Necrosis - Hinglish mein Samjho! 🧬
Necrosis kya hota hai?
Seedha baat karo toh - Necrosis = Cell ka pathological death (living body mein).
Yeh apoptosis (programmed death) se alag hai - necrosis mein cell accident se marta hai, apoptosis mein suicide karta hai. Aur necrosis ke saath inflammation zaroor aati hai.
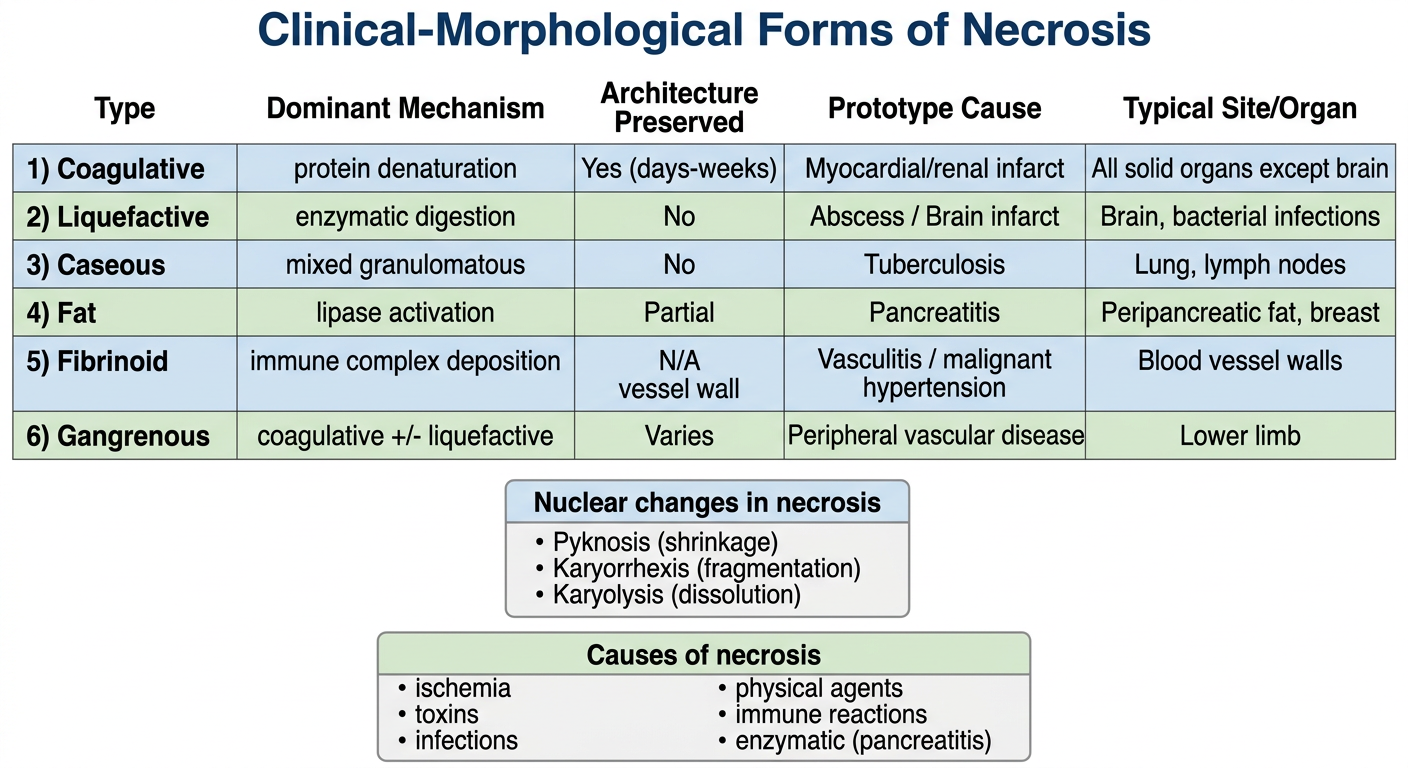
Necrosis Kyun Hota Hai? (Causes)
| Cause | Example |
|---|
| Ischemia (Blood supply band) | Heart attack, thrombosis |
| Physical injury | Burns, radiation, thanda/garmi |
| Chemical/Toxic | Zeher, heavy metals, strong acids |
| Bacteria/Virus ke toxins | Infections |
| Immune reaction | Antigen-antibody complex vessel wall mein |
| Enzymes leak ho jayein | Pancreatitis mein lipase leak |
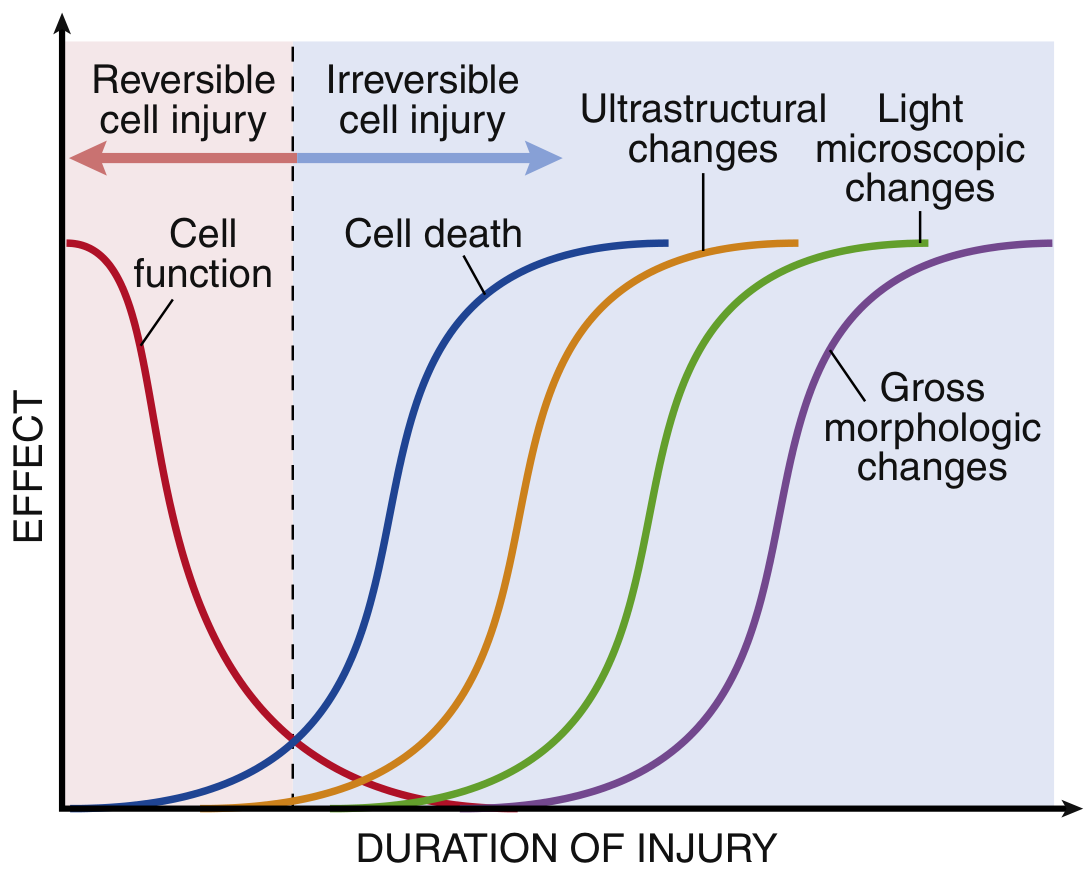
Mechanism kaise hota hai? (Pathogenesis)
Step-by-step samjho:
1. ATP khatam hoti hai (sabse pehle aur sabse important!)
- Na⁺/K⁺ pump band → cell swell karta hai
- Anaerobic glycolysis shuru → lactic acid banta hai → pH girta hai → chromatin clump hota hai
2. Calcium andar ghus aata hai (Ca²⁺ increases)
- Phospholipases activate → membrane digest hone lagti hai
- Proteases activate → proteins toot jaate hain
- Endonucleases activate → DNA toot jaata hai
3. Mitochondria damage hoti hai
- Mitochondrial permeability pore (MPTP) khul jaata hai
- Cytochrome c leak hota hai
- ATP generation permanently band → point of no return
4. Lysosomes phoot jaate hain 💥
- Digestive enzymes cytoplasm mein aa jaate hain
- Cell apne aap ko digest kar leta hai (autolysis)
5. Membrane permanently damage hoti hai
- Cellular contents bahar aa jaate hain (blood mein)
- Troponin, transaminases, LDH → biomarkers ka basis yahi hai!
- Bahar aaye molecules (DAMPs) → inflammation trigger karte hain
Morphology - Microscope mein Kya Dikhta Hai?
Cytoplasm mein changes:
- Eosinophilia badhti hai → cell bright pink dikhta hai H&E mein
- (RNA khatam hoti hai jo blue color deti thi, denatured proteins eosin/red se bind karte hain)
- Glassy appearance → glycogen khatam
- Moth-eaten look → organelles digest ho gayi
Nucleus mein 3 changes (yaad karo teen K):
Pyknosis → Karyorrhexis → Karyolysis
(Shrink) (Fragment) (Dissolve)
- Pyknosis - nucleus sikar jaata hai, bahut dark ho jaata hai
- Karyorrhexis - pyknotic nucleus toot ke fragments ban jaata hai
- Karyolysis - basophilia fade ho jaati hai, nucleus dissolve ho jaata hai (1-2 din mein)
6 Clinical-Morphological Forms - Ek Ek Karke!
1. 🔴 Coagulative Necrosis
Yaad karo: "Architecture bachti hai"
Mechanism: Proteins denature hote hain - structural proteins + enzymes dono. Isliye enzymes kaam nahi kar paate, autolysis nahi hoti.
Microscope mein: Ghost cells dikhte hain - cell ka outline bacha rehta hai, nucleus khatam, eosinophilic
Kahan hoti hai: Ischemia se - brain ke alawa har solid organ mein
- Heart attack (myocardial infarct)
- Kidney infarct
- Spleen infarct
Trick: Coagulative = Cooked egg jaise - shape bachi rehti hai!
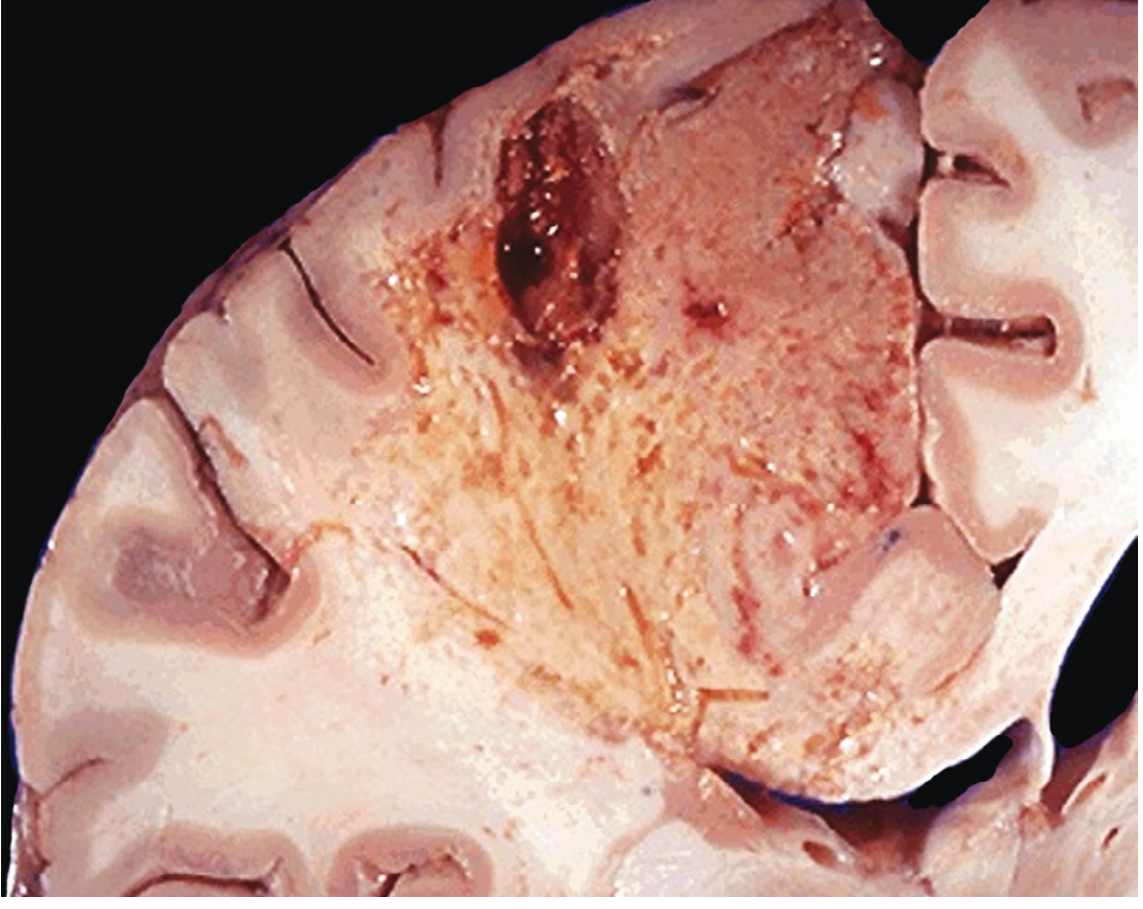
2. 💛 Liquefactive Necrosis
Yaad karo: "Sab kuch liquid ban jaata hai"
Mechanism: Enzymatic digestion dominant hoti hai - leukocytes ke enzymes tissue ko liquid mein convert kar dete hain
Microscope mein: Koi architecture nahi, viscous liquid, agar bacteria hai toh creamy yellow pus
Kahan hoti hai:
- Bacterial/fungal infections → pus banta hai → localized collection = abscess
- Brain ischemia → brain mein coagulative nahi, liquefactive hoti hai (reason unclear)
Trick: Liquefactive = Liquid - bacteria ne sab "pee" liya!
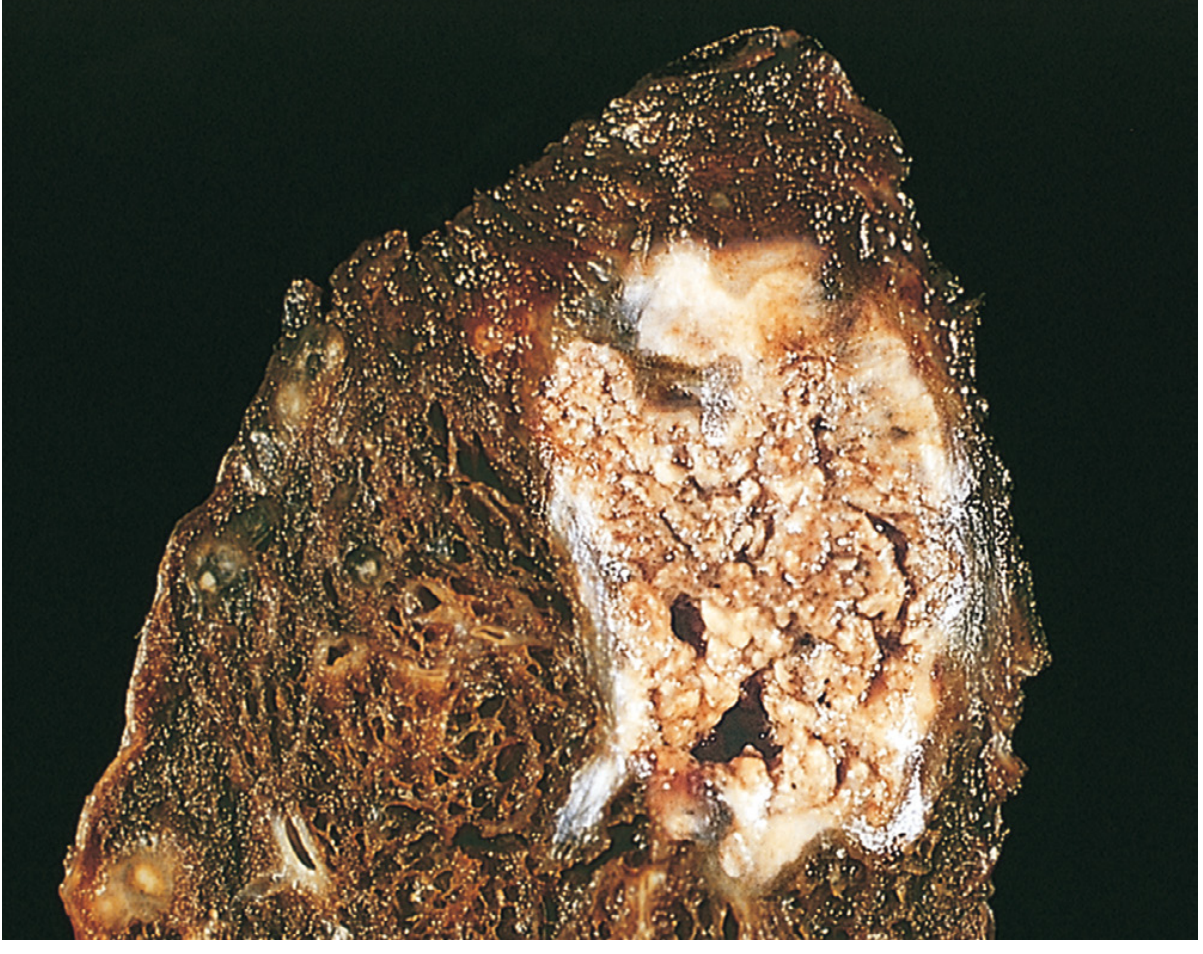
3. 🟡 Caseous Necrosis
Yaad karo: "Cheese jaisi dikhti hai"
Mechanism: Coagulation + liquefaction ka mix, granulomatous inflammation ke saath
Microscope mein:
- Amorphous, granular pink debris - koi cell outline nahi
- Architecture completely khatam
- Surrounded by epithelioid macrophages = granuloma banta hai
Gross appearance: Friable (crumbly), white-yellow, cheese jaisi material
Kahan hoti hai: TB (Tuberculosis) - sabse classic! Aur histoplasmosis
Trick: Caseous = Cheese = TB!
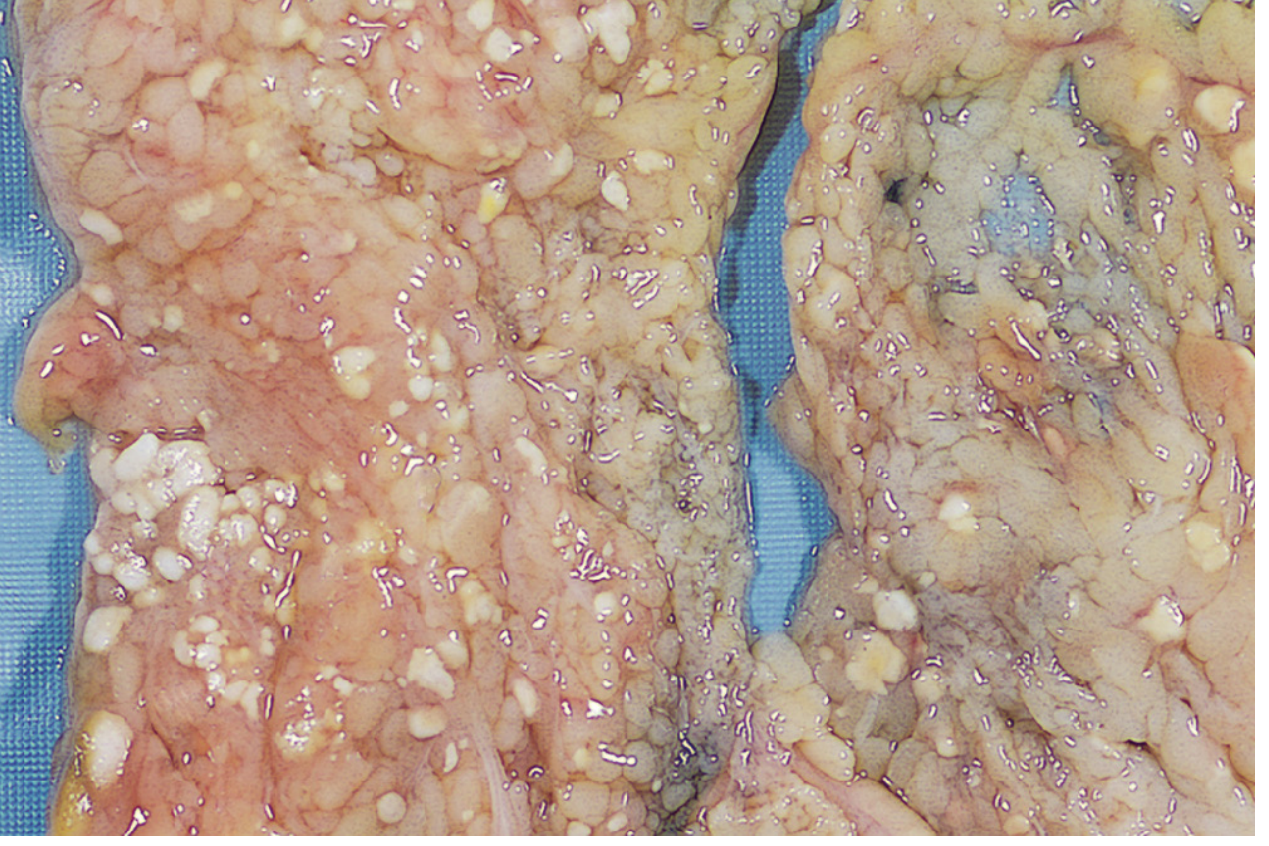
4. ⬜ Fat Necrosis
Yaad karo: "Saponification - soap banta hai"
Mechanism: Lipase enzymes fat cells ke triglycerides ko fatty acids mein convert karte hain → fatty acids + calcium → calcium soaps (saponification)
Microscope mein:
- Necrotic fat cells ke shadowy outlines
- Basophilic (blue) calcium deposits granular form mein
- Surrounding inflammatory reaction
Gross appearance: Chalky white deposits
Kahan hoti hai:
- Acute pancreatitis - pancreatic lipase leak karke peripancreatic fat digest karta hai
- Breast/abdominal trauma
Trick: Fat Necrosis = Fat ko soap banao = Pancreatitis!
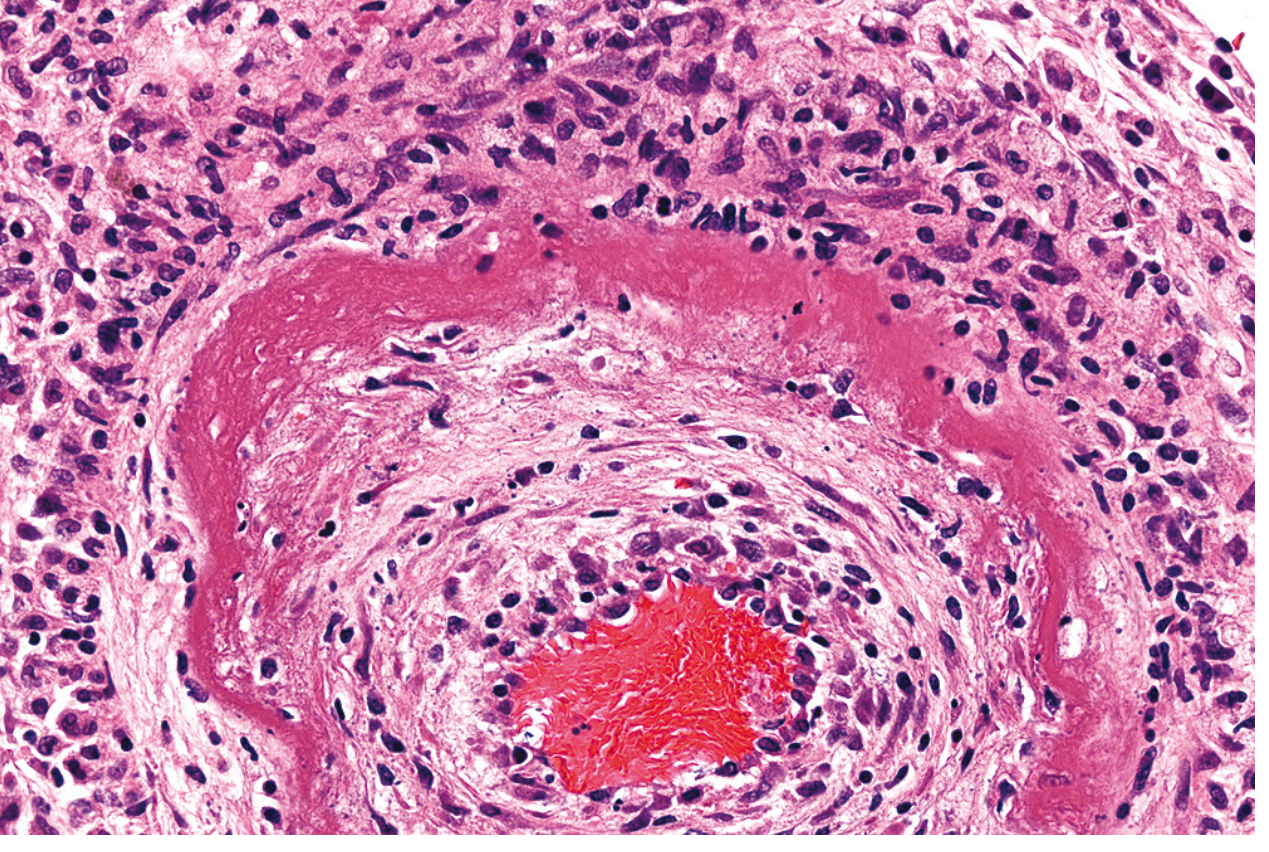
5. 🩷 Fibrinoid Necrosis
Yaad karo: "Sirf microscope mein dikhti hai"
Mechanism: Antigen-antibody complexes vessel wall mein deposit hote hain + plasma proteins leak hote hain → fibrin jaisa material wall mein impregnate ho jaata hai
Microscope mein:
- Bright pink (intensely eosinophilic), amorphous, homogeneous material vessel wall mein
- Circumferential involvement
- Neutrophils surrounding area mein
Gross appearance: Koi distinctive appearance nahi - sirf microscope se detect hoti hai
Kahan hoti hai:
- Vasculitis (immune complex deposition)
- Malignant/severe hypertension
- Organ transplant rejection
Trick: Fibrinoid = Fibrin jaisa pink material = Vessels mein = Vasculitis/HTN!
6. 🖤 Gangrenous Necrosis
Yaad karo: "Clinical term hai, mechanistic nahi"
Yeh ek clinical term hai - mainly lower limb ki ischemia describe karta hai
| Type | Kya hota hai | Appearance |
|---|
| Dry gangrene | Sirf coagulative, koi infection nahi | Dry, dark, mummified, clear boundary |
| Wet gangrene | Coagulative + bacterial infection | Swollen, moist, badbu, unclear boundary |
| Gas gangrene | Clostridium perfringens | Crepitus (gas feel hota hai), rapidly spreading |
Ek Line Summary (Exam ke liye!)
| Form | Cause | Key Feature |
|---|
| Coagulative | Ischemia (brain chhod ke) | Ghost cells, architecture preserved |
| Liquefactive | Bacteria, brain ischemia | Pus, liquid tissue |
| Caseous | TB | Cheese jaisi, granuloma |
| Fat | Pancreatitis | Chalky white, saponification |
| Fibrinoid | Vasculitis, HTN | Bright pink vessel wall |
| Gangrenous | Limb ischemia ± infection | Clinical term, coagulative base |
Clinical Importance - Serum Biomarkers
Necrosis mein cell membrane toot jaati hai → intracellular proteins blood mein aa jaate hain:
- Troponin I/T → Heart cell necrosis (MI) - 2 ghante mein detect hota hai!
- ALT/AST (transaminases) → Liver cell necrosis
- LDH, CK-MB → Various tissue necrosis
- Alkaline phosphatase → Bile duct injury
Yahi reason hai ki blood test se pata chalta hai kaunsa tissue necrotic hua! 🔬
Source: Robbins & Kumar Basic Pathology + Robbins Cotran Pathologic Basis of Disease