I have all the material needed. Here is the complete, exam-ready answer for every question in your list:
Delivery Room Care & Neonatal Management — Complete Answer Set
1. Anticipated Problems in a Preterm Baby & Prevention of Hypothermia
Anticipated Problems in a Preterm Baby
Prematurity creates vulnerability across all organ systems:
| System | Problem |
|---|
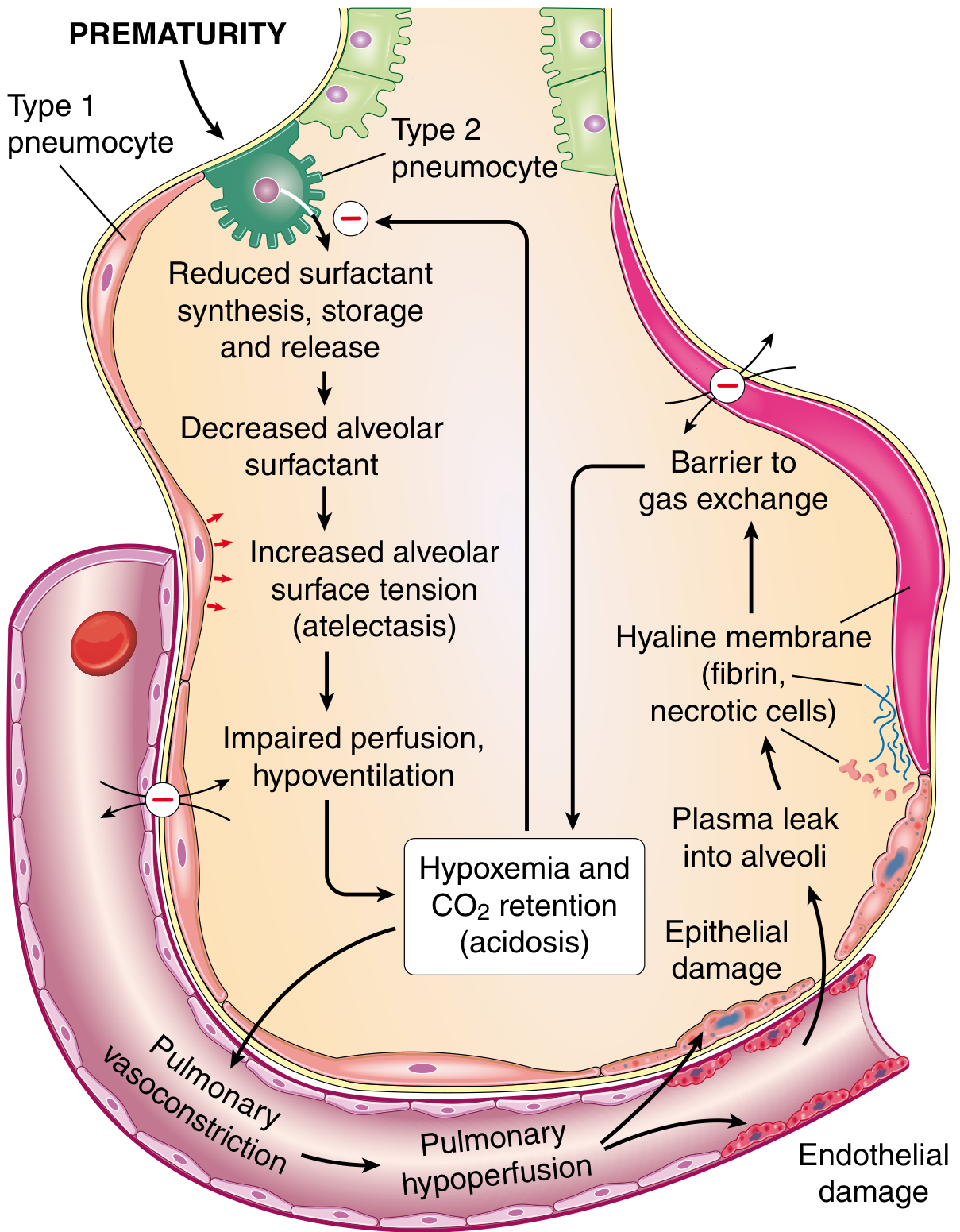
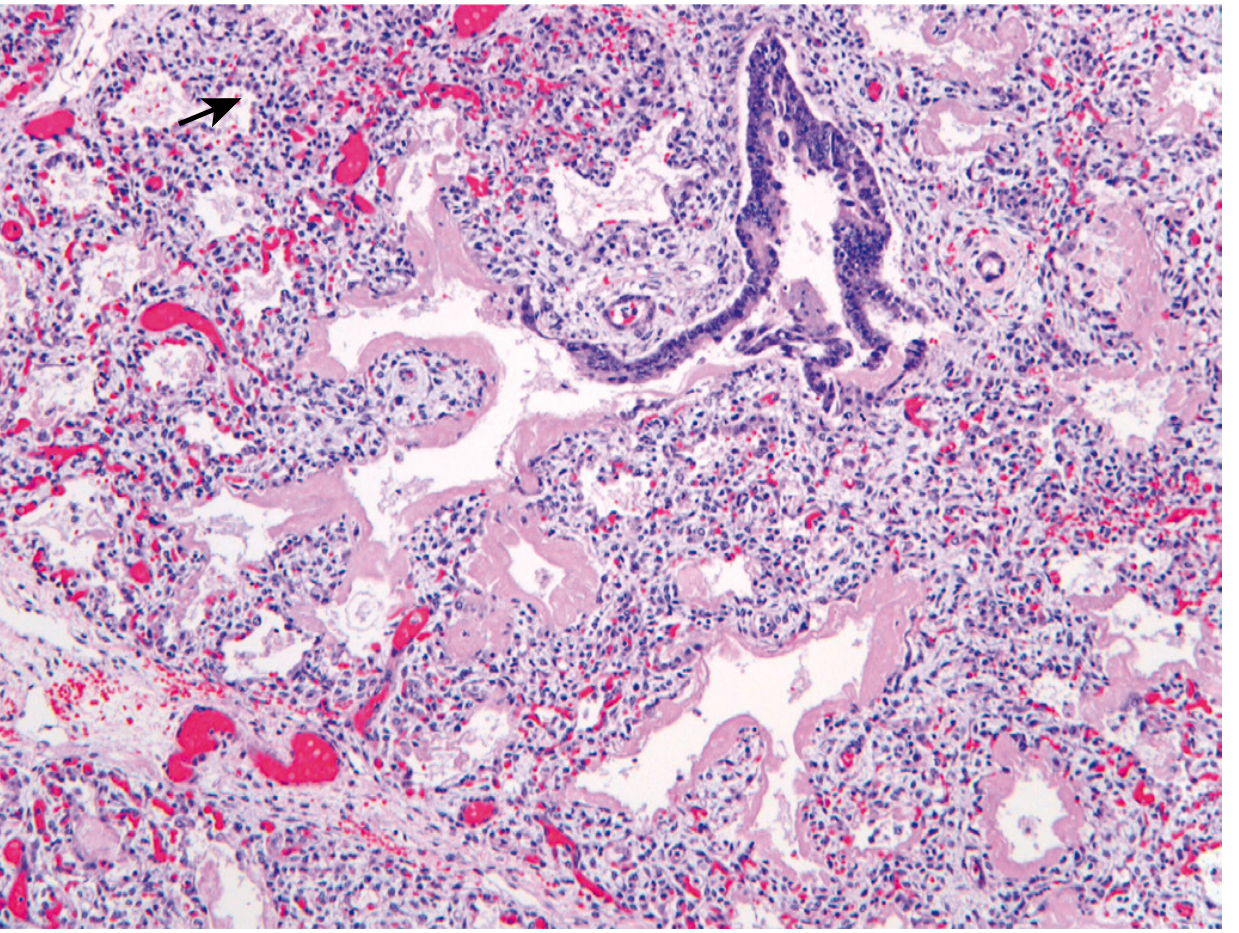
| Respiratory | Hyaline membrane disease (RDS/HMD), apnea of prematurity, bronchopulmonary dysplasia |
| Cardiovascular | Patent ductus arteriosus → left-to-right shunt → pulmonary edema, CCF |
| Neurological | Intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL) |
| Gastrointestinal | Necrotizing enterocolitis (NEC), feeding intolerance, poor suckling reflex |
| Metabolic | Hypothermia, hypoglycemia, hypocalcemia, hyperbilirubinemia |
| Haematological | Anaemia of prematurity, coagulation defects |
| Immune | Increased susceptibility to infection/sepsis |
| Renal | Fluid and electrolyte imbalance |
| Eyes | Retinopathy of prematurity (ROP) |
| Skin | Fragile, permeable skin → increased insensible losses |
Prevention of Hypothermia in a Newborn
The newborn is uniquely susceptible to hypothermia due to:
- Large surface area-to-body mass ratio (especially the head)
- Inability to shiver — can only generate heat via non-shivering thermogenesis in brown fat
- Thin subcutaneous fat — poor thermal insulation
- No behavioral adaptation (cannot change clothing or move away from cold)
- Wet at birth — evaporation is the primary heat loss mechanism immediately after delivery
Measures to Prevent Hypothermia in the Delivery Room
| Measure | Detail |
|---|
| Warm delivery room | Maintain room temperature at 25–28°C |
| Pre-warmed radiant warmer | Switch on before delivery; place infant under warmer immediately after birth |
| Immediate drying | Dry the baby thoroughly with warm towels; remove wet linen immediately |
| Skin-to-skin (Kangaroo care) | For vigorous term infants — place on mother's chest and cover with blanket; very effective |
| Warm blankets/caps | Cover head (large source of heat loss); use pre-warmed blankets |
| Plastic wrap / polyethylene bag | For infants <29 weeks or very low birth weight — place in food-grade polyethylene bag without drying; cover from neck to feet; effective in preventing evaporative heat loss |
| Heated humidified incubator | For VLBW/ELBW infants in NICU |
| Warm IV fluids | IV fluids given at room temperature can cause hypothermia |
| Avoid unnecessary exposure | Minimize examination time; keep covered during procedures |
| Kangaroo Mother Care (KMC) | Continuous skin-to-skin contact with mother — proven to reduce hypothermia in LBW |
Normal axillary temperature in newborn: 36.5°C – 37.5°C
2. Classification of Hypothermia & Management of Severe Hypothermia
Classification of Hypothermia in a Newborn (WHO Classification)
| Category | Axillary Temperature | Features |
|---|
| Cold stress (mild hypothermia) | 36.0°C – 36.4°C | Peripheral vasoconstriction, cool extremities |
| Moderate hypothermia | 32.0°C – 35.9°C | Lethargy, poor feeding, weak cry, pallor |
| Severe hypothermia | < 32°C | Bradycardia, bradypnea, cold to touch all over, poor perfusion, may appear dead |
Management of Severe Hypothermia (< 32°C)
Severe hypothermia is a medical emergency. Management involves rapid rewarming and treating complications simultaneously.
Step-by-step Management:
1. Assess and stabilize
- Check airway, breathing, circulation
- Assess blood glucose immediately (hypoglycemia frequently co-exists)
- Attach cardiac/SpO₂ monitoring
2. Rapid rewarming
- Place under pre-warmed radiant warmer or in a servo-controlled incubator (set at 35–36°C skin temperature)
- Apply warm blankets; warm the room
- Use warm, humidified oxygen if O₂ therapy needed
- Avoid rapid rewarming with water > 38–40°C (risk of burns and cardiovascular instability)
- Target: raise temperature by 0.5–1°C per hour; aim for normothermia (36.5–37.5°C) within 2–6 hours
3. Treat hypoglycemia
- If blood glucose < 40 mg/dL: give IV 10% dextrose (2 mL/kg bolus), then continuous infusion at 80–100 mL/kg/day of D10W
- Monitor glucose every 1–2 hours during rewarming
4. Respiratory support
- Apnea and bradycardia are common in severe hypothermia
- Provide oxygen and PPV/CPAP/ventilation as indicated
5. Manage complications
- Metabolic acidosis → correct with adequate ventilation; sodium bicarbonate only if ventilation is adequate
- Coagulopathy → fresh frozen plasma/platelets as needed
- Sepsis → broad-spectrum antibiotics (ampicillin + gentamicin) if infection suspected
- Fluid and electrolyte imbalance → careful IV fluid management
6. Nutritional support
- Withhold enteral feeds until temperature is ≥ 36°C and baby is stable
- Start IV nutrition early
7. Monitoring
- Temperature every 15–30 minutes during rewarming
- Blood glucose, electrolytes, blood gases
- Avoid hyperthermia during rewarming (can cause apnea and worsen hypoxic-ischemic injury)
3. Apgar Score
The Apgar score is a rapid, standardized clinical assessment tool to evaluate a newborn's condition at birth and response to resuscitation. Introduced by Dr. Virginia Apgar in 1952.
Components (Mnemonic: Appearance, Pulse, Grimace, Activity, Respiration)
| Sign | 0 | 1 | 2 |
|---|
| Appearance (Color) | Blue/pale all over | Pink body, blue extremities (acrocyanosis) | Completely pink |
| Pulse (Heart Rate) | Absent | < 100 beats/min | ≥ 100 beats/min |
| Grimace (Reflex irritability) | No response to stimulation | Grimace | Cough, sneeze, cry |
| Activity (Muscle tone) | Limp | Some flexion of limbs | Active motion, good flexion |
| Respiration | Absent | Weak, irregular, slow | Strong, crying |
Scoring and Interpretation
| Total Score | Interpretation |
|---|
| 7–10 | Normal |
| 4–6 | Moderate depression — may need stimulation and supplemental O₂ |
| 0–3 | Severe depression — immediate resuscitation required |
When to Assess
- 1 minute: Reflects intrauterine/intrapartum status and need for immediate intervention
- 5 minutes: Reflects response to resuscitation; most predictive
- If score < 7 at 5 minutes: repeat every 5 minutes up to 20 minutes
Important Points
- Resuscitation must NOT be delayed to calculate the Apgar score
- Score is influenced by: gestational age (preterm infants score lower), maternal medications, infection, trauma, ongoing resuscitation
- A 5-minute score of 0–3 correlates with increased neonatal mortality
- A low score alone cannot diagnose birth asphyxia or predict neurological outcome
4. Four Basic Needs of a Baby at Birth & How to Provide Them
The four basic needs of every newborn in the delivery room are:
- Warmth
- Clear airway
- Breathing
- Prevention of infection
(Some texts add: Nutrition — initiated by early breastfeeding)
How to Provide These Needs in Routine Care
(a) Warmth
- Warm delivery room (25–28°C)
- Pre-warm radiant warmer/blankets
- Dry immediately after birth; remove wet towels
- Skin-to-skin with mother for vigorous term infants
- Cap on the head; wrap in dry, warm blanket
(b) Clear Airway
- Position: head in neutral position (slight neck extension / "sniffing position")
- Suction mouth first, then nose only if visible secretions or obstruction are present
- Current guidelines: routine suctioning is not recommended for vigorous infants with clear or meconium-stained fluid
- Stimulate breathing by rubbing the back or flicking the soles of the feet (2–3 times)
(c) Breathing
- Assess: breathing? Crying? Good tone? → if yes, routine care
- If not breathing after stimulation: provide positive pressure ventilation (PPV) with bag and mask
- Rate: 40–60 breaths/min; peak inspiratory pressure ~20 cmH₂O
- Start with room air; increase FiO₂ only if SpO₂ targets not met
(d) Prevention of Infection
- Strict aseptic technique at delivery
- Sterile cord clamping and cutting (delayed cord clamping 1–3 min in vigorous infants)
- Eye prophylaxis: 1% tetracycline or 0.5% erythromycin ointment (or 1% silver nitrate drops) — against Neisseria gonorrhoeae and Chlamydia
- Vitamin K₁ 1 mg IM — prevents haemorrhagic disease of the newborn
- Early breastfeeding — provides passive immunity via IgA
- Hepatitis B vaccine + HBIg (if mother HBsAg positive) within 12 hours of birth
5. Delivery Room Care
(a) Requirements for Normal Newborn Care
Every delivery room must have a pre-checked, assembled resuscitation area before delivery.
Equipment Checklist:
| Category | Items |
|---|
| Warmth | Radiant warmer (pre-warmed), warm blankets, plastic wrap/polyethylene bag (for VLBW) |
| Airway | Bulb syringe, suction device (wall suction at ≤100 mmHg), suction catheters (5, 8, 10 Fr) |
| Ventilation | Self-inflating bag (450 mL and 750 mL), flow-inflating bag, masks (premature, newborn, infant sizes), T-piece resuscitator, pressure manometer |
| Intubation | Laryngoscope with straight blades (00, 0, 1), uncuffed ETTs (2.5, 3.0, 3.5, 4.0 mm), stylets, meconium aspirator, CO₂ detector, scissors and tape |
| Circulation | Umbilical catheters (3.5 and 5 Fr), hemostats, sterile drapes, povidone-iodine, scalpel, umbilical tape, three-way stopcock |
| Monitoring | Pulse oximeter, ECG leads, clock/timer |
| PPE | Gown, gloves, eye protection |
| Medications | Epinephrine (1:10,000), normal saline (10 mL/kg for volume), 10% dextrose, surfactant (if anticipated preterm) |
| Other | Stethoscope, cord clamp, Vitamin K₁, eye drops, identification bands |
Personnel required: At least one person present at every delivery whose sole responsibility is care of the newborn. For high-risk deliveries, a full team (paediatrician, nurse, anaesthetist) should be present.
(b) Algorithm for Routine Care of a Normal Newborn
BIRTH
│
▼
Assess: Term gestation? Breathing/crying? Good muscle tone?
│
YES → All three YES
│
▼
ROUTINE CARE (with mother)
• Warm (skin-to-skin with mother or radiant warmer)
• Dry and stimulate
• Delayed cord clamping (1–3 minutes, if vigorous)
• Clear airway ONLY if obstructed (bulb suction, mouth then nose)
• Ongoing assessment every 30 seconds:
– Respiratory effort
– Heart rate
– Colour/SpO₂
│
▼
After 30 seconds: breathing well, HR >100, good tone, colour improving?
│
YES
│
▼
Continue routine care:
• Eye prophylaxis (erythromycin/tetracycline ointment)
• Vitamin K₁ 1 mg IM
• Identification band, weight, head circumference
• Apgar at 1 and 5 minutes
• Encourage early breastfeeding within 1 hour
• Hepatitis B vaccine (within 24 hours)
• Initiate neonatal screening (metabolic screen, hearing screen)
If any of the three initial questions is NO → move to resuscitation algorithm (see next section)
(c) Indications for Artificial Ventilation (Positive Pressure Ventilation — PPV)
Initiate PPV if, after the initial 30-second steps (warm, dry, stimulate, position airway):
| Indication | Detail |
|---|
| Apnea | Infant not breathing at all after stimulation |
| Gasping | Agonal, ineffective respiratory effort |
| Heart rate < 100 beats/min | Bradycardia almost always reflects inadequate ventilation in a neonate |
| Persistent central cyanosis | SpO₂ not meeting targets despite supplemental O₂ |
| Poor respiratory effort | Laboured breathing with retractions + HR < 100 |
Initial settings:
- Rate: 40–60 breaths/min
- Peak inspiratory pressure: ~20 cmH₂O (up to 30–40 cmH₂O for first breaths)
- Start with room air (21% O₂); titrate FiO₂ upward to meet SpO₂ targets
- Place orogastric tube if BMV required for > 2 minutes (prevents gastric distension)
Target SpO₂ goals (preductal — right hand/wrist):
| Time after birth | Target SpO₂ |
|---|
| 1 min | 60–65% |
| 2 min | 65–70% |
| 3 min | 70–75% |
| 4 min | 75–80% |
| 5 min | 80–85% |
| 10 min | 85–90% |
(d) Contraindications for Bag and Mask Ventilation
Bag and mask ventilation (BMV) is the first-line method of PPV, but it is contraindicated or must be replaced by endotracheal intubation in the following situations:
| Contraindication | Reason |
|---|
| Congenital diaphragmatic hernia (CDH) | BMV inflates the stomach/intestines that have herniated into the chest → worsens lung compression; immediate intubation required |
| Tracheo-oesophageal fistula (TOF) | Air enters stomach via fistula, causing regurgitation and aspiration; intubation needed |
| Failed BMV after corrective steps (SOPA: Seal, Opened mouth, Position, Airway cleared; re-adjust) | Requires intubation to secure airway |
| Need for chest compressions | When CPR is started, intubation is recommended to ensure effective ventilation without interruption |
| Extremely premature infants < 25–26 weeks | BMV alone insufficient; intubation + surfactant delivery preferred |
| Choanal atresia | Nasal obstruction prevents effective nasal mask ventilation; oral airway + intubation needed |
| Large omphalocele/gastroschisis | Risk of bowel injury; careful intubation preferred |
| Upper airway obstruction not cleared by suctioning | Obstruction prevents effective ventilation via mask; intubation required |
| Anticipated prolonged ventilation | ETT for sustained mechanical ventilation |
SOPA mnemonic for correcting ineffective BMV before moving to intubation:
- S — re-adjust mask Seal
- O — Open and reposition mouth
- P — reposition head/neck (Positioning)
- A — suction Airway / Alternate airway (ETT)
(e) Drugs Used via the Intratracheal (Endotracheal) Route
In the delivery room, the endotracheal tube may be used to administer medications when IV/IO access has not yet been established.
| Drug | Indication | Intratracheal Dose | Notes |
|---|
| Epinephrine (Adrenaline) | Asystole or persistent bradycardia (HR < 60 bpm) despite effective ventilation + chest compressions | 0.05–0.1 mg/kg (0.5–1 mL/kg of 1:10,000 solution) | IV/IO is preferred; intratracheal dose must be higher than IV dose; flush with 1 mL normal saline after |
| Surfactant (e.g., Poractant alfa, Beractant) | RDS/HMD in preterm infants | Prophylactic or rescue dose per weight (e.g., 100–200 mg/kg for poractant) | Administered via ETT directly into the trachea; INSURE technique (INtubation-SURfactant-Extubation) |
Drugs NO LONGER recommended via intratracheal route:
- Sodium bicarbonate — may worsen intracellular acidosis; not routinely recommended in neonatal resuscitation
- Naloxone — no longer recommended even for maternal opiate exposure; contraindicated if maternal narcotic addiction suspected (risk of seizures)
- Atropine — not recommended in neonatal resuscitation
- Calcium — not given via ETT
Important: IV/IO access (umbilical venous catheter is first choice) should always be sought in preference to the intratracheal route for drug delivery, as intratracheal absorption is unpredictable.
6. Steps of Neonatal Resuscitation (NRP Algorithm)
(a) Steps During the First 30 Seconds
Within the first 30 seconds after birth, perform the following simultaneously:
- Provide warmth — place under pre-warmed radiant warmer
- Dry — dry the baby thoroughly with a warm towel
- Stimulate — rub back vigorously 2–3 times; flick soles of feet
- Position airway — head in neutral/sniffing position (slight neck extension); avoid hyperextension
- Suction — only if airway is visibly obstructed; mouth first, then nose; use bulb syringe or mechanical suction ≤100 mmHg
- Remove wet linen
- Assess at 30 seconds: Is the baby breathing/crying? HR? Tone? Color?
Current NRP guidelines no longer recommend routine suctioning of all newborns, including those born through meconium-stained amniotic fluid who are vigorous.
(b) Indications for Bag and Mask Ventilation
Initiate BMV if, after the initial 30-second steps:
- Apnea — not breathing despite stimulation
- Gasping respirations — agonal breathing
- Heart rate < 100 beats/min — regardless of respiratory effort
- Persistent SpO₂ below targets despite supplemental oxygen
(c) Indications for Initiating Chest Compressions
Chest compressions are started if, despite 30 seconds of effective PPV:
- Heart rate remains < 60 beats/min
Before starting compressions:
- Ensure ventilation is truly effective (chest rise, bilateral breath sounds)
- Switch to 100% O₂
- Intubation is recommended when chest compressions are initiated
Technique:
- Location: lower third of sternum (just below nipple line)
- Depth: one-third of the AP diameter of the chest
- Two methods: two-thumb technique (preferred; encircle chest with fingers) or two-finger technique
- Ratio: 3 compressions : 1 ventilation = 90 compressions + 30 breaths per minute
- Stop compressions when HR > 60 beats/min
(d) Drugs Given Through the Endotracheal Tube
(See section 5e above — same drugs apply)
| Drug | Dose via ETT |
|---|
| Epinephrine | 0.05–0.1 mg/kg (1:10,000 solution) |
| Surfactant | Per weight-based dosing protocol; prophylactic or rescue |
(e) Volume Expanders in the Delivery Room
Indication: Evidence of blood loss / hypovolemia:
- Pallor despite adequate oxygenation
- Weak, rapid pulse
- Poor response to resuscitation (persistent low HR despite adequate ventilation and compressions)
Volume expanders used:
| Agent | Dose | Rate |
|---|
| Normal saline (0.9% NaCl) — first choice | 10 mL/kg IV/IO | Over 5–10 minutes |
| O-negative packed RBCs | 10 mL/kg | Over 5–10 minutes |
| Lactated Ringer's solution | 10 mL/kg | Over 5–10 minutes |
Important cautions:
- Avoid rapid bolus in premature infants → risk of intraventricular hemorrhage
- Higher-volume boluses (20 mL/kg) may be used in full-term infants
- Repeat as needed based on clinical response
- D10W (dextrose) is NOT a volume expander — it is used only for hypoglycemia
7. Low Birth Weight (LBW)
Definition
Low Birth Weight (LBW): Birth weight < 2,500 g regardless of gestational age
| Category | Birth Weight |
|---|
| Low birth weight (LBW) | < 2,500 g |
| Very low birth weight (VLBW) | < 1,500 g |
| Extremely low birth weight (ELBW) | < 1,000 g |
Causes:
- Prematurity (< 37 weeks) — most common in developed countries
- Intrauterine growth restriction (IUGR/FGR) — small for gestational age (SGA)
- Both prematurity + IUGR may coexist
Problems in LBW Neonates
| System | Problem |
|---|
| Thermoregulation | Hypothermia — minimal subcutaneous fat, large SA:volume ratio |
| Respiratory | HMD/RDS, apnoea of prematurity, bronchopulmonary dysplasia |
| Cardiovascular | Patent ductus arteriosus, hypotension, poor peripheral perfusion |
| Neurological | Intraventricular haemorrhage, periventricular leukomalacia, hypoxic-ischaemic encephalopathy |
| Metabolic | Hypoglycaemia (poor glycogen stores), hypocalcaemia, hyponatraemia, metabolic acidosis |
| GI | Necrotizing enterocolitis, poor feeding, gastroesophageal reflux, immature digestive enzymes |
| Haematological | Anaemia, coagulopathy, polycythaemia (in IUGR) |
| Renal | Fluid and electrolyte imbalance, renal tubular dysfunction |
| Immune | Sepsis, meningitis (immature immune system, poor maternal antibody transfer) |
| Jaundice | Hyperbilirubinaemia, kernicterus risk |
| Eyes | Retinopathy of prematurity |
| Long-term | Neurodevelopmental delay, learning difficulties, increased risk of adult metabolic syndrome |
Feeding of LBW Babies
Principles
- LBW infants have high metabolic demands but immature GI tract, poor suck-swallow coordination, small gastric capacity, and risk of aspiration
Feeding Methods (by maturity/stability):
| Gestational age / Weight | Method |
|---|
| < 28–30 weeks or unstable | Parenteral nutrition (PN) as primary; minimal enteral nutrition (MEN) as trophic feeds from day 1–2 if haemodynamically stable |
| 30–34 weeks | Nasogastric (NG) or orogastric (OG) tube feeds; gradually introduce suckling |
| > 34 weeks and vigorous | Direct breastfeeding; cup/spoon feeding; nipple shield if needed |
Preferred Feeds:
- Breast milk — FIRST CHOICE for all LBW infants
- Provides IgA, growth factors, reduces NEC risk significantly
- Fortified breast milk: add human milk fortifier (HMF) for VLBW infants (increases protein, calcium, phosphorus, energy)
- Donor pasteurised human milk — if own mother's milk unavailable (VLBW/ELBW)
- Preterm formula — only if human milk unavailable; higher protein and mineral content than term formula
Feeding Schedule and Volumes:
- Start with trophic/minimal enteral feeds (10–20 mL/kg/day) from day 1–2 to stimulate gut maturation
- Advance by 10–20 mL/kg/day if tolerated
- Full enteral feeds: ~150–180 mL/kg/day
- Feed frequency: every 2–3 hours (8–12 feeds/day)
- Monitor for feed tolerance: gastric residuals, abdominal distension, vomiting, blood in stools (signs of NEC)
Energy Requirements:
- 110–130 kcal/kg/day for VLBW infants
- Protein: 3.5–4.5 g/kg/day (higher than term infants)
- Supplement Vitamin D (400–800 IU/day), Iron (from 2–4 weeks), Folate, Zinc
Sources: Rosen's Emergency Medicine, pp. 3120–3132; Tintinalli's Emergency Medicine, pp. 3780–3857; Textbook of Family Medicine 9e, pp. 526–528; Medical Physiology, pp. 1698–1699; Barash Clinical Anesthesia, p. 3616