Healing pathway
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"wound healing"[MeSH Terms] AND "phases"
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a thorough answer. Here is the complete overview of the wound healing pathway:
Wound Healing Pathway
Wound healing is a complex, overlapping cellular and biochemical cascade that restores tissue integrity and function. It is traditionally divided into four phases: hemostasis, inflammation, proliferation, and remodeling. These phases are not strictly sequential - they overlap considerably.
Phase 1 - Hemostasis (Minutes to hours)
Immediately after injury, damaged vessels constrict (vasoconstriction) and the coagulation cascade is activated. Platelets adhere to exposed collagen and aggregate, forming a platelet plug. Thrombin converts fibrinogen to fibrin, reinforcing the clot. This clot (provisional matrix) serves both to stop blood loss and as a scaffold for infiltrating cells.
Degranulating platelets release a rich cocktail of growth factors that set the healing process in motion:
- Platelet-derived growth factor (PDGF) - recruits fibroblasts and smooth muscle cells
- Transforming growth factor-beta (TGF-β) - potent fibroblast chemoattractant and activator of collagen synthesis
- Epidermal growth factor (EGF) - stimulates epithelial proliferation
- Vascular endothelial growth factor (VEGF) - initiates angiogenesis
Phase 2 - Inflammation (Hours to ~5 days)
The inflammatory phase is characterized by infiltration of leukocytes into the wound. This has two sub-waves:
Neutrophils arrive first (within hours), peak at 24-48 hours, and are the predominant cell type for the first 2-3 days. They kill bacteria via phagocytosis, oxidative burst, and degranulation. They are largely replaced by...
Macrophages, which arrive by day 2-3 and become the dominant cell type by day 3. Macrophages are the master regulators of healing - they:
- Continue bacterial clearance
- Phagocytose debris and spent neutrophils
- Release growth factors (PDGF, TGF-β, VEGF, FGF) that drive the next phase
- Orchestrate the transition from inflammation to proliferation
Wounds depleted of macrophages fail to progress to the proliferative phase, underscoring their central importance. Lymphocytes also appear later in the inflammatory phase and modulate the response.
As per Schwartz's Principles of Surgery (11th ed.), p. 272: "All tissues heal by similar mechanisms, and the process undergoes phases of inflammation, cellular migration, proliferation, matrix deposition, and remodeling."
Phase 3 - Proliferation (Day 3 to ~3 weeks)
This phase encompasses three overlapping processes: fibroplasia, angiogenesis, and epithelialization.
Fibroplasia and Granulation Tissue Formation
Fibroblasts migrate into the wound (recruited by macrophage-derived PDGF and TGF-β) and proliferate, synthesizing the components of a new extracellular matrix. The result is granulation tissue - a combination of new capillaries, proliferating fibroblasts, and loose connective tissue that has a characteristic "granular" pink appearance.
Matrix deposition follows a predictable sequence:
- Fibronectin and collagen type III form the initial scaffolding
- Glycosaminoglycans and proteoglycans (e.g., hyaluronic acid, chondroitin sulfate) come next
- Collagen type I is the final and dominant matrix component
By several weeks post-injury, collagen content plateaus, but tensile strength continues to increase for months as fibril cross-linking proceeds.
Angiogenesis
New blood vessels grow from existing ones at the wound margin. This is driven by VEGF and bFGF. New capillary loops are essential to supply oxygen and nutrients to the metabolically active healing tissue.
Epithelialization
Epidermal cells at the wound margins begin migrating across the wound surface within 24 hours of injury. Marginal basal cells lose attachment to the dermis, enlarge, and migrate over the provisional matrix. Fixed basal cells nearby divide rapidly to supply the moving front. Cells migrate in a "leapfrog" fashion until the defect is covered, then resume their columnar shape and resume layering (re-stratification and keratinization).
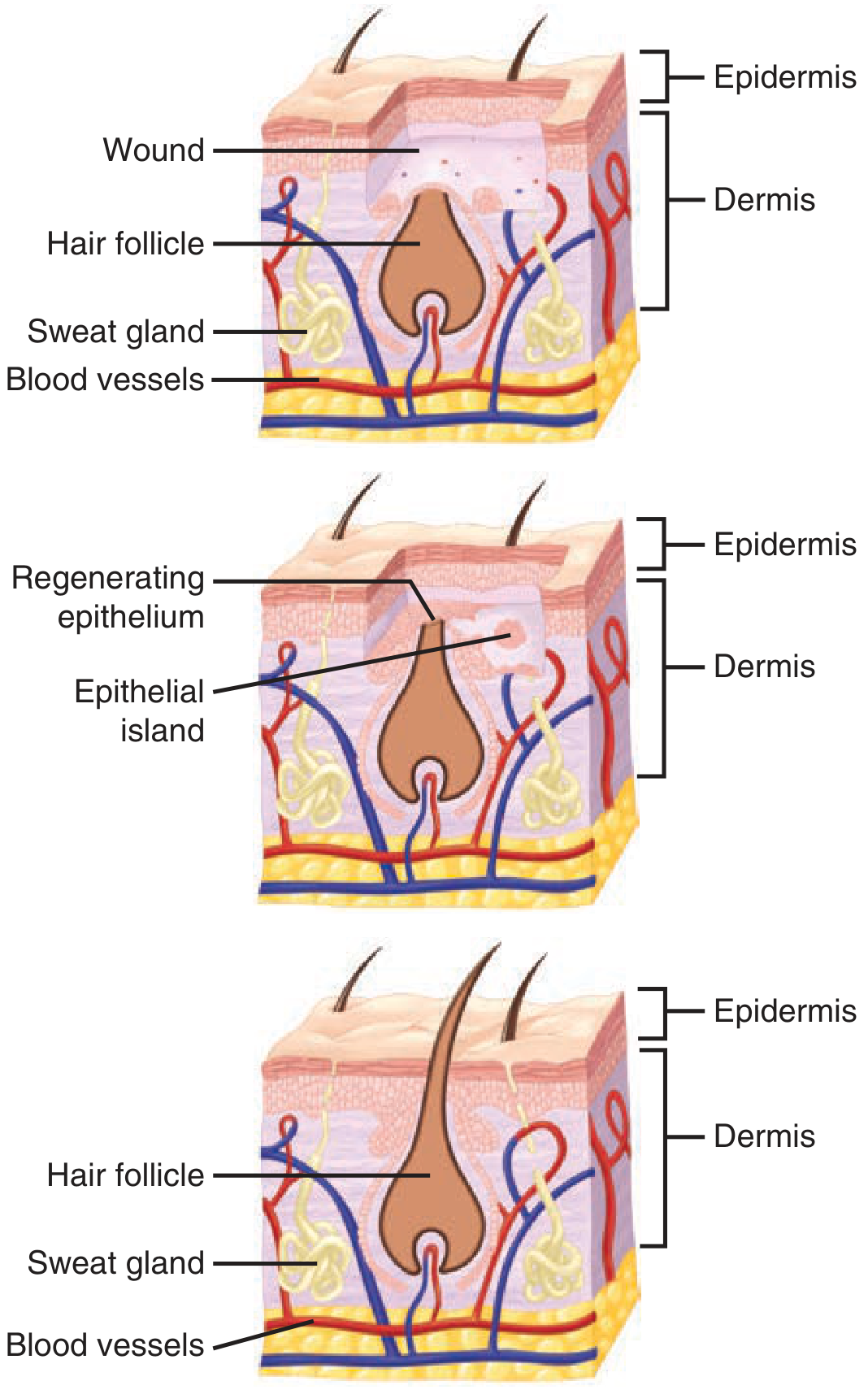
In approximated incised wounds, reepithelialization is complete in less than 48 hours. In larger wounds with significant defects, it may take considerably longer.
Key stimuli for reepithelialization include: loss of contact inhibition, exposure to fibronectin, and cytokines from immune cells (EGF, TGF-β, bFGF, PDGF, IGF).
Wound Contraction
Fibroblasts differentiate into myofibroblasts, which contain smooth muscle actin (alpha-SMA) and have contractile properties. They pull wound edges together, reducing wound size. Wound contraction is maximal at around 10-21 days and can reduce wound area by up to 80% in open wounds.
Phase 4 - Remodeling / Maturation (3 weeks to 1-2 years)
Once the wound has been filled and re-epithelialized, the extracellular matrix is progressively reorganized and strengthened. This is the longest phase.
- Type III collagen (weaker, early) is gradually replaced by type I collagen (stronger, organized along lines of stress)
- Fibril cross-linking (by lysyl oxidase) increases tensile strength
- Excess vascularity regresses - granulation tissue becomes an avascular, acellular scar
- MMPs (matrix metalloproteinases) degrade excess matrix; their activity is counterbalanced by TIMPs (tissue inhibitors of metalloproteinases), regulated largely by TGF-β
Important limitation: Scar tissue never fully recovers the mechanical strength of normal tissue. Remodeled scar achieves a maximum of approximately 70-80% of normal skin tensile strength.
Remodeling continues for 6-12 months post-injury.
Types of Wound Healing
| Type | Description | Example |
|---|---|---|
| Primary intention | Wound edges approximated surgically; minimal scar | Sutured surgical incision |
| Secondary intention | Wound left open; fills by granulation and contraction | Abscess cavity, pressure ulcer |
| Tertiary intention (delayed primary) | Wound initially left open, closed later (e.g., after infection clears) | Contaminated trauma wound |
Key Growth Factors in Healing
| Growth Factor | Source | Key Role |
|---|---|---|
| PDGF | Platelets, macrophages | Fibroblast migration/proliferation |
| TGF-β | Platelets, macrophages, fibroblasts | Collagen synthesis, inflammation modulation |
| EGF | Platelets, saliva | Epithelial cell proliferation/migration |
| VEGF | Macrophages, keratinocytes | Angiogenesis |
| bFGF | Macrophages, mast cells | Fibroblast and endothelial proliferation |
| IGF-1 | Liver, fibroblasts | Collagen synthesis |
Factors That Impair Healing
Local factors:
- Infection (prolongs inflammation, destroys new tissue)
- Poor blood supply / ischemia
- Foreign body or necrotic tissue
- Radiation damage
- Wound tension
Systemic factors:
- Diabetes mellitus (impairs neutrophil function, angiogenesis, collagen synthesis)
- Malnutrition (protein deficiency impairs collagen synthesis; zinc and vitamin C deficiencies specifically impair healing)
- Corticosteroids (suppress inflammation and fibroblast activity)
- Immunosuppression
- Jaundice / renal failure
- Chemotherapy / radiotherapy
- Aging (slower cellular responses throughout all phases)
Abnormal Healing Outcomes
- Hypertrophic scar: Excess collagen deposition within wound boundaries; typically improves over time. Treated with silicone, corticosteroid injection, or compression.
- Keloid: Scar extends beyond original wound margins, may be locally destructive. More common in darker skin types, affects earlobes, deltoid, and presternal region. More resistant to treatment; may need excision plus adjuvant radiotherapy.
- Chronic wound: Healing fails to progress through normal phases (most commonly stuck in inflammation); seen in venous ulcers, diabetic foot ulcers, pressure ulcers.
Sources: Schwartz's Principles of Surgery, 11th ed., Ch. 9 (Wound Healing); Bailey and Love's Short Practice of Surgery, 28th ed., Ch. 47.
This is a shared conversation. Sign in to Orris to start your own chat.