Facial nerve anatomy detailed explanation and in simple way
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the content needed for a thorough, detailed yet simple explanation. Let me compile the complete answer.
Facial Nerve (CN VII) - Complete Anatomy
Overview
The facial nerve is the 7th cranial nerve (CN VII). It is primarily a motor nerve but carries 5 different fiber types, making it one of the most complex cranial nerves in the body. Think of it as a "mixed cable" - it controls your facial muscles, carries taste, controls tear and saliva production, and even carries some sensation.
1. Fiber Types - "What Does It Carry?"
The facial nerve trunk contains 5 distinct fiber types:
| Fiber Type | Function | What It Does |
|---|---|---|
| Special Visceral Efferent (SVE) | Motor (main) | Moves muscles of facial expression, stapedius, stylohyoid, posterior digastric |
| General Visceral Efferent (GVE) | Parasympathetic | Lacrimal gland (tears), submandibular & sublingual glands (saliva), nasal glands |
| Special Visceral Afferent (SVA) | Taste | Anterior 2/3 of tongue, soft palate |
| General Somatic Afferent (GSA) | Sensation | Skin of external auditory canal (EAC) and concha |
| Visceral Afferent | Sensation | Mucosa of nose, pharynx, palate |
Source: Shambaugh Surgery of the Ear
2. Nuclei - "Where Does It Come From?"
Three nuclei in the brainstem give rise to facial nerve fibers:
-
Motor nucleus - in the caudal pons. Drives all facial muscle movement.
- Upper part (forehead/eye muscles) gets input from both sides of the motor cortex (bilateral cortical input). This is clinically important!
- Lower part (mouth/cheek) gets input from the opposite side only (contralateral only).
- This is why in a stroke (UMN lesion), only the lower face is weak - the forehead is spared because it has bilateral representation.
-
Superior salivatory nucleus - dorsal to motor nucleus in the pons. Controls the parasympathetic secretomotor fibers (tears, saliva).
-
Nucleus of the solitary tract - in the medulla. Receives taste (gustatory) input.
3. Course of the Facial Nerve - The 5 Segments
Think of the facial nerve's journey in 5 stages - from brain to face:
Segment 1: Intracranial (Cisternal) - 24 mm
- Exits the pons (at the pontomedullary junction, between pons and olive)
- Travels through the cerebellopontine angle (CPA) cistern
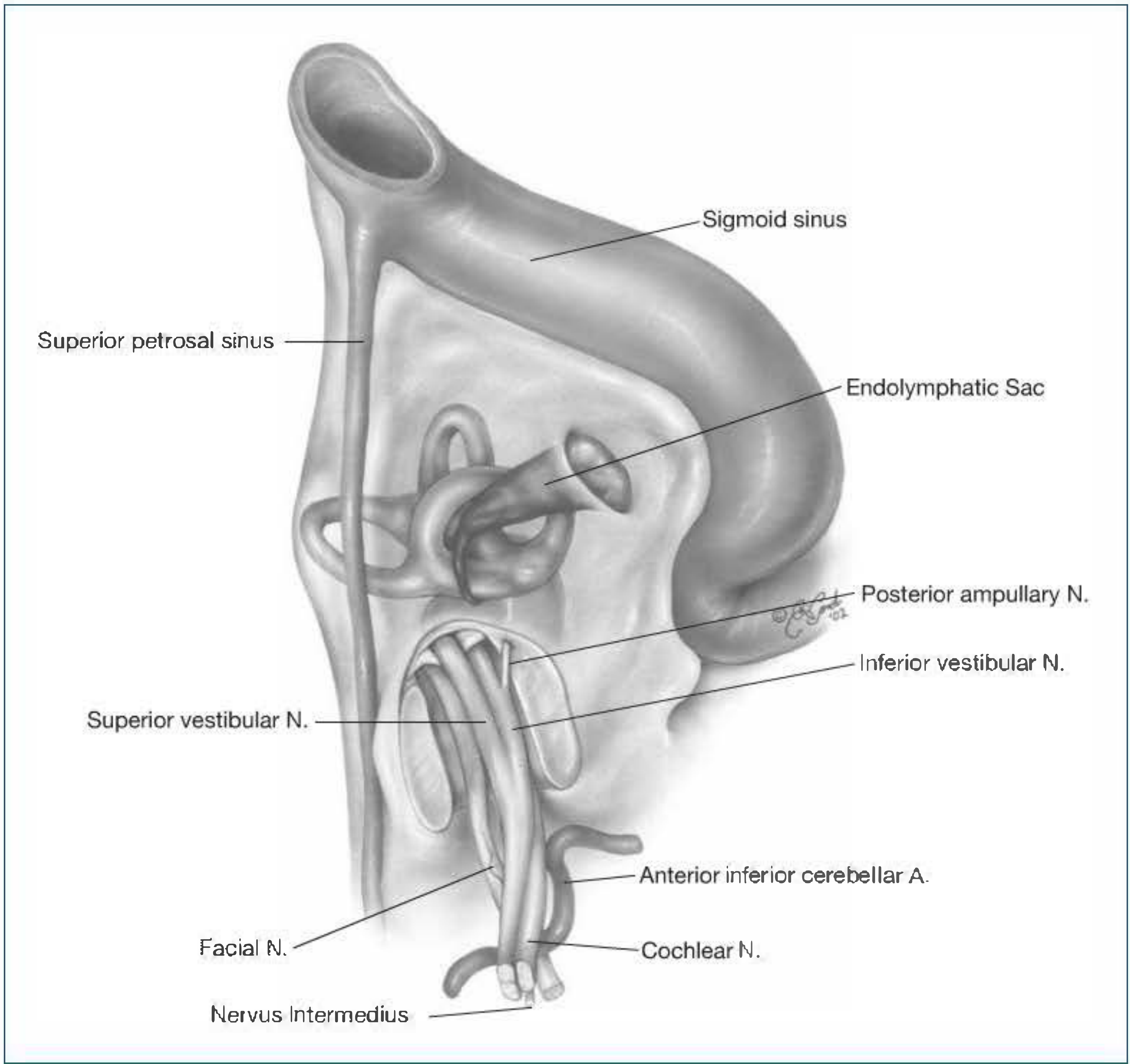
- Travels alongside CN VIII (vestibulocochlear nerve) and the nervus intermedius (see below)
- Enters the internal auditory meatus (IAM) via the porus acusticus
Segment 2: Intracanalicular (IAC) - variable
- Inside the internal auditory canal (IAC), CN VII sits in the anterosuperior quadrant
- CN VIII is posteriorly located
- At the lateral end (fundus) of the IAC, the nervus intermedius joins the main facial nerve trunk
Segment 3: Labyrinthine - 4 mm (shortest segment)
- Runs from the beginning of the fallopian canal (the bony canal for the facial nerve) to the geniculate ganglion
- Passes between the cochlea and vestibule
- Has the narrowest diameter of any part of the facial canal - this is why Bell's palsy edema here causes the most nerve compression
Segment 4: Tympanic (Horizontal) - ~13 mm
- At the geniculate ganglion, the nerve makes a sharp backward turn (the 1st genu)
- Runs horizontally in the medial wall of the middle ear
- Passes above the oval window and the cochleariform process
- Curves down at the 2nd genu (at the level of the lateral semicircular canal)
Segment 5: Mastoid (Vertical) - ~20 mm
- Runs vertically downward from the 2nd genu to the stylomastoid foramen
- Passes behind the external auditory canal
- Finally exits the skull through the stylomastoid foramen
Simple memory trick for segments: "I Eat Lime Teriyaki and Meat" = Intracranial, Extracranial (IAC), Labyrinthine, Tympanic, Mastoid
4. Intratemporal Branches - Inside the Skull
Three branches leave the facial nerve while it's still inside the temporal bone:
a) Greater (Superficial) Petrosal Nerve (GSPN)
- Arises from the geniculate ganglion (1st genu)
- Carries preganglionic parasympathetic fibers to the lacrimal gland (via the pterygopalatine ganglion)
- Also carries taste from the soft palate
- Emerges through the facial hiatus onto the floor of the middle cranial fossa
- Surgical traction on this nerve can cause facial palsy via hemorrhage or edema
b) Nerve to Stapedius
- Branches off the mastoid segment near the pyramidal eminence
- Supplies the stapedius muscle (dampens loud sounds)
- Damage = hyperacusis (sounds are painfully loud)
c) Chorda Tympani
- Leaves the facial nerve ~4 mm above the stylomastoid foramen
- Carries taste from anterior 2/3 of tongue
- Carries preganglionic parasympathetics to the submandibular and sublingual glands (for saliva)
- Ascends in its own canal, enters the middle ear through the iter chordae posterius
- Crosses the tympanic cavity: lateral to the long process of incus, medial to the malleus
- Exits via the iter chordae anterius (canal of Huguier) through the petrotympanic fissure
- Joins the lingual nerve (CN V3) in the infratemporal fossa
5. Extracranial Course - Outside the Skull
After exiting the stylomastoid foramen, the facial nerve:
- Gives off the posterior auricular nerve - supplies occipital belly of occipitofrontalis and auricular muscles
- Gives a muscular branch - supplies posterior belly of digastric and stylohyoid
- Enters the parotid gland - divides into upper (temporofacial) and lower (cervicofacial) divisions
- Passes through the parotid substance, branching further, then emerges as 5 terminal branches
6. Five Terminal (Peripheral) Branches
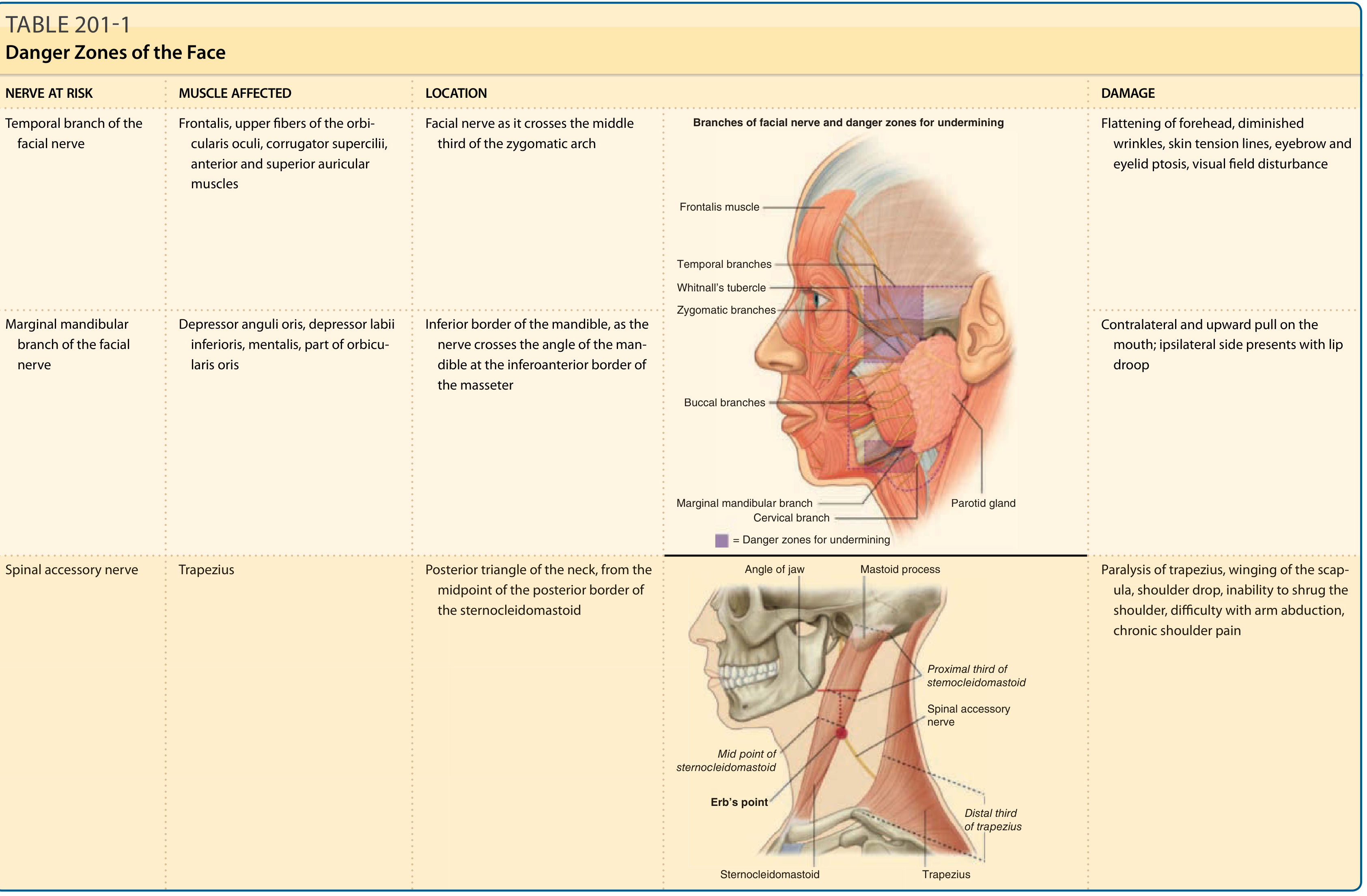
Memory mnemonic: "To Zanzibar By Motor Car"
| Branch | Muscles Supplied | Clinical Relevance |
|---|---|---|
| Temporal | Frontalis, upper orbicularis oculi, corrugator supercilii, anterior/superior auricular muscles | Most vulnerable - crosses mid-third of zygomatic arch just under skin |
| Zygomatic | Lower eyelid / orbicularis oculi (lower fibers) | Forms anastomotic network with buccal - less affected by single injury |
| Buccal | Buccinator, orbicularis oris, upper lip muscles | Also has anastomoses - resilient to injury |
| Mandibular (marginal) | Depressor anguli oris, depressor labii, mentalis, orbicularis oris | Most dangerous inferiorly - crosses mandible angle, no backup anastomoses |
| Cervical | Platysma | Least important clinically |
All terminal branches lie deep to the SMAS and enter muscles from their deep surface - so surgical procedures that remain superficial to fat are relatively safe. - Fitzpatrick's Dermatology
7. The Nervus Intermedius - "The Hidden Nerve"
- Also called the nerve of Wrisberg
- A separate small nerve bundle running between CN VII and the superior vestibular nerve in the IAC
- Carries all the non-motor fibers: taste, parasympathetic secretomotor, and sensory fibers
- Joins the main facial nerve trunk within the temporal bone
- The chorda tympani is essentially the "separation" of nervus intermedius sensory fibers at the inferior mastoid segment
8. Geniculate Ganglion - Key Relay Station
- Located at the 1st genu (bend) of the facial nerve at the end of the labyrinthine segment
- Contains the cell bodies of sensory neurons (taste and somatic sensation)
- Key branches arise here (GSPN)
- Viral reactivation here (Herpes zoster) = Ramsay Hunt Syndrome - causes painful ear vesicles, ipsilateral facial palsy, hearing loss, and vertigo
9. Fallopian Canal (Facial Canal)
- The bony canal the facial nerve travels through from the IAC to the stylomastoid foramen
- Has natural dehiscences (gaps) in many people, especially over the oval window area (~50% have some dehiscence)
- These gaps make the nerve vulnerable to infection, trauma, and cholesteatoma erosion
10. Clinical Correlations - Why This Anatomy Matters
| Lesion Level | Features Lost |
|---|---|
| Above geniculate ganglion (e.g., geniculate herpes) | Facial palsy + loss of lacrimation + loss of taste (anterior 2/3) + hyperacusis |
| Between GSPN and nerve to stapedius | Facial palsy + normal lacrimation + loss of taste + hyperacusis |
| Between nerve to stapedius and chorda tympani | Facial palsy + normal lacrimation + loss of taste + normal hearing |
| Below chorda tympani / at stylomastoid foramen | Facial palsy only - no taste, lacrimation, or hearing changes |
| UMN (stroke) | Lower face only weak - forehead spared (bilateral cortical representation) |
| LMN (Bell's palsy, Ramsay Hunt) | Entire ipsilateral face paralyzed including forehead |
Simple Summary Diagram (Text-Based)
BRAINSTEM (pons) → Cerebellopontine Angle → IAC → Labyrinthine segment
↓
GENICULATE GANGLION (1st genu)
↓ gives off: Greater Petrosal N. (to lacrimal gland)
↓
TYMPANIC segment (horizontal, over oval window)
↓
2nd genu (at lat. semicircular canal)
↓ gives off: Nerve to Stapedius
↓
MASTOID segment (vertical)
↓ gives off: Chorda Tympani
↓
STYLOMASTOID FORAMEN (exits skull)
↓ gives off: Posterior Auricular N.
↓
PAROTID GLAND (divides here)
___________↙ ↘___________
Temporofacial division Cervicofacial division
↓ ↓ ↓ ↓
Temporal Zygomatic Buccal Marginal Mandibular
+ Cervical
Sources:
- Shambaugh Surgery of the Ear, pp. 67-69 (segments, fiber types, intratemporal branches)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 (cisternal course, extracranial division)
- Gray's Anatomy for Students (parotid relationships, terminal branches)
- Fitzpatrick's Dermatology (mnemonic, danger zones, surgical relevance)
- Cummings Otolaryngology Head and Neck Surgery (clinical imaging correlations)
This is a shared conversation. Sign in to Orris to start your own chat.