Orciprenalline
Reading File
Finding Sources
Finding Sources
Searching the Web
orciprenalline metaproterenol pharmacology mechanism uses
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook content. Here is the full answer:
Orciprenalline (Metaproterenol)
Orciprenalline is the European name for metaproterenol - a moderately selective beta-2 adrenergic agonist bronchodilator. It belongs to the resorcinol structural class and is classified as a short-acting beta-2 agonist (SABA).
Chemical Structure & Class
Orciprenalline is structurally derived from isoproterenol (isoprenaline) but with a key modification: the hydroxyl groups are placed at positions 3 and 5 of the phenyl ring (resorcinol arrangement) instead of the catechol positions 3 and 4. This makes it a resorcinol bronchodilator, along with terbutaline and fenoterol.
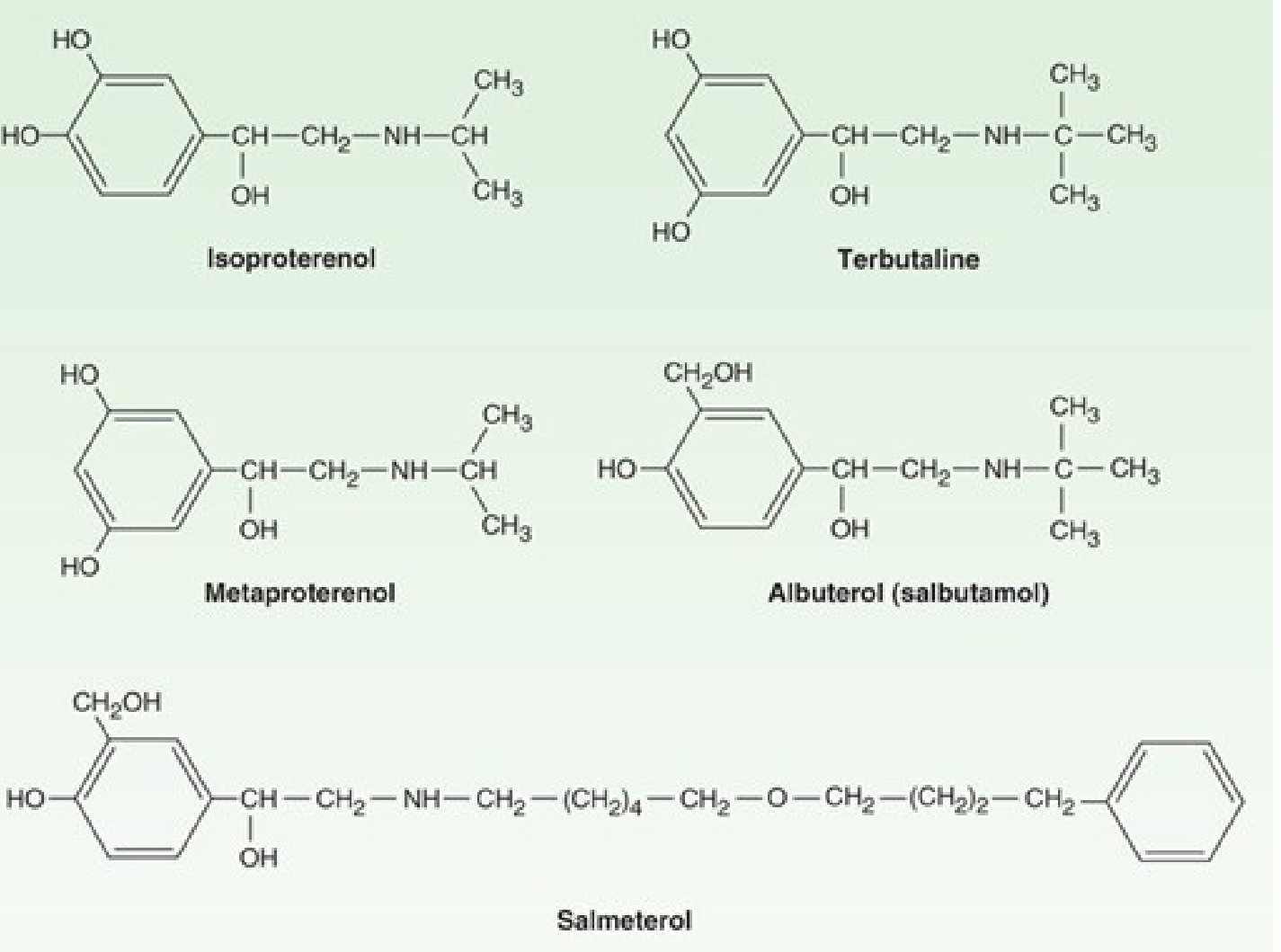
Structural comparison: note the 3,5-dihydroxy (resorcinol) arrangement in metaproterenol vs the 3,4-catechol in isoproterenol - Katzung's Basic and Clinical Pharmacology
Mechanism of Action
Orciprenalline acts by stimulating beta-2 adrenergic receptors on bronchial smooth muscle, leading to:
- Bronchodilation - relaxation of bronchial smooth muscle, decreased airway resistance
- Suppression of mediator release (leukotrienes, histamine) from pulmonary mast cells
- Enhanced mucociliary clearance
- Decreased microvascular permeability
- Possible inhibition of phospholipase A2
The beta-2 selectivity is moderate - it is considered less selective than albuterol or terbutaline, making it more prone to cause cardiac stimulation (beta-1 effects) at higher doses.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Pharmacokinetics
The resorcinol modification confers a major pharmacokinetic advantage:
- Resistant to COMT methylation (catechol-O-methyl transferase cannot act on it, unlike isoproterenol)
- ~40% oral bioavailability - a substantial fraction absorbed in active form after oral administration
- Not metabolized by MAO to a significant degree
- Excreted primarily as glucuronic acid conjugates
| Route | Onset | Duration |
|---|---|---|
| Inhalation | Within minutes | Several hours (3-4 h) |
| Oral | Slower (delayed) | 3-4 hours |
| Subcutaneous | Prompt | - |
- Goodman & Gilman's, Short-Acting beta Adrenergic Agonists section
Therapeutic Uses
- Asthma - acute bronchospasm and long-term management of obstructive airway disease
- COPD - bronchospasm relief; beta-2 selective drugs including metaproterenol are the preferred agents when administered as inhaled aerosols, especially in patients with cardiac disease
- Pulmonary function testing - used as a bronchodilator challenge agent in spirometry to assess reversibility of airflow limitation (a 15-20% improvement in FEV1 indicates reversible obstruction, as in asthma)
- Pregnancy - listed as an acceptable beta-2 agonist in pregnant patients with asthma
- K.J. Lee's Essential Otolaryngology; Murray & Nadel's Textbook of Respiratory Medicine
Route of Administration
- Metered-dose inhaler (MDI) - preferred route; minimizes systemic side effects
- Oral tablets/syrup
- Nebulized solution
- Subcutaneous injection
Inhalation is preferred because it delivers the greatest local bronchial effect with the least systemic toxicity. With aerosol delivery, 80-90% of the dose is deposited in the mouth/pharynx; optimal particles are 2-5 microns, and bronchial deposition is improved by slow inhalation and 5+ seconds of breath-holding.
Adverse Effects
| Effect | Mechanism |
|---|---|
| Tremor (most common) | Beta-2 in skeletal muscle; tolerance develops |
| Restlessness, apprehension, anxiety | CNS beta effects |
| Tachycardia / arrhythmia | Beta-1 activation (more so than albuterol) - especially with oral dosing |
| Hypokalemia | Beta-2 stimulation drives K+ into cells |
Patients tend to develop tolerance to tremor over time. The cardiac side effects are more pronounced than with albuterol due to orciprenalline's lower beta-2 selectivity.
Drug Interactions
- MAOIs - increase risk of adverse cardiovascular effects; concomitant use should be avoided
- Non-selective beta blockers (e.g., propranolol) - diminish or counteract the bronchodilatory effect
- At high concentrations, cardiac stimulation becomes more likely due to loss of beta-2 selectivity
Position in Therapy
Orciprenalline/metaproterenol has been largely displaced by more beta-2 selective agents such as albuterol (salbutamol) and terbutaline in most guidelines. Per Goodman & Gilman's, non-selective or less selective short-acting beta agonists like metaproterenol "should only be used as a last resort." Albuterol and levalbuterol are now the SABAs of first choice for acute bronchospasm.
It is not available as an inhaler in some countries (e.g., the US market for inhaled terbutaline is withdrawn; metaproterenol formulations have similarly declined).
Summary Table
| Property | Detail |
|---|---|
| Drug class | Short-acting beta-2 agonist (SABA); resorcinol bronchodilator |
| Selectivity | Moderate beta-2 selectivity (less than albuterol) |
| COMT metabolism | Resistant (resorcinol structure) |
| Oral bioavailability | ~40% |
| Duration of action | 3-4 hours |
| Primary use | Asthma, COPD bronchospasm |
| Main side effect | Tremor (most common); tachycardia with oral use |
| Current status | Largely replaced by more selective SABAs (albuterol) |
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic and Clinical Pharmacology, 16th ed.; Murray & Nadel's Textbook of Respiratory Medicine
Isoprenaline
Finding Sources
Searching the Web
isoprenaline isoproterenol pharmacology mechanism clinical uses
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent - I have comprehensive data from multiple top textbooks. Here is the full answer:
Isoprenaline (Isoproterenol)
Isoprenaline (INN) = isoproterenol (USAN). Also known as isopropyl noradrenaline, isopropylterenol, or INE. Brand name: Isuprel. It was the first selective beta-adrenergic receptor agonist ever developed, introduced clinically in 1947.
Chemical Structure & Class
Isoprenaline is a synthetic catecholamine - the N-isopropyl analogue of norepinephrine. Its full chemical name is d,l-β-[3,4-dihydroxyphenyl]-α-isopropylaminoethanol. It has the standard catechol (3,4-dihydroxyphenyl) ring, so it is:
- A substrate for COMT - metabolized relatively quickly
- A relatively poor substrate for MAO and the norepinephrine transporter (NET), so it is not taken up by sympathetic neurons to the same extent as norepinephrine/epinephrine
The bulky isopropyl group on the nitrogen confers high beta-receptor affinity and markedly reduces alpha-receptor activity.
Receptor Profile
| Receptor | Activity |
|---|---|
| Beta-1 | +++ (potent, cardiac) |
| Beta-2 | +++ (potent, vascular/bronchial) |
| Alpha-1 | Essentially none |
| Alpha-2 | Essentially none |
It is a potent, non-selective beta agonist with virtually no alpha activity - the defining characteristic that distinguishes it from epinephrine and norepinephrine. Per Guyton & Hall, it has "an extremely strong action on beta receptors but essentially no action on alpha receptors."
Pharmacological Actions
Cardiovascular Effects
The unique receptor profile creates a characteristic hemodynamic pattern:
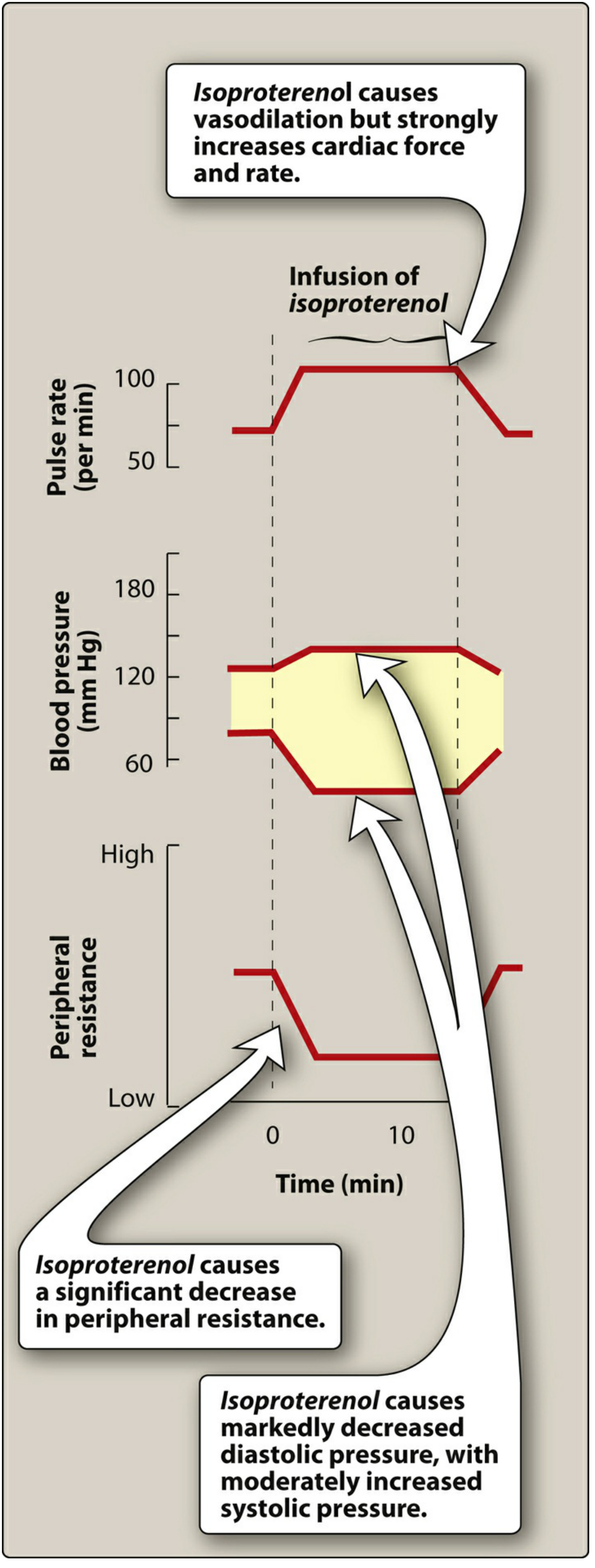
Cardiovascular effects of intravenous isoproterenol infusion - Lippincott Illustrated Reviews: Pharmacology
| Parameter | Effect | Mechanism |
|---|---|---|
| Heart rate | ↑↑↑ (tachycardia) | Beta-1: positive chronotropy |
| Myocardial contractility | ↑↑↑ | Beta-1: positive inotropy |
| Cardiac output | ↑↑ | Beta-1 effects |
| Peripheral vascular resistance | ↓↓↓ | Beta-2: vasodilation in skeletal muscle, renal, mesenteric, splenic beds |
| Systolic BP | ↑ (slight) or unchanged | Increased cardiac output |
| Diastolic BP | ↓↓ markedly | Peripheral vasodilation |
| Mean arterial pressure | ↓ | Net effect dominated by vasodilation |
| Pulse pressure | Widened | Systolic slightly up, diastolic down |
This produces the classic "hyperdynamic" pattern: strong cardiac stimulation + peripheral vasodilation + reduced diastolic BP. The fall in diastolic pressure also means coronary perfusion pressure decreases, which - combined with greatly increased myocardial O2 demand and shortened diastolic filling time - creates significant risk of subendocardial ischemia, even without coronary stenosis.
Bronchial Effects
- Potent bronchodilator via beta-2 stimulation of airway smooth muscle
- Inhibits antigen-induced release of histamine and other inflammatory mediators from pulmonary mast cells
- Relaxes almost all smooth muscle when tone is high, most pronounced in bronchial and GI smooth muscle
Other Effects
- Relaxes uterine smooth muscle (tocolytic effect via beta-2)
- Causes glycogenolysis and lipolysis
- CNS: mild stimulation
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Readily absorbed parenterally or by aerosol; poorly absorbed orally |
| Metabolism | Primarily by COMT in the liver; also in other tissues |
| MAO metabolism | Relatively poor substrate - not degraded by MAO as efficiently as NE/EPI |
| Neuronal uptake | Poor substrate for NET; not sequestered in sympathetic neurons |
| Duration | Relatively brief, but somewhat longer than epinephrine |
| IV half-life | ~2.5 to 5 minutes |
| IV duration | ~10 to 15 minutes |
Therapeutic Uses (Current & Historical)
Current / Active Uses
- Symptomatic bradyarrhythmias - refractory bradycardia as a bridge while awaiting cardiac pacemaker insertion
- AV (heart) block - pharmacological rate support; given as very dilute IV infusion (e.g., 2 mg in 500 mL normal saline)
- Torsades de pointes - drug-induced or acquired long QT; isoprenaline increases heart rate and shortens the QT interval, suppressing the arrhythmia
- Cardiac transplantation - to increase heart rate and contractility in the denervated donor heart (which lacks autonomic innervation and cannot respond to atropine)
IV dosing: Start infusion at 2 mcg/min, titrate every 5-10 minutes; usual range 2-10 mcg/min (titrated to adequate heart rate).
Historical Uses (Now Largely Replaced)
| Former Use | Replaced By |
|---|---|
| Asthma/bronchospasm | Beta-2 selective SABAs (albuterol, salbutamol) |
| Cardiogenic shock | Dopamine, dobutamine |
| Pulmonary hypertension/RV failure | Inhaled NO, prostacyclin (more selective, fewer side effects) |
| General bronchospasm | Selective beta-2 agonists |
In asthma: non-selective beta agonists like isoprenaline "should only be used as a last resort" (Goodman & Gilman's). Its cardiac effects (beta-1) are unwanted when treating airway disease.
Adverse Effects
| Effect | Basis |
|---|---|
| Palpitations, sinus tachycardia | Beta-1 chronotropy |
| Ventricular arrhythmias (PVCs, VT) | Beta-1 cardiac excitability |
| Supraventricular tachyarrhythmias | AV nodal acceleration (dromotropic) |
| Headache, flushing | Peripheral vasodilation |
| Hypotension | Marked beta-2 vasodilation |
| Myocardial ischemia / subendocardial necrosis | Increased O2 demand + reduced coronary perfusion pressure + shortened diastolic filling time |
| Pulmonary edema | With IV use |
| Dyspnea | Ventilation-perfusion mismatch worsening |
Large doses in experimental animals cause myocardial cell death from ischemia.
Contraindications
- Angina pectoris / coronary artery disease
- Pre-existing tachyarrhythmias or ventricular arrhythmias
- Digoxin toxicity (isoprenaline + digoxin increases arrhythmia risk)
- Underlying QT prolongation (use with extreme caution; the rate increase is needed for torsades but the drug itself is proarrhythmic in other settings)
Comparison with Related Drugs
| Drug | Alpha | Beta-1 | Beta-2 | Key Use |
|---|---|---|---|---|
| Isoprenaline | 0 | +++ | +++ | Bradycardia, heart block |
| Epinephrine | +++ | +++ | +++ | Anaphylaxis, cardiac arrest |
| Norepinephrine | +++ | +++ | + | Vasopressor (septic shock) |
| Albuterol | 0 | + | +++ | Asthma (inhaled) |
| Dobutamine | +/- | +++ | + | Cardiogenic shock (inotrope) |
Summary
Isoprenaline is a potent, non-selective beta agonist (beta-1 + beta-2) with negligible alpha activity. Its cardiovascular signature is: markedly increased heart rate and contractility + peripheral vasodilation + decreased diastolic BP. It has been largely displaced in most of its former uses by more selective agents, but retains a niche role in refractory bradyarrhythmias, AV block, torsades de pointes, and cardiac transplantation. Its proarrhythmic potential and adverse myocardial oxygen supply-demand effects limit its clinical application.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic and Clinical Pharmacology, 16th ed.; Barash, Cullen & Stoelting's Clinical Anesthesia, 9th ed.; Tintinalli's Emergency Medicine; Guyton & Hall Textbook of Medical Physiology
Difference between orciorenalline and isoprenalline
Based on the detailed coverage in our previous two responses, I can answer this directly and comprehensively without additional searches, as all the information is already in our conversation context.
Orciprenalline vs Isoprenaline - Key Differences
1. Chemical Structure
| Feature | Orciprenalline (Metaproterenol) | Isoprenaline (Isoproterenol) |
|---|---|---|
| Ring type | Resorcinol (OH at positions 3 & 5) | Catechol (OH at positions 3 & 4) |
| N-substituent | Isopropyl group | Isopropyl group (same) |
| Class | Resorcinol bronchodilator | Synthetic catecholamine |
This single structural difference - the position of the hydroxyl groups on the benzene ring - has profound downstream consequences.
2. Receptor Selectivity (Most Important Difference)
| Receptor | Orciprenalline | Isoprenaline |
|---|---|---|
| Beta-1 | + (weak) | +++ (potent) |
| Beta-2 | +++ (predominant) | +++ (potent) |
| Alpha | None | None |
- Isoprenaline is a non-selective beta agonist - equally potent at both beta-1 and beta-2
- Orciprenalline is a moderately selective beta-2 agonist - preferentially acts on bronchial smooth muscle, with less cardiac stimulation
- Orciprenalline's selectivity is still less than albuterol or terbutaline
3. Metabolism
| Feature | Orciprenalline | Isoprenaline |
|---|---|---|
| COMT substrate? | No - resorcinol ring resists COMT methylation | Yes - catechol ring is metabolized by COMT |
| MAO substrate? | No | Poor substrate (but metabolized more than orciprenalline) |
| Oral bioavailability | ~40% (active fraction absorbed) | Poor orally (destroyed in gut/liver) |
| Primary metabolites | Glucuronic acid conjugates | O-methylated products (COMT) + conjugates |
| Duration of action | Longer (3-4 hours) | Shorter (minutes IV; slightly longer than EPI) |
This is a key pharmacokinetic distinction: because orciprenalline is not a catechol, it escapes COMT degradation and can be given orally with meaningful bioavailability. Isoprenaline cannot.
4. Cardiovascular Effects
| Effect | Orciprenalline | Isoprenaline |
|---|---|---|
| Heart rate | Mild increase (oral/inhaled doses) | Marked tachycardia |
| Contractility | Minimal | Strongly increased |
| Systolic BP | Minimally affected | Slightly increased |
| Diastolic BP | Minimally affected | Markedly decreased |
| Peripheral resistance | Mild decrease | Marked decrease |
| Arrhythmia risk | Lower | Higher |
| Risk of myocardial ischemia | Low | Significant (increased O2 demand + reduced coronary perfusion) |
Isoprenaline's powerful beta-1 action causes the classic "hyperdynamic" pattern: strong cardiac stimulation + vasodilation + widened pulse pressure. Orciprenalline at therapeutic inhaled doses largely avoids this.
5. Routes of Administration
| Route | Orciprenalline | Isoprenaline |
|---|---|---|
| Inhalation (MDI/nebulizer) | Yes (preferred) | Yes (historical; now rarely) |
| Oral | Yes (40% bioavailability) | No (poorly absorbed) |
| IV infusion | Limited | Yes (primary route for cardiac indications) |
| Sublingual | No | Historically yes (now obsolete) |
6. Clinical Uses
| Indication | Orciprenalline | Isoprenaline |
|---|---|---|
| Asthma/bronchospasm | Yes (but 2nd line to albuterol) | Rarely - last resort only |
| COPD | Yes | No |
| Heart block / bradycardia | No | Yes - primary indication |
| Torsades de pointes | No | Yes |
| Cardiac transplantation | No | Yes (denervated heart) |
| Spirometry bronchodilator challenge | Yes | No |
| Uterine relaxation (tocolysis) | Acceptable in pregnancy | No |
7. Adverse Effect Profile
| Adverse Effect | Orciprenalline | Isoprenaline |
|---|---|---|
| Tremor | Common (most frequent) | Yes |
| Tachycardia/arrhythmia | Mild (mainly with oral dosing) | Prominent - main limiting toxicity |
| Myocardial ischemia | Rare | Clinically significant risk |
| Headache/flushing | Mild | Common (from vasodilation) |
| Hypotension | Mild | Marked (peripheral vasodilation) |
8. Current Clinical Status
| Orciprenalline | Isoprenaline | |
|---|---|---|
| Primary role today | Largely displaced by albuterol for airway disease | Niche cardiac use (bradycardia, torsades) |
| Guideline stance | "Last resort" for non-selective use in asthma | Retained for specific arrhythmia indications |
One-Line Summary
Orciprenalline is a moderately beta-2 selective, orally active, COMT-resistant bronchodilator used for airway disease. Isoprenaline is a non-selective, potent beta-1 + beta-2 agonist, catecholamine that is used primarily for cardiac indications (bradycardia, heart block, torsades de pointes) due to its powerful chronotropic and dromotropic effects - at the cost of significant cardiac toxicity risk.
The structural difference (resorcinol vs catechol) explains virtually all the pharmacokinetic differences; the receptor selectivity difference explains all the clinical differences.
This is a shared conversation. Sign in to Orris to start your own chat.