastic Tumours
GTD encompasses a spectrum of tumours and tumour-like conditions characterised by proliferation of placental (trophoblastic) tissue. All elaborate human chorionic gonadotropin (hCG) to varying degrees. The major entities are:
- Hydatidiform Mole (Complete and Partial)
- Invasive Mole
- Choriocarcinoma
- Placental Site Trophoblastic Tumour (PSTT)
- Epithelioid Trophoblastic Tumour (ETT)
1. HYDATIDIFORM MOLE
Etiology / Genetics
Both types result from fertilisation with an excess of paternal genetic material.
| Feature | Complete Mole | Partial Mole |
|---|---|---|
| Karyotype | Diploid (46,XX or 46,XY) | Triploid (69,XXY) |
| Embryo/fetus | Absent | May be present (growth restricted, anomalies) |
| Villous edema | All villi | Some villi |
| Trophoblast proliferation | Diffuse, circumferential | Focal, slight |
| Serum hCG | Greatly elevated | Less elevated |
| Risk of choriocarcinoma | 2.5% | Rare |
- Incidence: 1 in 1000-2000 pregnancies in the US; twice as common in Southeast Asia
- Risk is higher at extremes of reproductive life (teenagers and women 40-50 years)
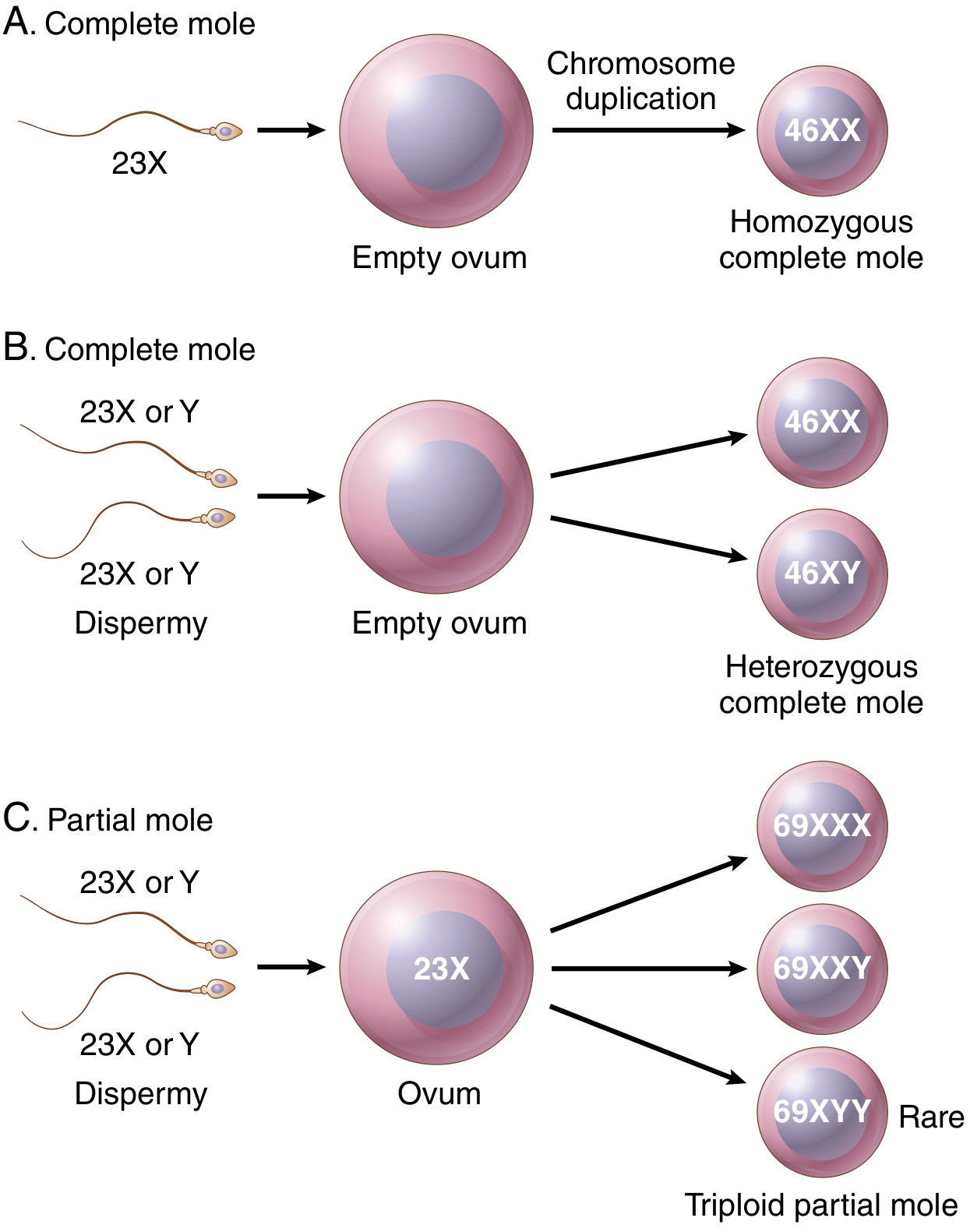
Complete Mole - Pathogenesis
- 90%: fertilisation of an "empty" egg (no maternal chromosomes) by a single sperm that undergoes chromosome duplication (monospermic androgenesis) → 46,XX
- 10%: dispermy (two sperm fertilise an empty egg) → 46,XX or 46,XY
- No embryonic development is possible
Partial Mole - Pathogenesis
- An egg with intact maternal chromosomes is fertilised by two sperm → triploid karyotype (69,XXY most commonly)
- Fetal development may occur but with lethal central nervous system and skeletal abnormalities (syndactyly)
GROSS MORPHOLOGY - Hydatidiform Mole
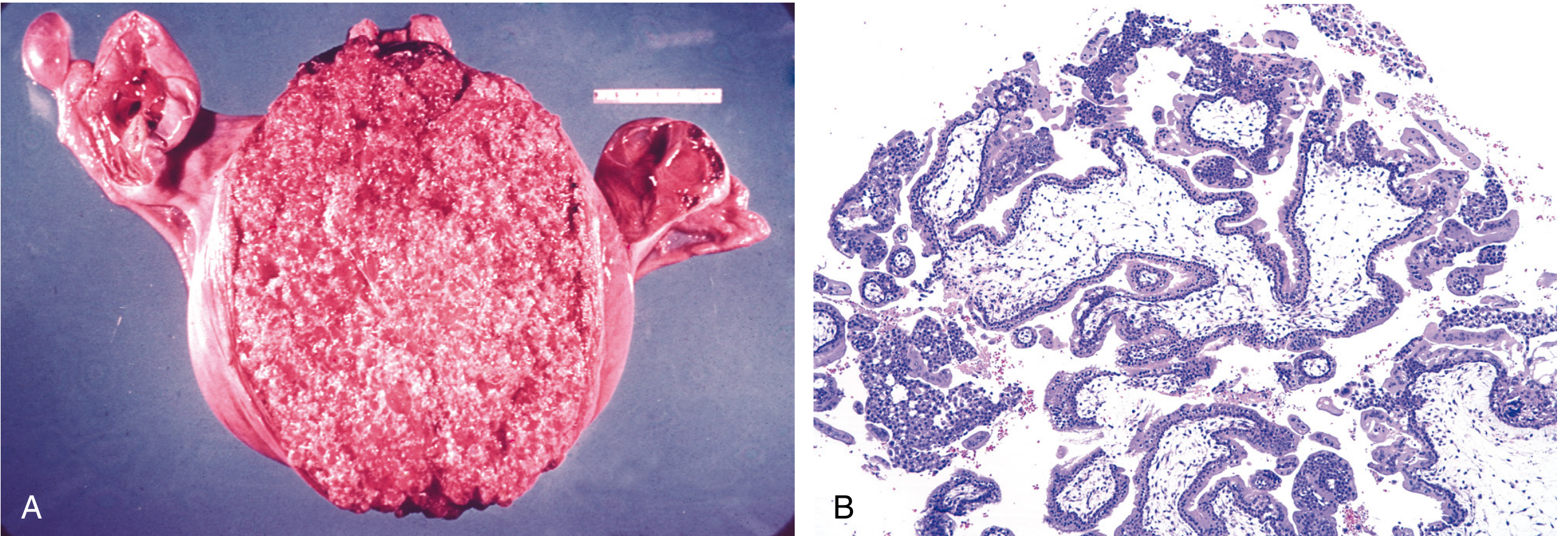
- The complete mole appears as a delicate, friable mass of thin-walled, translucent, cystic, grape-like structures - swollen oedematous (hydropic) villi that distend the uterus
- The partial mole shows only focal villous swelling; the rest of the villi appear normal
MICROSCOPY - Hydatidiform Mole
Complete mole (microscopy):
- All or most villi are affected
- Chorionic villi are enlarged, smooth, and oval with central cavitation (cisterns)
- Covered by circumferential biphasic trophoblast proliferation (both cytotrophoblast and syncytiotrophoblast)
- Loose, oedematous stroma; fetal blood vessels typically absent
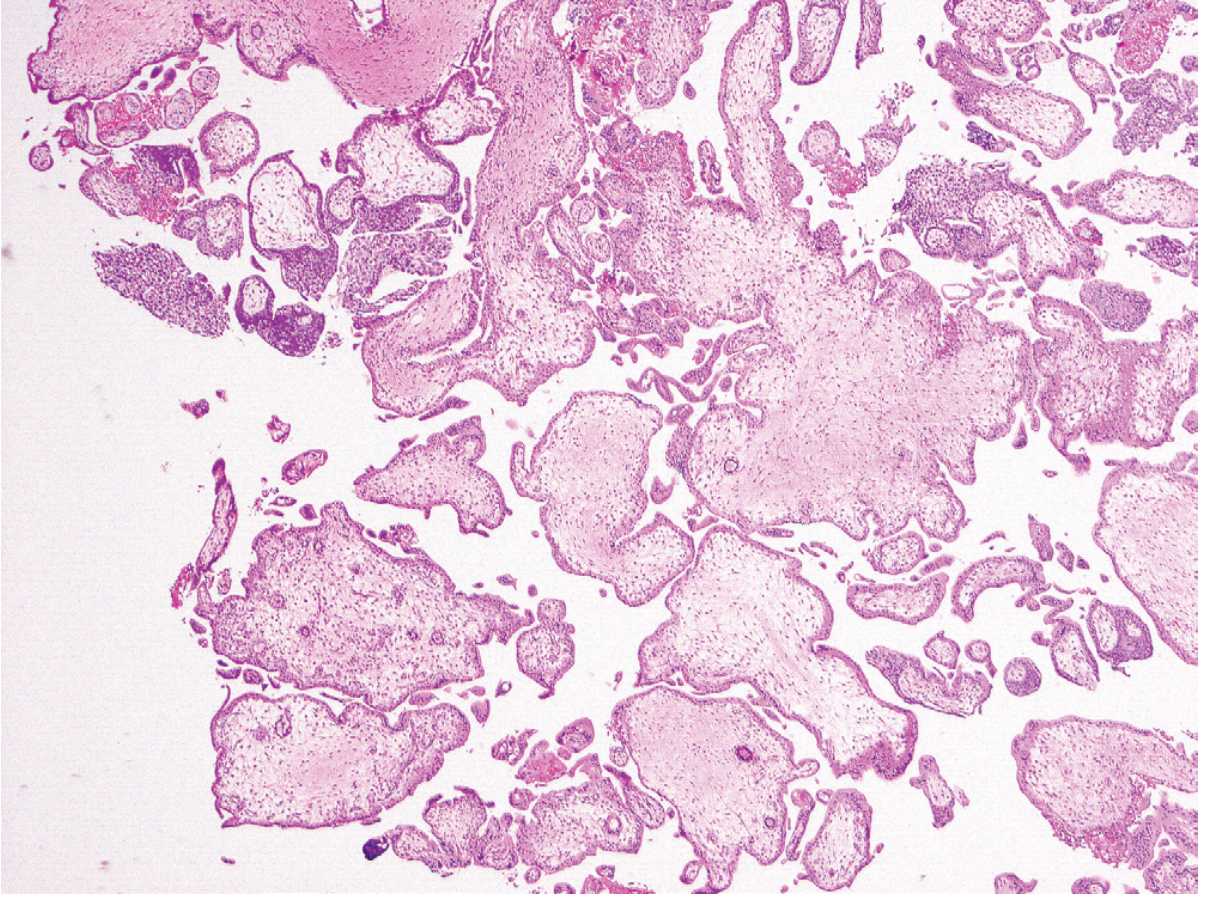
Partial mole (microscopy):
- Only some villi are enlarged; others are normal
- Trophoblast proliferation is focal and slight
- Irregular villous outlines; "scalloped" contour of villi
- Fetal/embryonic elements may be present
2. INVASIVE MOLE
Gross
- Infiltrative lesion that penetrates and sometimes perforates the uterine wall
- Haemorrhagic areas in the myometrium; hydropic villi visible within the muscle wall
Microscopy
- Hydropic chorionic villi lined by proliferating cytotrophoblast and syncytiotrophoblast invade the myometrium
- Villi may invade parametrial tissue and blood vessels; can embolise to lungs and brain (~5% of complete moles)
Clinical features
- Vaginal bleeding, irregular uterine enlargement, persistently elevated serum hCG after evacuation
3. CHORIOCARCINOMA
A malignant neoplasm of trophoblastic cells arising from a previously normal or abnormal pregnancy.
Incidence: 1 in 20,000-30,000 pregnancies
Antecedents: 50% arise from complete hydatidiform mole; 25% follow spontaneous abortions; ~22% follow normal pregnancies; remainder from ectopic pregnancies
GROSS MORPHOLOGY
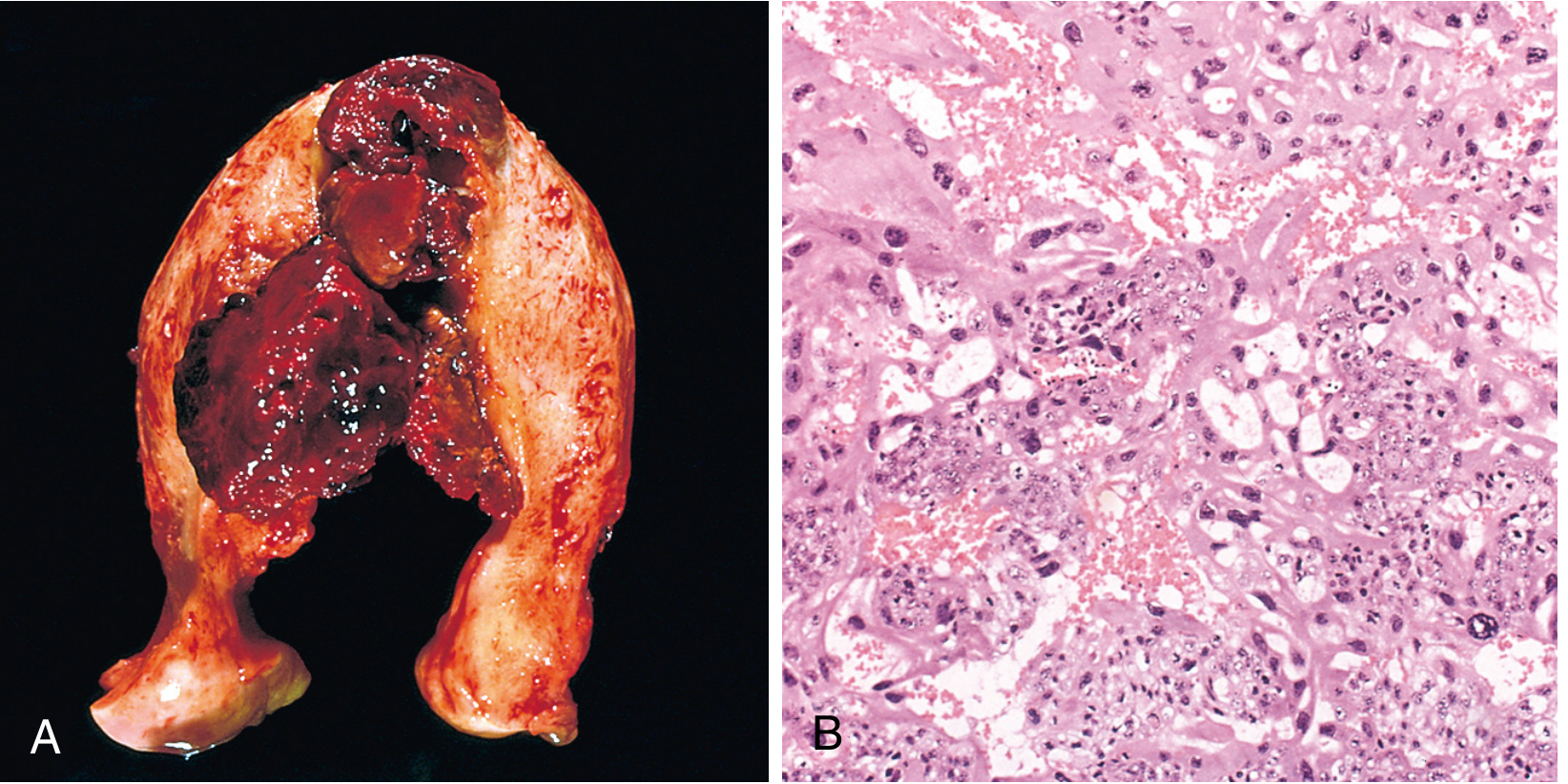
- Soft, fleshy, yellow-white tumour with large pale areas of necrosis and extensive haemorrhage
- Invades the myometrium and may extend to the uterine serosa and adjacent structures
- Bulky, destructive, haemorrhagic mass
MICROSCOPY
- Proliferating syncytiotrophoblasts and cytotrophoblasts arranged in sheets and columns
- Chorionic villi are ABSENT - this is the key distinguishing feature
- Abundant mitoses, sometimes abnormal
- Tumour invades the myometrium and penetrates blood vessels
- Extensive areas of necrosis and haemorrhage surrounding viable tumour at the periphery
Metastases
- Hematogenous spread is characteristic
- Lungs (50%), vagina (30-40%), brain, liver, bone, kidney - in descending frequency
- hCG is typically very elevated
Prognosis
- Despite widespread metastases, responds extremely well to chemotherapy (methotrexate ± actinomycin D)
- Near 100% remission rate; most patients can have normal subsequent pregnancies
4. PLACENTAL SITE TROPHOBLASTIC TUMOUR (PSTT)
Gross
- Uterine mass; may follow normal pregnancy (50%), spontaneous abortion, or hydatidiform mole
- Presents with abnormal uterine bleeding or amenorrhea; moderately elevated hCG (much lower than choriocarcinoma)
MICROSCOPY
- Composed of polygonal mononuclear or binucleated extravillous trophoblasts with abundant cytoplasm
- Invades without local destruction or haemorrhage (unlike choriocarcinoma)
- Shows tropism for maternal vessels
- No biphasic pattern (no syncytiotrophoblast sheets); no villi
Prognosis
- Localised disease: good prognosis with surgical removal alone
- 10-15% die of disseminated disease
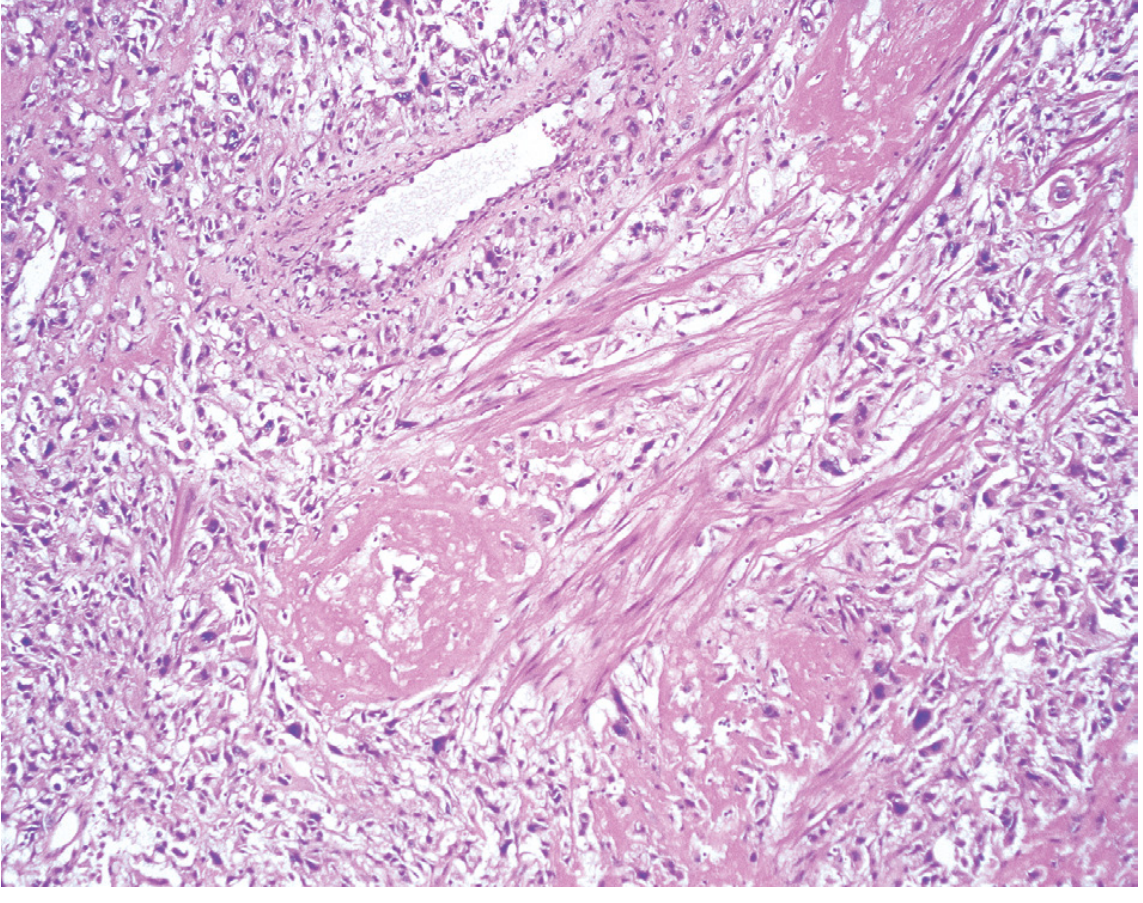
5. EPITHELIOID TROPHOBLASTIC TUMOUR (ETT)
Gross / Clinical
- Most commonly presents following pregnancy with amenorrhea, sometimes a palpable mass
- Most are intrauterine or cervical; extrauterine tumours also occur
MICROSCOPY
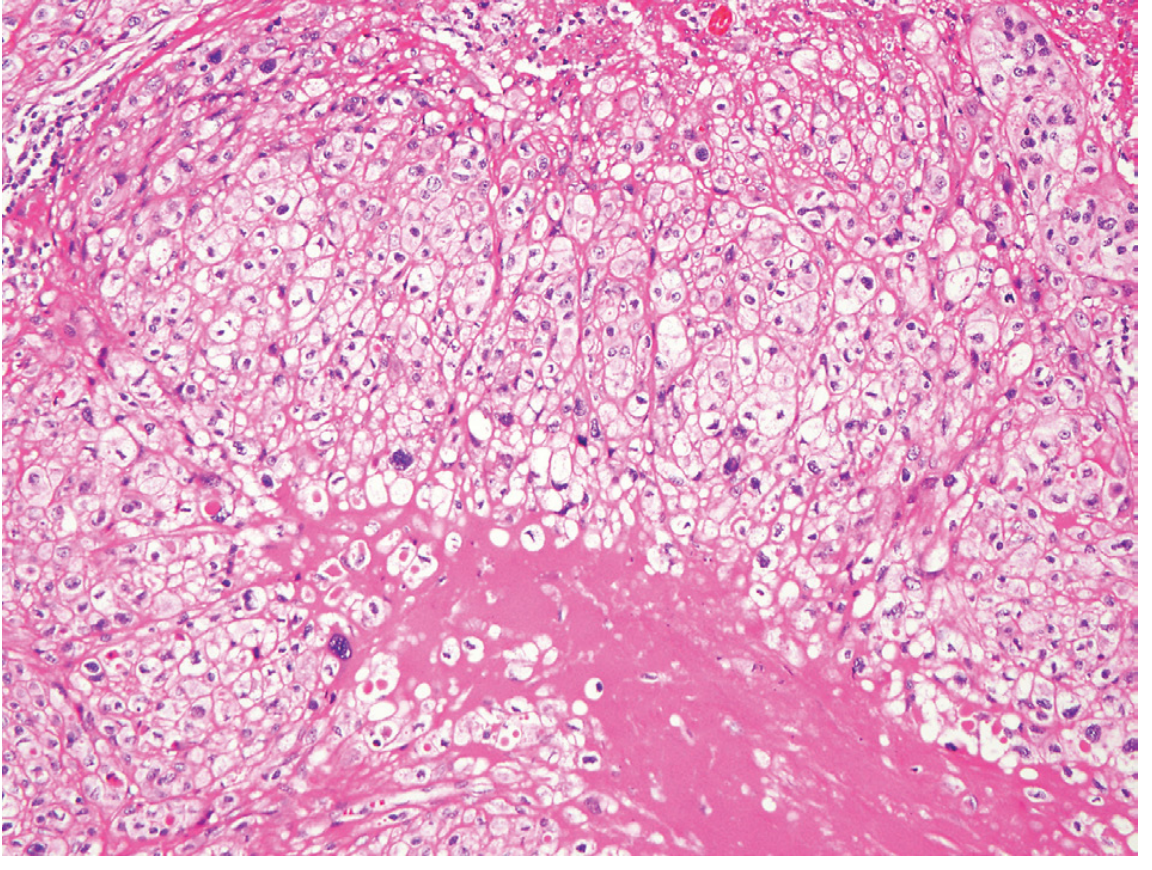
- Sheets of mononuclear trophoblast cells with abundant clear cytoplasm
- Characteristic pink hyaline material within the tumour
- Lacks the overt invasive/destructive features of PSTT
- Metastasises most commonly to lungs and bone
- ~10-15% of patients with metastatic disease eventually succumb
Summary Table
| Entity | Key Gross | Key Microscopy | hCG | Malignant potential |
|---|---|---|---|---|
| Complete Mole | Grape-like villi, distended uterus | All villi enlarged, cisterns, circumferential trophoblast hyperplasia | Very high | 2.5% → choriocarcinoma |
| Partial Mole | Focal villous swelling | Focal villi enlarged, scalloped outline, some normal villi | Moderately elevated | Low |
| Invasive Mole | Hydropic villi in myometrium | Villi + trophoblast invading muscle | Elevated | Local/metastatic |
| Choriocarcinoma | Haemorrhagic, necrotic uterine mass | Cyto + syncytiotrophoblast, NO villi, marked mitoses | Very high | High - but chemo-curable |
| PSTT | Uterine mass, no haemorrhage | Mononuclear extravillous trophoblasts, splits muscle fibres | Mildly elevated | 10-15% mortality |
| ETT | Intrauterine/cervical mass | Mononuclear cells, clear cytoplasm, hyaline material | Mildly elevated | 10-15% mortality |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar Basic Pathology (10th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.