Give a long note on herpes simplex virus causing vesicobullous lesion for oral medicine exam final year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have comprehensive content. Now I'll compile a thorough, exam-ready long note on HSV causing vesicobullous lesions in oral medicine.
Herpes Simplex Virus (HSV) Causing Vesicobullous Lesions in the Oral Cavity
A Comprehensive Oral Medicine Note for Final Year Examination
1. INTRODUCTION AND CLASSIFICATION
Herpes simplex virus (HSV) is the most common cause of viral vesicobullous lesions in the oral cavity and oropharynx. It belongs to the family Herpesviridae, subfamily Alphaherpesvirinae, and causes both primary and recurrent infections. Oral and oropharyngeal lesions caused by HSV are the most common virally induced oropharyngeal ulcerative conditions, affecting 60-90% of the population worldwide.
Two serotypes are clinically recognized:
- HSV-1 (HHV-1): Responsible for the vast majority of orofacial disease - primary herpetic gingivostomatitis and herpes labialis
- HSV-2 (HHV-2): Primarily associated with genital infection; rarely causes oral lesions
Oral HSV disease is classified into two major clinical forms:
- Primary Herpetic Gingivostomatitis (PHGS) - the initial infection
- Recurrent/Secondary Herpes Simplex Infection - reactivation of latent virus
- Herpes labialis (cold sores, fever blisters)
- Recurrent intraoral herpes simplex (RIHS)
2. VIROLOGY AND STRUCTURE
HSV consists of:
- A double-stranded DNA (dsDNA) core
- Surrounded by a protein capsid in the three-dimensional form of an icosahedron
- Enclosed within a protein envelope structure that measures approximately 200 nm
- Subclassified into subtypes based on virulence in tissue culture
- HSV-1 and HSV-2 fall within the alpha (α) group of virulence classification (more aggressive viruses fall in β or γ groups)
3. EPIDEMIOLOGY
- Each year in the United States, approximately 600,000 new cases of primary HSV-1 infection develop
- The incidence of primary HSV-1 infection is greatest during childhood, when 30-60% of children are exposed
- Rates of infection increase with age and with reduced socioeconomic status
- Seroprevalence of HSV-1 in the US (2005-2010):
- 30% in persons 14-19 years of age
- 50% in persons 20-29 years of age
- 62% in persons 30-39 years of age
- 20-40% of the population has had episodes of herpes labialis
- The frequency of recurrent episodes averages approximately once per year
- Most HSV-1-infected persons are asymptomatic yet can still transmit the virus
- 12% of oral swabs are positive for HSV by PCR in persons seropositive for HSV-1
4. TRANSMISSION AND SPREAD
- Spread through direct contact with an actively infected individual (primary or recurrent disease)
- Asymptomatic viral shedding within saliva of recovering or previously infected persons is also a source of infection
- Transmission occurs via kissing, shared utensils, or direct mucosal contact
- Recurrent infection originates from reactivation of latent virus in the trigeminal ganglion
5. PATHOGENESIS AND MECHANISM OF VESICLE FORMATION
5a. Initial Infection (Primary Phase)
The mode of oral infection with HSV-1 relates to specific binding of virus to cell surface or plasma membrane receptors, specifically envelope proteins on the virion surface:
- The virus binds to keratinocytes and neurons at specific surface receptors
- Entry into the cytoplasm occurs via endocytosis
- Viral particles migrate through nuclear pores into the nucleoplasm
- Propagation, virus core assembly, and release occur within the nucleus
- A nucleocapsid structure is acquired during this process
- Mature viral particles are transported into the cytoplasm and released through the cell membrane into the extracellular space
- Released virions infect adjacent cells, spreading the lytic infection
How the vesicle forms:
- As viral replication and propagation proceed within keratinocyte nuclei, terminal cytopathic changes develop:
- Nuclear changes (ballooning degeneration, nuclear molding)
- Plasma membrane leakage
- Intracellular metabolic activity ceases
- The cell becomes necrotic and releases large numbers of viral particles into surrounding extracellular space
- This lytic process spreads from cell to cell, producing intraepithelial acantholysis
- Fluid accumulates within the epithelium forming a clinically visible intraepithelial vesicle
5b. Latency Development
- During the primary infection, the virus enters adjacent neurons via surface receptor engagement and endocytosis
- Virus ascends along sensory nerve axons to the trigeminal ganglion (and less commonly nodose/vagal, dorsal root, and sympathetic ganglia)
- Replication occurs within a minority of neurons (4-35% of ganglionic neurons harbor latency-infected cells)
- The immune system suppresses replication and α-gene expression, maintaining the latency state
- A viral RNA reservoir (LAT - latency-associated transcripts) maintains the latency state
5c. Reactivation (Recurrent Disease)
Triggers for reactivation:
- Fever (URI, systemic illness)
- Ultraviolet light (sun exposure)
- Trauma (dental procedures, surgery)
- Stress (emotional, physical)
- Hormonal changes (menstruation)
- Immunosuppression (HIV, corticosteroids, chemotherapy)
- Local trauma
Once reactivated, virus travels from the ganglion back down the sensory nerve to the skin/mucosa, replicating and producing the characteristic vesicular lesion.
6. CLINICAL FEATURES
6a. PRIMARY HERPETIC GINGIVOSTOMATITIS (PHGS)
Definition: The initial infection with HSV-1 (rarely HSV-2) in an individual without prior immunity.
Age of onset: Most commonly in children (6 months to 5 years); less commonly in young adults (primary infection in adults can occur and may be more severe).
Incubation period: Approximately 5-7 days after contact with an infected person.
Prodrome (up to 48 hours):
- Malaise, headache, irritability
- Fever (may be high, 38-40°C)
- Focal mucosal tenderness and erythema
- Cervical lymphadenopathy (submandibular and anterior cervical nodes are enlarged and tender)
- Difficulty eating and swallowing (dysphagia)
Oral manifestations:
- Numerous small, thin-walled vesicles arise on any oral mucosal surface (both keratinized and non-keratinized)
- Vesicles are short-lived (rupture within hours) - leaving shallow, painful, discrete superficial ulcerations
- Each ulcer is surrounded by an inflammatory (erythematous) halo
- Ulcers may coalesce to form larger irregular erosions
- The gingiva is a key diagnostic site: appears erythematous, boggy, and tender, with discrete involvement of the free gingival margin - this is a hallmark of PHGS
- The infection can extend to the oropharynx and occasionally to perioral skin
- Any mucosal surface may be involved: lips, buccal mucosa, tongue, hard and soft palate, floor of mouth
Duration: 7-14 days; self-limiting course. Viral shedding can continue for several weeks after clinical resolution.


6b. RECURRENT HERPES SIMPLEX INFECTION
I. Herpes Labialis (Cold Sore / Fever Blister)
- The most common clinical form of recurrent HSV-1 disease
- Prevalence: 40-60% of those with HSV-1 immunity experience labial recurrences; 58-61% suffer recurrences every 1-4 months
- Site of predilection: The vermilion border of the lip (skin-vermilion junction), consistently recurring at the same site
Clinical stages:
| Stage | Features | Duration |
|---|---|---|
| Prodrome | Focal tingling, burning, pruritus, or altered sensation at the site | Hours before vesicles |
| Erythema | Focal erythema and edema at prodromal site | Hours |
| Papule | Small raised papule(s) | 1-2 days |
| Vesicle | Pinhead-sized, clustered vesicles on erythematous/edematous base; coalesce | 24-48 hours |
| Ulcer/Crust | Vesicles rupture, forming tender ulcerations, then crusting | 5-7 days |
| Healing | Heals without scarring (immunocompetent); scarring in immunosuppressed | Complete resolution |
II. Recurrent Intraoral Herpes Simplex (RIHS)
- Occurs almost exclusively on keratinized epithelium - a key distinguishing feature from primary disease
- Sites of predilection:
- Hard palate (along distribution of the greater palatine nerve, especially first molar-premolar area)
- Attached gingiva (mandibular molar-premolar area and maxillary gingiva)
- Dorsal tongue surface (less commonly)
- Distribution: Usually unilateral, does not cross the midline; follows nerve distribution
- Presents as multiple, shallow, closely cropped tender erosions and ulcerations
- Distinguished from PHGS in that lesions are confined to keratinized mucosa only
7. HISTOPATHOLOGY
7a. Vesicle Formation (Key Microscopic Features)
- Intraepithelial vesicle - the vesicle forms within the epithelium (not subepithelial as in pemphigoid)
- The vesicle is filled with:
- Serous fluid (serum)
- Free-floating, virally infected keratinocytes
- Inflammatory cells (neutrophils, lymphocytes)
- Intense, focal, mixed inflammatory infiltrate surrounds the vesicle
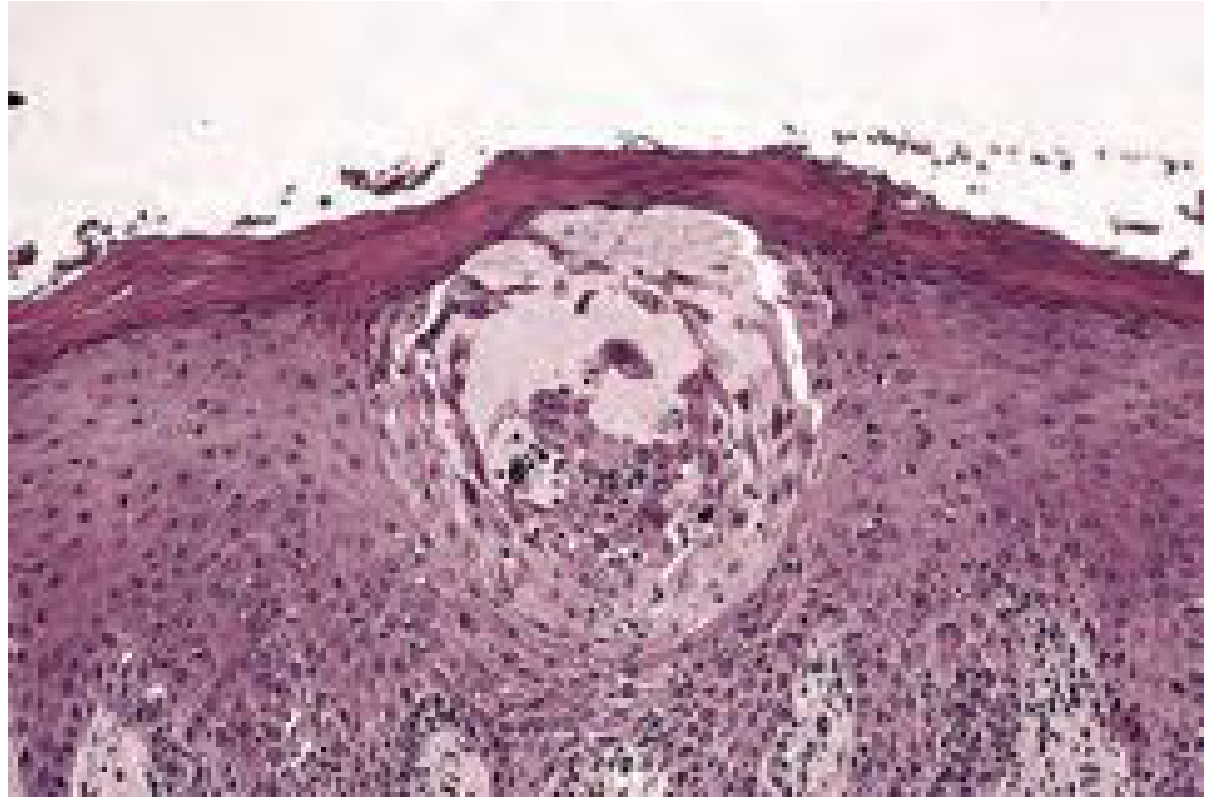
7b. Characteristic Cytopathic Changes (Viral Cytopathic Effect - VCPE)
- Ballooning degeneration - enlargement and swelling of infected epithelial cells
- Acantholysis - loss of intercellular attachments leading to free-floating cells (Tzanck cells)
- Multinucleated giant cells (syncytia) - fusion of adjacent virally-infected cells; nuclei are molded together
- Intranuclear eosinophilic inclusion bodies (Cowdry Type A inclusions) - eosinophilic inclusion bodies separated from the nuclear membrane by a clear halo; represent viral particles within the nucleus
- Nuclear molding - nuclei pushed together at their margins, "ground-glass" appearance
- Reticular degeneration - vesicle formation due to ballooning and rupture of individual cells
8. DIAGNOSTIC INVESTIGATIONS
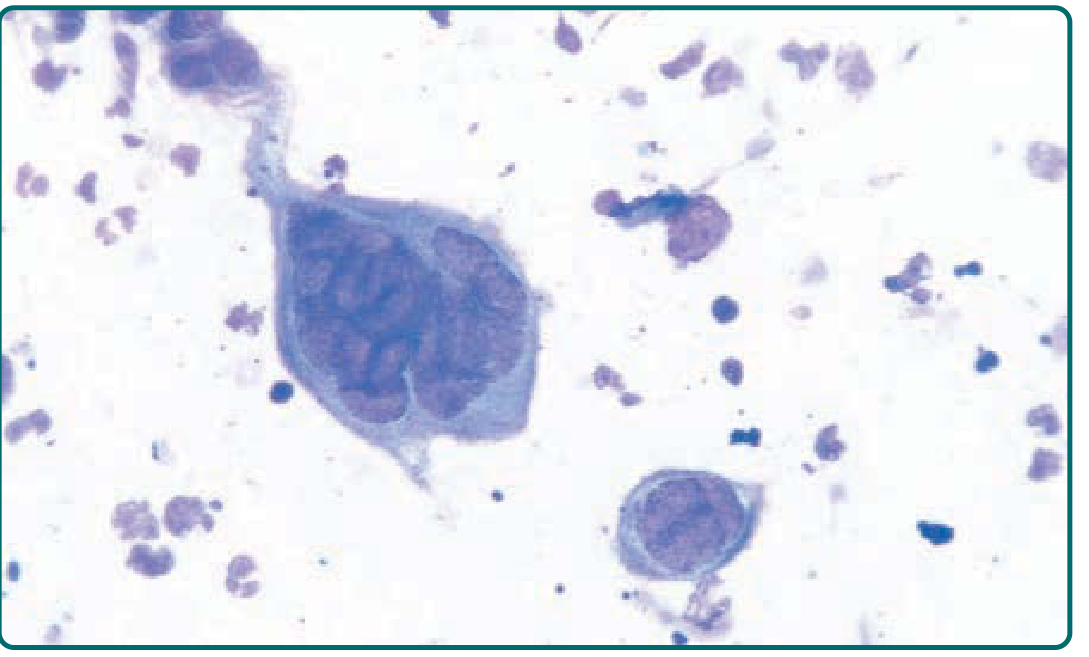
8a. Tzanck Smear (Cytology) - MOST IMPORTANT RAPID TEST
Procedure:
- Unroof a freshly ruptured vesicle
- Scrape the base of the vesicle with a scalpel blade
- Smear material onto a glass slide
- Stain with Giemsa stain (or Wright stain or Papanicolaou stain)
- Examine under microscope
Positive findings:
- Multinucleated giant cells (Tzanck cells) - diagnostic of herpetic infection
- Ballooned, swollen epithelial cells
Important note: The Tzanck test is helpful for rapid diagnosis but is less sensitive than viral culture - positive in fewer than 40% of culture-proven cases. It cannot differentiate between HSV and VZV (both cause identical Tzanck changes).
8b. Viral Culture (Gold Standard)
- Swab of vesicle fluid or base of fresh ulcer
- Most sensitive for active lesions
- Takes 24-72 hours; limited in recurrent mild disease
8c. Polymerase Chain Reaction (PCR)
- Highly sensitive and specific
- Can detect and type HSV-1 vs HSV-2
- Method of choice for CSF analysis (encephalitis)
8d. Direct Fluorescent Antibody (DFA) Test
- Staining of lesion scrapings with fluorescent-labeled antibodies
- Good sensitivity, faster than culture
- Can differentiate HSV-1, HSV-2, and VZV
8e. Serology (Antibody Titers)
- HSV-specific IgG and IgM
- Seroconversion (IgM in primary; fourfold rise in IgG in recurrent)
- Useful for retrospective diagnosis
- Type-specific serology: gG-1 and gG-2 antibodies
- Not ideal for acute lesion diagnosis
| Serology Pattern | HSV-1 IgG (acute) | HSV-1 IgG (convalescent) |
|---|---|---|
| Primary HSV-1 | Negative | Positive |
| Recurrent HSV-1 | Positive | Positive (stable or rising) |
8f. Biopsy and Histopathology
- Intraepithelial vesicle with Cowdry Type A inclusions, multinucleated giant cells, ballooning degeneration
- Useful when clinical diagnosis is uncertain
- Immunohistochemistry with anti-HSV antibodies confirms diagnosis
9. DIFFERENTIAL DIAGNOSIS
For Primary Herpetic Gingivostomatitis:
| Condition | Key Distinguishing Features |
|---|---|
| Herpangina (Coxsackievirus A) | Vesicles confined to soft palate/uvula/tonsillar pillars; no gingival involvement |
| Hand-Foot-Mouth Disease (Coxsackievirus A16) | Oral lesions + exanthem on palms, soles, buttocks |
| Chickenpox/Varicella (VZV) | Diffuse cutaneous vesicular rash; oral lesions milder |
| Erythema Multiforme | "Target" skin lesions; hemorrhagic lip crusting; usually no gingival vesiculation |
| Aphthous Stomatitis | No systemic symptoms, no gingival involvement, no prodrome, no vesicle stage |
| Measles (Koplik spots) | Small white papules/ulcers on buccal mucosa; associated rash, Koplik spots pathognomonic |
| Pemphigus Vulgaris | Chronic condition in older adults; flaccid bullae, Nikolsky sign positive; Tzanck shows acantholytic cells without viral changes |
For Recurrent Herpes Labialis:
- Aphthous ulcers (on non-keratinized mucosa; no vesicle stage)
- Angular cheilosis
- Contact sensitivity dermatitis
- Perioral dermatitis (traumatized)
- Primary syphilis (indurated painless ulcer)
- Erythema multiforme
10. MANAGEMENT AND TREATMENT
10a. Primary Herpetic Gingivostomatitis
General principles: Management is primarily symptomatic and supportive as the patient develops antibodies. However, early antiviral therapy can reduce severity and duration.
Supportive measures:
- Adequate hydration (IV fluids if severe dehydration in children)
- Rest
- Soft, bland diet; avoid acidic/spicy foods
- Analgesics: Paracetamol/ibuprofen for pain and fever
- Topical anesthetics (viscous lidocaine, benzocaine) for mucosal pain relief
- Mouth rinses: Chlorhexidine gluconate 0.2% for secondary infection prevention
- Good oral hygiene (gentle tooth brushing)
Antiviral therapy:
- Acyclovir (Aciclovir): Drug of choice
- Mechanism: Nucleoside analogue - inhibits viral DNA polymerase after activation by viral thymidine kinase
- Dose (adults): 200-400 mg 5 times daily for 5-7 days
- Dose (children): 20 mg/kg (max 400 mg) 4 times daily for 5 days
- Intravenous for severe/immunocompromised cases: 5-10 mg/kg every 8 hours
- Valacyclovir: Prodrug of acyclovir; better oral bioavailability; 1 g BD for 7-10 days
- Famciclovir: Prodrug of penciclovir; alternative option
Key clinical note: Antiviral therapy is most effective when initiated within 72 hours of symptom onset (during the prodrome or early vesicular stage).
10b. Recurrent Herpes Labialis
Immunocompetent patients: Generally does not require systemic antivirals for isolated labial recurrences.
Topical agents:
- Penciclovir cream (1%): Applied every 2 hours while awake; inhibits HHV-1 DNA polymerase
- Docosanol cream (10%): Saturated 22-carbon primary alcohol; prevents viral envelope-keratinocyte plasma membrane fusion - blocks viral entry; first FDA-approved OTC antiviral
- Acyclovir cream (5%): Modest benefit only
- Topical foscarnet, cidofovir, or imiquimod: For recalcitrant cases
Systemic antivirals (for frequent or severe recurrences):
- Acyclovir 400 mg 5 times/day for 5 days (episodic)
- Valacyclovir 2 g twice daily for 1 day (pulse/single-day therapy)
- Famciclovir 1500 mg as a single dose
Suppressive therapy (for very frequent recurrences, e.g., >6/year):
- Acyclovir 400 mg BD daily (long-term suppression)
- Valacyclovir 500 mg once daily
10c. Recurrent Intraoral Herpes Simplex
- Similar to herpes labialis management
- Topical antivirals applied early in prodrome
- Systemic antivirals for immunocompromised patients
10d. Immunocompromised Patients (HIV, transplant recipients, etc.)
- More severe, atypical, and prolonged lesions
- Systemic acyclovir or valacyclovir required
- IV acyclovir for severe/disseminated disease
- Acyclovir-resistant HSV (thymidine kinase-deficient mutants): Treat with foscarnet (IV, 40 mg/kg every 8 hours)
- Suppressive antiviral therapy should be considered for recurrent episodes
11. COMPLICATIONS AND SPECIAL SITUATIONS
11a. Erythema Multiforme (EM) Association
- Recurrent HSV infection is the most common precipitating event in cases of recurrent erythema multiforme
- HSV-associated EM is acute, self-limited, and recurrent (lasting ~3 weeks)
- Lesions are symmetric, on acral extremities and face; mucosal involvement restricted to the mouth
- Management: Suppressive antiviral therapy (acyclovir at sub-therapeutic doses has reduced further EM episodes)
11b. Eczema Herpeticum (Kaposi Varicelliform Eruption)
- Widespread cutaneous HSV infection in patients with atopic dermatitis or other skin barrier disruptions
- Life-threatening in severe cases
- Requires systemic acyclovir
11c. Herpetic Whitlow
- HSV infection of the finger/nail fold
- Relevant to dental professionals (occupational hazard from contact with patient oral secretions)
- Prevention: Use of gloves during dental procedures
11d. Ocular Herpes
- HSV keratoconjunctivitis, stromal keratitis
- Leading cause of corneal blindness from recurrent episodes
- Treatment: Topical trifluridine + systemic acyclovir
11e. Neonatal Herpes
- Acquired perinatally from mother with genital HSV infection
- Risk of transmission: 25-50% for primary maternal infection (vaginal delivery)
- Three forms: SEM (skin-eye-mouth), CNS/encephalitic, disseminated
- Without therapy, mortality is 65%
- Treatment: IV acyclovir 60 mg/kg/day in 3 divided doses for 14-21 days, followed by oral suppression for 6 months
11f. HSV Encephalitis
- Rare but most common cause of fatal sporadic viral encephalitis
- Predominantly temporal lobe involvement
- Treated with IV acyclovir 10 mg/kg every 8 hours for 14-21 days
12. KEY DIFFERENCES: PRIMARY vs. RECURRENT ORAL HSV
| Feature | Primary PHGS | Recurrent (Labialis/RIHS) |
|---|---|---|
| First occurrence | Yes (no prior immunity) | No (prior HSV immunity) |
| Age | Usually children; young adults | Any age |
| Systemic features | Prominent (fever, malaise, lymphadenopathy) | Absent (prodrome only) |
| Oral mucosa affected | Keratinized AND non-keratinized | Keratinized only (RIHS); vermilion/lip (labialis) |
| Gingival involvement | Characteristic - erythematous, boggy | Only if on attached gingiva (RIHS) |
| Distribution | Diffuse, widespread | Localized, clustered, same site |
| Vesicle size | Small, thin-walled | Small, clustered, coalesce |
| Duration | 7-14 days | 7-10 days |
| Scarring | No (immunocompetent) | No (immunocompetent) |
| Serology | Seroconversion (IgM, then IgG) | Pre-existing IgG; modest rise |
| Antiviral benefit | High (if started early) | Moderate (shortens by 1-2 days) |
13. SUMMARY TABLE: HSV VESICOBULLOUS LESION AT A GLANCE
| Parameter | Details |
|---|---|
| Causative agent | HSV-1 (mainly), HSV-2 (rarely orally) |
| Virus type | Double-stranded DNA, icosahedral capsid, 200 nm |
| Virus family | Herpesviridae, Alphaherpesvirinae |
| Vesicle type | Intraepithelial (not subepithelial) |
| Mechanism | Ballooning degeneration + acantholysis → vesicle formation |
| Key histology | Intraepithelial vesicle, Cowdry Type A inclusions, multinucleated giant cells |
| Tzanck smear | Multinucleated giant cells (Giemsa/Wright stain) |
| Latency site | Trigeminal ganglion (dorsal root ganglion) |
| Key drug | Acyclovir (nucleoside analogue) |
| Drug mechanism | Viral thymidine kinase activation → inhibits viral DNA polymerase |
| Topical agents | Penciclovir cream, Docosanol cream |
| Resistance treatment | Foscarnet (IV) |
14. IMPORTANT EXAM POINTS TO REMEMBER
- Intraepithelial vesicle - in contrast to pemphigoid (subepithelial) and pemphigus (suprabasilar acantholysis without Cowdry inclusions)
- Cowdry Type A intranuclear inclusions - eosinophilic, with clear halo, in both HSV and VZV
- Tzanck smear cannot differentiate HSV from VZV - both show multinucleated giant cells
- Recurrent intraoral HSV occurs only on keratinized mucosa - hard palate and attached gingiva; aphthous ulcers occur on non-keratinized mucosa
- Gingival involvement is pathognomonic of primary PHGS - recurrent aphthous stomatitis does NOT involve the gingiva
- Herpes labialis recurs at the same site (vermilion border) due to the nerve distribution from the latency ganglion
- Docosanol acts by preventing viral envelope-cell membrane fusion (unlike nucleoside analogues)
- Foscarnet is used for acyclovir-resistant HSV - does not require activation by viral thymidine kinase
- HSV is the most common trigger for erythema multiforme - recurrent EM should prompt investigation for HSV
- Asymptomatic shedding is clinically significant for transmission even without visible lesions
Sources: Cummings Otolaryngology Head and Neck Surgery (Oral Disease section); Fitzpatrick's Dermatology Vol. 1&2 (Chapter 164: Herpes Simplex); Goldman-Cecil Medicine (Viral Oral Ulcers); Tintinalli's Emergency Medicine (HSV Infections)
This is a shared conversation. Sign in to Orris to start your own chat.